
Abstract
Abstract
Heart failure (HF) affects ∼600,000 Canadians and is a chronic, life-limiting illness marked by exacerbations of distressing symptoms requiring acute medical management, typically sought in Canada's emergency departments. HF often has an unpredictable illness trajectory and is a chronic terminal illness with a poor prognosis. Patients living with advanced HF have difficulty in accessing palliative care (PC) supports, which can result in unnecessary suffering as their HF progresses and they near end of life (EOL). This is, in part, due to a lack of research, helping clinicians to identify patients who are approaching EOL. In addition, the unpredictable nature of illness progression often precludes access to most EOL resources in our current prognosis-dependent healthcare system. PC teams focus on optimizing quality of life through symptom management and ensure that care plans are congruent with patient and family preferences. A PC team was embedded into our institution's existing HF team. Findings show that integration of an embedded model of PC delivery for patients living with advanced HF led to overwhelming positive patient and family feedback while providing timely advance care planning discussions that may be associated with beneficial patient, family, and system outcomes. These outcomes can be used to inform public policy and speak to a cost-effective patient and family-centered approach for providing care to individuals and families living with advanced HF.
Introduction
H
Patients living with advanced HF often have difficulty in accessing palliative care (PC) supports, which can result in unnecessary suffering at end of life (EOL). This is, in part, due to a lack of research, helping clinicians to identify patients who are approaching EOL. In addition, the unpredictable nature of the illness progression often precludes access to most EOL resources in our current prognosis-dependent healthcare system. The 2014 Ontario provincial Auditor General's report found that current PC resources are mostly accessed by patients living with cancer; this report called for education, training, and care standards to improve the delivery of PC for patients with noncancer diagnoses. 6
There is limited research to date describing PC and advanced HF program integration. However, early results suggest associations between PC involvement and improved symptom burden, lower rates of depression, and improved QoL in both the outpatient and inpatient settings.7,8
Our institution is a 450-bed community academic hospital in suburban Toronto, Ontario. Our HF clinic currently serves ∼3500 patients per year through a multidisciplinary team including cardiologists, nurse practitioners, a registered nurse, a registered dietician, and pharmacists. The clinic's goal is to prevent avoidable ED visits and admissions to hospital for patients with advanced HF through close longitudinal follow-up care in the ambulatory setting. The clinic defines advanced HF patients as having class III or IV New York Heart Association symptoms requiring chronic intermittent use of intravenous medications for management of symptoms.
Despite the clinic's existence, many patients require inpatient admission for symptom management, especially as their advanced HF progresses into its final stages. PC, when sought, typically occurs late in the illness trajectory during an acute exacerbation and often in the patient's final days or weeks of life. 9 Emerging evidence suggests that two hospitalizations within the same year for treatment of HF exacerbations portend a high risk of death within the next 12 months. 10 As such, there is an opportunity to help facilitate illness understanding, prognostic awareness, and discussions about goals of care that are consistent with patient and family preferences earlier in the illness. These are key competencies of PC teams, which act as an added layer of support to patients and their families living with advanced serious illness. 11 Current consensus guidelines and general recommendations advocate for PC integration for this patient population.12–14
The focus of any PC team is to optimize QoL through expert-level symptom management while ensuring that treatment is aligned with patient/family goals. Assistance in navigating a complex healthcare system and advance care planning (ACP) are key aspects of high-quality PC. In addition to general discussions about appointing a substitute decision maker and goals for EOL care, complex decision making that is unique to HF includes discussions centering on preferences for device therapy (e.g., implantable cardioverter-defibrillator, left ventricular assist device therapy) and deactivation of devices and inotrope infusion, which can alter the EOL trajectory. Moreover, patients with HF can experience sudden cardiac death, making ACP even more important at earlier stages of the illness and throughout the illness as it progresses into its final stages. Goodlin's state-of-the-art review describes a comprehensive care model to address these issues for HF patients throughout its stages. 15 The cardiac team at our institution cited lack of communication skills and lack of time as barriers to engaging in ACP.
