
Abstract
Abstract
Background:
Strong opioids are a cornerstone of pain treatment, of which morphine is considered an essential analgesic by the World Health Organization. Access to opioids is limited, due to restrictive laws, limited education, and high prices. This is the second phase of a global project to monitor and report the dispensing price of opioids with the specific aim to expand and increase the information and allow further analysis of the challenges in their availability and affordability.
Method:
Participants were asked to provide the lowest dispensing price of the smallest selling unit and lowest strength of five opioids in 13 formulations from a licensed pharmacy located closest to a public facility that provides diagnosis/treatment for life-threatening conditions. Data were collected from July 2015 to March 2016. Average availability, median (Me), and interquartile range (IQR) price were calculated for four gross national income (GNI) categories: higher income countries (HIC), upper middle income countries (UMIC), low middle income countries (LMIC), and low income countries (LIC). Affordability for one month of treatment with morphine immediate release (IR) tablet was also calculated.
Results:
Data were submitted by 67 participants from 43 countries. Availability is strongly related to GNI level (Kruskal–Wallis tests p < 0.0001). Mean price for morphine IR tablets for a 30-day treatment within the GNI categories ranged between USD 3.28 and 376; average USD 78.5 (SD = 92, Me = 49.7, IQR = 80.5). Methadone oral liquid and hydromorphone slow release were the lowest priced (Me = 13.1, IQR = 70 and Me = 14.9, IQR = 89.1, respectively). Morphine IR tablet is less affordable in countries in lower income groups: LIC (mean = 54.1 ± 0.873, Me = 54.1); LMIC (mean = 21.1 ± 19.6, Me = 10.6); UMIC (mean = 14.1 ± 14.1, Me = 10.23); and HIC (mean = 3.2 ± 5.2, Me = 1.33). A negative correlation between the number of days and the countries' income category (Rs = −0.7; p < 0.001) was identified.
Conclusion:
Patients in LIC and MIC have less access to opioid medications. This highlights the need to continue efforts at improving access, availability, and affordability.
Background
A
In 2016, the United Nations General Assembly Special Session (UNGASS) adopted a resolution highlighting the need to enhance national efforts and international cooperation at all levels…promoting measures to ensure their availability and accessibility for medical and scientific purposes. 4 Still in many countries limited or no access is a significant problem. Low and middle income countries (LMIC) with about 80% of the world population account for 6% of the global morphine consumption. 5 Regions as North America, western and central Europe, and Oceania have shown some increase, but use remains very inadequate in Central America and the Caribbean, Africa, and South Asia, or inadequate in East and South-East Asia and Eastern Europe. 6
Access to opioids is limited due to several reasons, including restrictive drug control laws and regulations, lack of education, and high prices.7,8 In LMIC, they have been reported to be more expensive than in high income countries (HIC),9–13 and prices in small cities and rural areas are higher than in large cities. 14
WHO and Health Action International (HAI) developed a method to monitor and report the price of essential medicines as a measure of access, 15 which has prompted some governments to lower the cost of medicines. 16 However, with one exception of a study that includes morphine, 17 the WHO/HAI surveys do not include opioids and there is limited information on their price and affordability.
In 2012, the International Association for Hospice and Palliative Care (IAHPC) initiated the Opioid Price Watch (OPW), a project to monitor and report the dispensing price of opioids around the world. This project is part of IAHPC's formal collaboration with the WHO. 18
During 2014, IAHPC implemented a pilot to test the OPW. The results and main findings were published, 13 and the reports of the dispensing prices were uploaded in a special OPW section and a map in the IAHPC website. The report presented data on availability, dispensing prices, and affordability submitted by 30 participants from 26 countries.
This article presents the data collected for the second phase of the OPW, following the similar methodology and process of the pilot project.
The objectives of OPW second phase are to expand and increase the information collected from the first phase and allow further analysis of the challenges in the availability and affordability of opioid analgesics.