PC teams have specialized training in communication skills that can assist with these discussions. ACP has been associated with choosing less aggressive medical interventions at EOL, making earlier referrals to comfort-focused care near time of death, 16 allowing families the time needed to prepare both emotionally and practically for the possibility of their loved one's death, 17 care delivery that is more concordant with patient wishes, and increased satisfaction with care received. 18 Given the chronic, relapsing, and unpredictable HF course, PC teams are well situated to provide early and regular ACP discussions, ensuring treatments still align with goals as the illness advances into its final stages.
At our institution, PC consults for our cardiac population were requested in the hours and days before a patient's death. Earlier PC introduction for patients living with cancer has been shown to improve symptom control and optimize QoL while at the same time helping patients live longer. 19 We wanted to investigate how earlier PC involvement affected ACP, resource utilization, and the healthcare experience for our patients and their families. A PC team was embedded into our institution's existing HF team, and patients who were likely to be in their last year of life were systematically identified to receive PC. We present our findings in this article.
Methods
Setting
In early 2014, the cardiology and PC teams met to engage in an educational exchange and to conduct a needs assessment for our advanced HF population. In July 2014, we launched an innovative “Supportive Cardiology” service, which embedded a PC team into the existing multidisciplinary HF team.
Patients
Intervention group
We reviewed HF guidelines from Canada, the United States, and the United Kingdom to help identify patient needs that might benefit from PC consultation. Informal conversations with HF multidisciplinary team members at our institution also informed patient referral criteria. Patients with advanced HF and a likely unmet PC need were defined as having the following: New York Heart Association class III or IV symptoms with one or more ED visits, or two or more hospital admissions for treatment of their HF in the prior six months. Patients also needed to have multiple comorbidities or a prior intensive care unit admission or to have received cardiopulmonary resuscitation within the prior 12 months (Table 1). Patients interested in transplant or mechanical circulatory support devices and patients who had a prior PC consult were excluded. Patients meeting these referral criteria, which are listed in Table 1, made up our intervention group.
COPD, chronic obstructive pulmonary disease; CPR, cardiopulmonary resuscitation; CRF, chronic renal failure; CVA, cerebrovascular accident; DM, diabetes mellitus; IPF, interstitial pulmonary fibrosis; NYHA, New York Heart Association; HF, heart failure; ICU, intensive care unit.
Control group
Patients who met referral criteria to be seen by the PC team during admission for treatment of HF exacerbation but for whom the attending cardiologist did not approve PC consultation comprised our control group.
Study design
This is a nonrandomized prospective study comparing outcomes over a six-month study period for patients receiving PC, in addition to standard cardiac care versus standard cardiac care alone. Research ethics board approval was obtained from our institution, and patients provided informed written consent.
Study flow
Our clinical nurse specialist met weekly with the cardiac team to identify eligible patients from the inpatient setting. The patient's primary cardiologist was asked to agree to the PC team consultation and follow-up care. Eligible patients who agreed to a PC consult and whose cardiologist also agreed to PC consultation received an inpatient PC consult during an admission for treatment of HF exacerbation. Patients and their families were given an information guide that was developed by our PC and HF teams to assist with the following: describing how PC may be helpful in the management of advanced HF, describing basic HF symptom management, providing prognostic education, explaining the importance of ACP, and providing a telephone number to be used post-discharge for nonemergency support. The guide was developed with the intention that it would travel with patients from home to their appointments, thereby helping to ensure consistent delivery of information by clinicians in multiple settings. Participants' need for ongoing PC was assessed, and follow-up care was arranged.
An additional component of our intervention included referral to a community-based PC nurse practitioner who provided 24/7 symptom management support. This nurse practitioner liaised with the patient's cardiologist and family physician to help manage advanced HF in the home setting. It is important to note that to our knowledge, no formalized national hospice program exists in Canada. Instead, variable inter-professional, community-based PC teams are available in most regions. Access is typically prognosis based (e.g., patients who you would not be surprised if they die within the next year), need based (e.g., having symptoms requiring nursing management) and is carried out in the patient's home. More services are available in the last month of life.