Methods
The same medications and formulations included in the pilot study were included in this second phase
13
:
• Fentanyl [transdermal patch (TP)] • Hydromorphone [injectable, oral solid immediate release (IR), oral solid slow release (SR), and oral liquid] • Methadone (oral liquid and oral solid) • Morphine [injectable, tablet (IR and SR), and liquid], and • Oxycodone (oral solid IR and SR)
These opioids were selected as they were included in the 19th edition of the WHO Model List of Essential Medicines (EML) 2 or in the IAHPC List of Essential Medicines 19 or in the International Narcotics Control Board (INCB) reports on opioid consumption by member states. 20 Excluded from the study were formulations that require special delivery technology and/or skills, such as pumps and blockages.
Participants for the data collection of the second phase of OPW were recruited in several ways: by personal contact during the World Congress of Palliative Care in Copenhagen (May 2015), through an open invitation sent through the IAHPC Newsletter and the IAHPC social media (Facebook and twitter), and by sending a public announcement through the IAHPC list-serve.
Participants were informed of the objectives of the study, the total estimated time to complete the survey, that their names would be acknowledged, and that the data presented would be linked to their city and country. A signed informed consent was submitted by the participants before completing the survey. They were offered guidance and support during the collection period by a coauthor (Ebtesam Ahmed).
Participants were first asked if none of the opioids included in the study was available at any time in their country (never available). If yes, they were asked to select that option and submit the survey. Otherwise, they were asked to identify a public health facility (hospital) that provides diagnostic and treatment services for patients with life-threatening conditions. Then, they were asked to select the closest pharmacy to this facility—may be a licensed retail pharmacy or it may be a pharmacy located inside the facility (“hospital pharmacy”) that dispenses opioids to outpatients. IAHPC provided a letter to the participants addressed to the chief pharmacist confirming they were participating in the study and requesting the pharmacist's collaboration in providing the information for the study. If the chief pharmacist agreed, participants first inquired if at least one of the opioids included in the study was available. If yes, they were asked to provide the lowest dispensing price of the smallest selling unit of the lowest strength of each medication/formulation available. If any medication was available free of charge this was also recorded. Pharmacy address was recorded to avoid potential duplication. If the pharmacy did not have any of the opioids available included in the study, participants were asked to go to the closest pharmacy until they found a pharmacy where at least one opioid was available.
The survey was submitted through the IAHPC server. Participants who completed the reports were given three months of free membership to the IAHPC with full benefits.
Data were collected from July 2015 to March 2016 and reported in the local currency. Prices were automatically converted to US Dollars (USD) based on the corresponding day's exchange rate. 21
Data analysis
Survey results were exported to Microsoft Excel and analyzed using IBM SPSS Statistics. Descriptive analysis and bivariate analysis were conducted. Spearman's rank correlation (Rs), Kruskal–Wallis tests, and Wilcoxon test were used when applicable. A 30-day treatment dose for each medication was calculated using the Defined Daily Dose (DDD) for each medication and is described in Table 1.22,23 The price for the 30-day treatment was calculated by dividing the price of the package/bottle by the total mgs in each and then multiplying the resulting price per mg by the corresponding monthly DDD from the above. 15
Given that there is no identified DDD for pain treatment with methadone, a morphine equivalent (Meq) dose was defined as 1:5 based on the published literature: (100 mg/5 = 20 mg).
DDD, defined daily dose.
The average availability, median (Me), and interquartile range (IQR) price of each medication were calculated for each gross national income (GNI) region. 24 Spearman's rank correlation between availability and opioid consumption was calculated. 25 Opioid consumption data were collected from the Pain and Policy Studies Group (PPSG), a WHO Collaborating Center recognized as a reliable source of information on global consumption of opioids. 26
Calculations did not include medications dispensed for free.
Two additional calculations specific for morphine IR tablet were done: (1) affordability (number of working days needed by the lowest skilled worker to pay for one 30-day treatment) 15 was calculated using the country's minimum wage 27 and the reported dispensed price of the medication and (2) ratio between the dispensed price and the international reference price of morphine IR tablet. As per the International Drug Price Indicator, the 2014 international reference price was USD 0.93 for one morphine IR 10 mg tablet. 28
As in the first phase, the study was designed utilizing, whenever applicable, the checklist for cross-sectional studies of the Strengthening the Reporting of Observational Studies in Epidemiology. 29 Appendix 1 includes the definitions applied. An ethics review board from the Fundacion Federacion Medica de Buenos Aires in Argentina approved the study.
Results
Data were submitted by 67 participants from 43 countries. The list of participants is included in the Acknowledgment section. We received reports from more than one location in 13 countries: India (5), Kenya, and México (4); Brazil, Lithuania, Poland, and Portugal (3); and Bangladesh, Costa Rica, Egypt, Guatemala, Moldova, and Uganda (2). To facilitate distinction between different reports from the same country, the specific location is presented in brackets after the country's name.
All the reports were from large or medium urban centers. Twenty participants were from 14 HIC (17.9% of HIC), 17 from 11 UMIC (20% of UMIC), 24 from 13 LMIC (25% of LMIC), and 6 from 5 LIC (16.1% of LIC).
Availability
None of the participants replied yes to the question about opioids never being available in their countries. However, three participants reported that no opioids were available in any of the pharmacies they visited [(Albania, Benin, and Guatemala (Antigua)] on the day they collected the information.
The average number of pharmacies visited before finding one that had at least one opioid included in the study was 1.1 (SD = 2.0; Me = 0) and varied by GNI: HIC: 0.4 (SD = 0.7; range = 0–2), UMIC: 0.7 (SD = 1.5; range = 0–5), LMIC: 1.6 (SD = 2.6; range = 0–9), and LIC: 2.8 (SD = 6.0; range = 0–15). Figure 1 represents the number of pharmacies visited before finding one that had opioids available distributed in GNI categories.
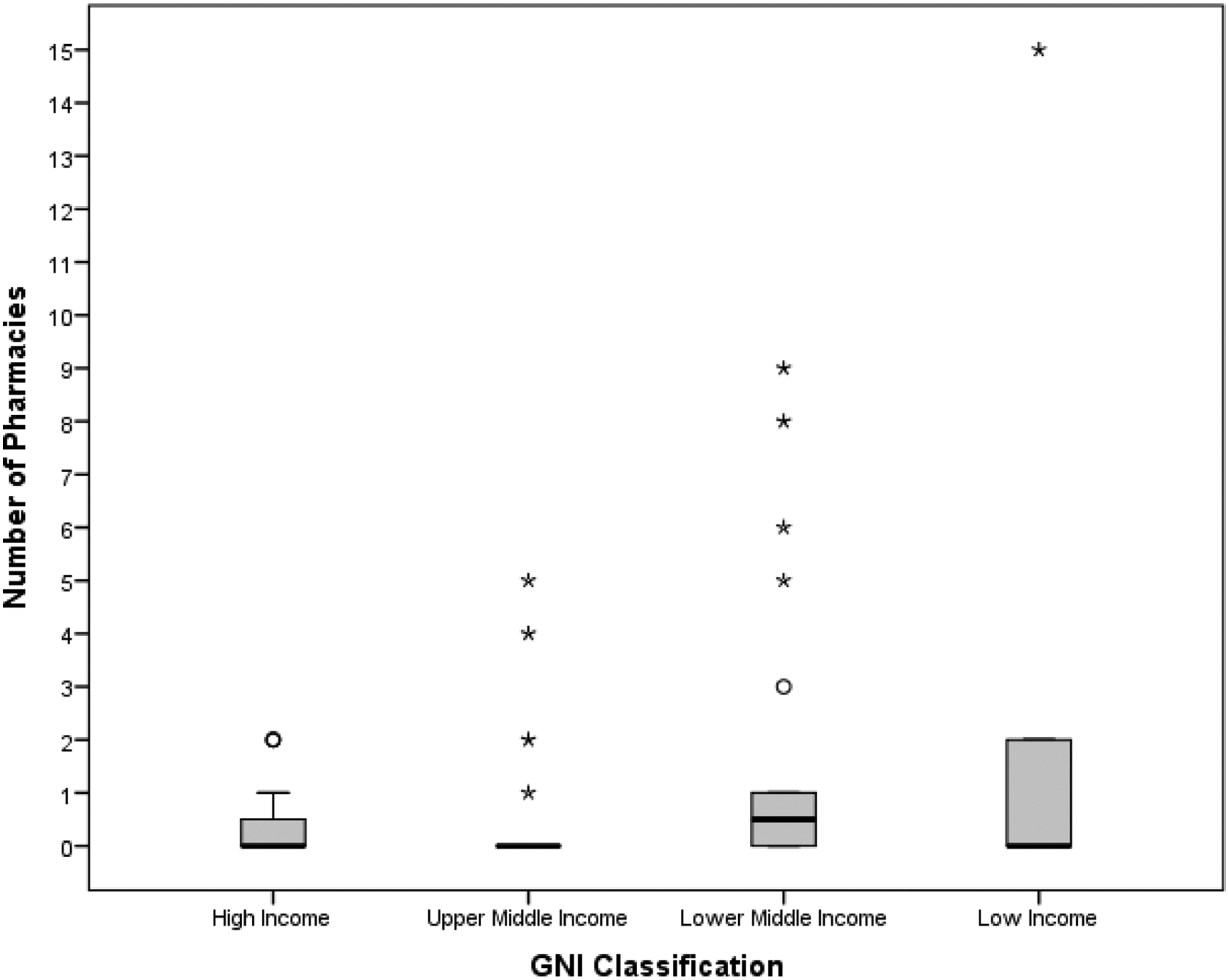
Number of pharmacies visited before finding one where at least one opioid was available within gross national income groups.
Almost 15% (n = 10) of the pharmacies visited had only one opioid and 34.3% (n = 23) had only two opioids available. Availability of formulations ranged from 92.3% in United Kingdom and Canada to 0% in Albania, Benin, and Guatemala (Antigua). In four locations, only one formulation was available [Nigeria, Guatemala (Guatemala City), Brazil (Rio de Janeiro), Bangladesh (Dhaka 2)]. In six locations, only two formulations were available: Uganda (Kampala 1 and 2), Mauritania, Kazakhstan, Brazil (Ribeirão Preto), and Armenia.