The PC outpatient team comprised two PC-trained physicians, a PC clinical nurse specialist, a part-time social worker, and a pharmacist. The PC team saw patients Monday through Friday between 8 AM and 5 PM and was colocated within the hospital's already existing HF clinic. Most PC visits occurred immediately after the HF team assessed the patient during a routine cardiac visit. Same-day appointments were always attempted. Patients could book separate appointments with the PC team, though joint visits were encouraged.
Outcomes
The primary outcome was documentation of ACP, which was defined as a patient's consultation or progress note documenting code status as “do not resuscitate” (DNR), “full code,” or “not documented.”
Secondary outcomes were acute care utilization, which was defined as the number of ED visits or hospital admissions for treatment of HF exacerbation throughout the study period, and patient/family satisfaction with PC received. Satisfaction was assessed by patient and family responses to interview questions asked by our research coordinator 48 hours and 6 months after index hospital discharge, which marked the study completion. Key words frequently used by respondents were categorized into themes. Provider satisfaction was assessed informally through conversations and e-mail exchange at the end of the study. Direct provider reports have been included in quotations in this article.
A medical resident completed a chart review for the purpose of comparing pre-/post-data outcomes. Only information obtained from our hospital's electronic medical record was used. Demographic information, laboratory investigations, and diuretic dose reflect data at the time of initial consultation. Documentation of ACP and acute care utilization was obtained in two ways: first, a retrospective one-year review before the patient's enrolment in the study and second, a follow-up prospective review six months after enrolling in the study.
Statistical analysis
Statistical analyses were evaluated by using SPSS (version 20.0) General Linear Model software using the Greenhouse-Geisser correction, which also included eta-squared effect sizes (η2), where: (1) 0.02–0.12 = small, (2) 0.13–0.25 = medium, and (3) ≥0.26 = large. Repeated-measures analysis of variance (ANOVA) tested Group (Intervention, Control) × Time (Pre-Treatment, Post-Treatment) interactions.
Results
Participants
Forty patients participated in our study. Demographic data are presented in Table 2. The intervention and control groups were similar in terms of age, gender, and daily furosemide dosing. Eighty percent of patients (n = 16) in the intervention group compared with 27% (n = 4) in the control group died during the study period.
BNP, brain natriuretic peptide.
Twenty patients comprised our intervention group and received PC, in addition to routine cardiac care through our embedded model (see Fig. 1). All patients in the intervention group received inpatient PC consultation. Three of these patients died during their hospitalization, and three were discharged to receive EOL care in a PC unit. The remaining 14 patients were discharged to long-term care (n = 6) or home with community-based PC (n = 8). All patients in the intervention group who were discharged to long-term care or home were referred to follow-up with outpatient PC. Nine out of the 14 (64%) patients received outpatient PC, with an average of 4.5 visits (range 1–12 visits) per patient throughout the study period. The majority of patients (7 out of 9, 78%) received same-day joint visits with the PC and HF teams. Only two patients requested an outpatient PC visit on a different day than their scheduled HF appointment.
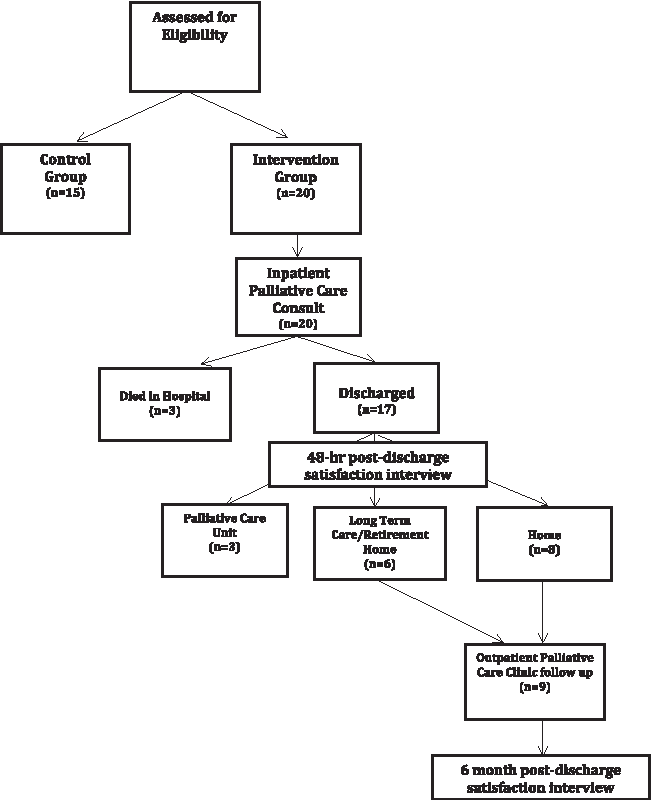
Study flow diagram.
The other 20 patients were part of our control group. Five of the 20 control group patients were referred for inpatient PC consultation during the study period. This disqualified them from the control group, and their post-study enrollment data were not collected for analysis. Thus, 15 patients comprised our control group. We tested whether there were differences between the 5 participants who were disqualified from the control group and the 15 participants who comprised our final control group to account for potential bias. No significant between-group differences emerged when examining baseline ED utilization (t(18) = 1.75, p = 0.10) and hospital admissions (t(18) = 0.43, p = 0.67).
Although not formally measured, reasons that the cardiologists provided for not approving PC consultation included: patients not dying and, therefore, not yet needing PC (e.g., equating PC to care of the imminently dying), and a cardiologist's subjective feeling of still being able to offer more disease-modifying therapies (e.g., misunderstanding of ability to offer PC and cardiac care simultaneously).
Advance care planning
There was no baseline difference between intervention and control group ACP documentation (χ 2 (1, n = 35) = 0.68, p = 0.41). However, there was an increase in ACP documentation for the intervention group throughout the study period (χ 2 (1, n = 35) = 21.39, p < 0.001). ACP increased from 40% to 100% for patients in the intervention group (Table 3). More patients in the intervention group elected DNR code status after receiving PC consultation (30% pre vs. 80% post). ACP documentation did not change throughout the study period for the control group. Only 5 out of 15 charts (33%) had a documented code status, and only 1 of these patients elected DNR code status.
ACP, advance care planning; DNR, do not resuscitate; ED, emergency department; pts, patients.
Acute care utilization
When examining ED visits, we conducted a Group (Intervention, Control) × Time (Pre-Treatment, Post-Treatment) repeated-measures ANOVA. No Group × Time interaction emerged, F(1,33) = 1.29, p = 0.27. Interestingly, there was a main effect for Time, F(1,33) = 18.57, p < 0.001, suggesting that across groups there was a general decrease in ED utilization throughout the study period. The main effect for Group was nonsignificant, F(1,33) = 0.95, p = 0.34. Given the preliminary nature of the study, post hoc effects for the nonsignificant interaction were decomposed for within- and between-group effects. Within-group analyses revealed that both the intervention (p < 0.001, η 2 = 0.34) and control (p = 0.04, η 2 = 0.12) groups showed reduced ED visits from pre- to post-treatment. For the between-group effects, importantly there were no differences in ED visits at baseline (p = 0.92, η 2 = 0.00); however, post-treatment, the intervention group showed significantly fewer ED visits relative to the control group at a trend level (p = 0.067, η 2 = 0.10).
For hospital admissions, we also conducted a Group (Intervention, Control) × Time (Pre-Treatment, Post-Treatment) repeated-measures ANOVA. No Group × Time interaction emerged, F(1,33) = 0.15, p = 0.70; however, across participants, there was a main effect for Time, F(1,33) = 43.39, p < 0.001, indicating a general decrease in hospital admissions throughout the study period. The main effect for Group was nonsignificant, F(1,33) = 1.22, p = 0.27. Similar to our approach with ED utilization, we also probed our nonsignificant interaction. Within-group analyses revealed that the intervention (p < 0.001, η 2 = 0.46) and control (p = 0.04, η 2 = 0.34) groups showed reduced hospital admissions from pre- to post-treatment. No between-group effects emerged for pre- (p = 0.64, η 2 = 0.01) or post-treatment (p = 0.14, η 2 = 0.06).