In Western Nepal, opioids are available only in one teaching hospital. They can only be prescribed by oncologists and injectable morphine can only be used for hospitalized patients. Participants from Albania, Dominican Republic, Lithuania, Mauritania, Thailand, and Uganda reported that opioids were available only in hospital pharmacies that dispense also for outpatients.
The availability of medications and their different formulations is strongly related to GNI level (Table 2) (Kruskal–Wallis tests p < 0.0001).
Kruskal–Wallis tests p < 0.0001.
HIC, higher income countries; LIC, low income countries; LMIC low middle income countries; UMIC, upper middle income countries.
On average, the countries reported 52% of all medicines and 34.4% of the 13 formulations as available (Table 3). Overall, injectable morphine was the most frequently available (73.1%, n = 49), followed by fentanyl TP (71.6%, n = 47) and morphine SR tablets (65.7%, n = 44). Morphine oral IR was available in 52.2% (n = 35) pharmacies. Morphine in liquid formulation was available in 38.8% (n = 26) of the pharmacies and methadone in 19.4% (n = 13). Hydromorphone liquid was the least available (only Canada and United States).
GNI, gross national income.
The number of medications and formulations available is correlated to the opioid consumption reported by PPSG (Rs = 0.488, CI = 0.272–0.704, p < 0.0001) and (Rs = 0.692, CI = 0.514–0.871, p < 0.0001).
Prices
Opioids are dispensed free in Costa Rica, Egypt, Kazakhstan, Lithuania (Kanuas 1 and 2), Moldova, Netherlands, New Zealand, Norway, Saudi Arabia, Thailand, Uganda, United Kingdom, and Zambia.