Community referrals
All patients in the intervention group who were discharged to either long-term care or home were referred to a community-based PC program. None of the patients in the control group were referred to a community-based PC program.
Satisfaction with palliative care
Patients and their families reported overwhelming high satisfaction with PC involvement, as evidenced by responses to structured questions asked by our research coordinator. One hundred percent of patients and their families appreciated having PC involved in their or their loved one's care at 48 hours and 6 months post-discharge from index hospitalization. Sixty-three percent of patients and their families reported a change in how they thought about their illness. Based on the frequency of qualitative responses to interview questions, our research coordinator identified four themes reflecting common patient and family experiences: PC acting as an added layer of support, PC assisting with illness understanding and ACP, appreciation of PC's holistic approach to care, and PC's assistance in navigating the healthcare system (Table 4). One family member of a patient seen in the intervention group wrote, “The work of the team was invaluable to me as I dealt with the new reality of the state of my dad's health. Without the PC team I would not have been successful in navigating the system of community-based supports and I strongly believe that without their work, my father would have deteriorated by now.”
CCAC, which offers provincial home-based services including physical therapy, occupational therapy, and nursing, based on need.
CCAC, Community Care Access Centre; PC, palliative care.
Both the PC clinicians and the cardiology team's qualitative feedback were also positive. A cardiology nurse practitioner reported that her experience of working with the PC team was very helpful: “Their expertise in symptom management and ACP has improved quality of care and filled a gap that existed in our program. They are making a world of difference in the lives of patients and families.” A family physician stated that he appreciated “being part of a team that is working together to help my patient achieve their goals.” Finally, a cardiologist who worked alongside the PC team observed that “as our patients age and develop multiple morbidities, we realize that cardiologists alone cannot deal with EOL and symptom management. Our PC team has become invaluable in managing these patients and reassuring their families. It's my belief that they are an essential limb of any HF clinic team.”
Interpretation
Earlier integration of PC for patients with advanced HF using an embedded inpatient and colocated outpatient model led to increased ACP, positive patient, family, and provider experiences, and a trend toward reduced acute care utilization at EOL. A key challenge to providing PC for this patient population is the unpredictability of the illness course. Moreover, some of our cardiology colleagues still felt that PC is appropriate only for the imminently dying or that it can only be offered after disease-modifying therapies have been stopped and are no longer providing benefits near EOL. By reviewing available HF guidelines, we were able to systematically identify patients who were likely to benefit from earlier PC involvement based on need and not prognosis. This removed some of the unpredictability associated with a typical HF trajectory. This also allowed us to have greater buy-in from cardiology clinicians since recognized experts in their field created these recommendations.
All patients receiving an inpatient PC consultation and discharged home were referred to a community-based PC program that was designed to assist patients and their families in understanding treatments, adhering to medication regimens, and managing symptoms at home by using both oral and intravenous diuretics. Partnering with a community-based team that was capable of providing 24/7 symptom support allowed real-time care that may have led to the trend to a decrease in the acute care utilization observed in our intervention group.
Our embedded inpatient and colocated outpatient clinical model acts on recommendations made in the most recent Ontario Auditor General's report, including: building public awareness and education around PC, better system integration, building common processes that enable clinicians to easily identify patients who would likely benefit from PC, and assisting patients living with end-stage illness to access PC support. 6
Moreover, the Ontario Medical Association recently reported that only 20% of Canadians are aware of the term “ACP” and advocated for increased public awareness on this issue. 20 Our intervention demonstrated that earlier and longitudinal PC integration for patients with advanced HF led to a substantial increase in ACP. We believe that this increase was correlated with both the longitudinal nature of our intervention and the information guide used as well. The ability to provide longitudinal care across settings afforded time to cultivate trust between the PC team, the HF team, and patients and their families.
Patients were given an information guide that further helped them to develop better illness understanding and facilitated increased prognostic awareness, which we believe helped to inform EOL decisions. The information guide was used in the hospital, outpatient clinic, and the patient's home, thereby helping to ensure consistent delivery of information in multiple settings. We also believe that this educational material helped to normalize sensitive EOL discussions, decreased the common stigma and fear surrounding PC, and created a safe space for these discussions to occur. Patients reported that the information guide helped them to better understand their HF and associated symptoms, and it acted as an aid to more effectively navigate the healthcare system. Coming to terms with one's mortality is a process that occurs over time. The longitudinal nature of our program, combined with the information guide's benefits described earlier, likely correlated with the higher rates of ACP and the trend to lower acute care utilization at EOL for patients receiving PC intervention.
One interesting outcome is that many more patients in the intervention group died during the study period compared with the control group (80% vs. 20%). Given the requirement for the patient's cardiologist to agree to a collaborative model of care with the PC team, it may be that the cardiologist's “gestalt” view held unique prognostic value. To explain further, informally we heard cardiologists state, “the patient is not yet palliative” or “it's not yet time to involve palliative care, there is more I can still do for this patient.” This highlights a gap in understanding that PC can be offered at any stage of any advanced serious illness, and that PC can be offered at the same time as disease-modifying care. It may be that cardiologists were more likely to approve the PC consult if they felt their patient was closer to EOL. In addition, our study took place over a short period of time and introduced a shared model of care requiring behavioral changes. The adoption of changes with any resulting system improvements is likely to take time. Additional research is needed in this area.
The embedded design of the program allowed for improved collaboration between HF and PC teams, breaking down current fragmented or siloed models of care. This also created a more patient-centered approach to care by providing same-day and same-location appointments for patients and their families. Joint visits allowed the cardiology teams to better understand the scope of PC providers who are often perceived as providing care to the imminently dying. The availability of real-time support to the cardiology team also facilitated an interdisciplinary approach to managing complex illness. This collaboration occurred in the outpatient HF clinic when the cardiology team urgently required PC consultation for symptom management, as well as through tele-home support and during inpatient hospitalizations. There was a progressive shift in thinking about PC from “is this patient dying?” to “how can the PC team help this patient to have enhanced QoL?” As joint patient visits become the standard of care in our clinical model, we are observing that collaborative care allows patients and their families to better appreciate the added layer of support required to optimize care delivery for patients with advanced HF.
Several limitations exist for our study. First, our sample size was small. Future studies should track symptom and quality metrics for larger numbers of patients to better demonstrate the impact of PC for this patient population. Second, our clinic was initially staffed to accommodate patients one half-day per week. Our early experiences demonstrated that this model would not meet the needs of all patients since some presented to the clinic unexpectedly with acute symptoms requiring urgent attention. Due to staffing limitations, we could not attend to all urgent patient needs and our findings might be strengthened if increased staffing was available. Future studies are needed to inform appropriate staffing ratios. Third, a large number of patients in the intervention group died during the study period. Since these patients were ineligible for readmission, the reporting of cumulative incidence of hospital utilization outcomes is limited. Also, an electronic medical record that only captures data for our institution limited us in understanding healthcare usage outside our hospital, which may have biased the results. In addition, there may have been bias in the way the qualitative data were obtained and analyzed, as we did not use either validated satisfaction or qualitative analysis tools. Future studies could consider incorporating validated measures into the study design to better understand the benefits of PC integration for this patient population. Finally, these data come from a single institution and may not be generalizable across settings.
To our knowledge, our program is a first-of-its-kind program in the country and has demonstrated the benefits of systematically identifying patients with advanced HF who may benefit from earlier PC delivery. PC offered concurrently with routine cardiac care is now the standard of care for HF patients at our institution. A trend toward a reduction in unwanted acute care utilization based on patient and family preferences at EOL, coupled with associated lower costs, warrants further study and carries implications to inform public policy as we plan for the best interests of an aging population.
Footnotes
Acknowledgments
The authors acknowledge Richard Hoang and Krista Margeson for their assistance with literature search and data entry. They are grateful to Shana Haberman for her incredible assistance with project coordination and gentle patient care.
Author Disclosure Statement
No competing financial interests exist.