The mean price for morphine IR tablet for a 30-day treatment period ranged between USD 3.28 and 376, on average USD 78.5 (SD = 92.0, Me = 49.7, IQR = 80.5). Methadone tablet had the lowest price (mean = 40.5, SD = 29.1, Me = 26.5, IQR = 38.3) followed by methadone oral liquid (mean = 58.8, SD = 103.3, Me = 13.1, IQR = 70.0) and hydromorphone SR (mean = 51.6, SD = 54.9, Me = 14.9, IQR = 89.1). Synthetic opioids and in some cases SR opioids were cheaper than morphine IR tablets. Oxycodone oral (SR) was the most expensive formulation (mean = 312.4, SD = 252.1, Me = 237.2, IQR = 473.2) followed by oxycodone oral IR (mean = 198.1, SD = 125.2, Me = 202.9, IQR = 156.8). Table 4 describes the prices for a 30-day treatment period compared between GNI.
In column “Free” the nominator equals number of countries where medication is dispensed free and denominator equals number of countries where medication is available.
IQR, interquartile range; Me, median.
The difference between the reported prices and the international reference price for morphine IR (one 10 mg tablet) ranged between 0.1 and 1.35 (Me = 0.8, IQR = 0.29). All the countries where morphine IR tablets were available at the time of the survey reported prices below the international reference price, with the exception of Panama and Portugal (Bragas) that reported higher prices (1.39 and 1.16, respectively).
Affordability
The mean number of minimum days' wages needed to purchase a 30-day treatment of morphine IR tablets was 15.8 days (SD = 18.84, Me = 8.63, ID = 22,2), varying greatly by country: from 54.76 (Togo), 54.75 (Bangladesh), and 53.52 (Rwanda) to less than one day in Portugal (Porto 0.30 and Lisbon 0.16) and Ireland (0.22) (Table 5).
Results indicate that when opioids are not dispensed for free, morphine IR tablet is less affordable in countries in lower income groups: LIC (mean = 54.1 ± 0.873, Me = 54.1), LMIC (mean = 21.1 ± 19.6, Me = 10.6), UMIC (mean = 14.1 ± 14.1, Me = 10.23), and HIC (mean = 3.2 ± 5.2, Me = 1.33). In general, a negative correlation between the number of days and the country income category (Rs = −0.7; p < 0.001) was identified.
Comparison with phase 1
Of the 43 countries, 12 were also included in the first phase of OPW (Bangladesh, Brazil, Guatemala, India, Kenya, Nepal, New Zealand, Nigeria, Norway, Poland, Uganda, and United Kingdom). Compared to the first phase, the average availability of opioids and formulations increased slightly (opioids 1.8 to 2.3, formulations 3.5 to 4). The price of morphine oral IR increased too from 29.7 to 32.81 while the affordability improved slightly from 20.7 to 15.4 days. These changes were not statistically significant (Wilcoxon test).
Discussion
This is the second study that presents information on the differences among availability and affordability of opioids across the World Bank GNI groups. It follows the OPW pilot study published in 2014.
All the reports were from large or medium urban centers. This is not surprising given that we investigated pharmacies close to a health facility that provides diagnostic and treatment services for patients with life-threatening conditions such as HIV and cancer and that these major treatment centers are usually located in large urban areas.
Availability
None of the participants replied yes to the question about opioids never being available in their countries, which is an indication of progress. 8 However, three participants reported that no opioids were available in any of the pharmacies they visited [Albania, Benin, and Guatemala (Antigua)] at the time of the survey. There are many reasons as to why opioids may not be available at a given time in a pharmacy and this analysis is beyond the scope of the study. Reports have suggested that onerous reporting systems, restrictive norms, and requirements on the storage and dispensing of controlled medications may result in an administrative decision not to store or dispense the medication.30–32
The possibility of having more than one opioid available at the pharmacy is directly correlated to the country's GNI, consistent with opioid consumption reports. However, participants often had to visit more than one pharmacy, and in one case, in an LIC, the participant visited 15 pharmacies before finding one that stocked opioids.
According with the INCB, consumption remains very inadequate (<100 S-DDD) in Central America and Caribbean, Africa and South Asia, or inadequate (101–200 S-DDD) in East and South-East Asia and Eastern Europe. Impediments to use include an absence of training and awareness in medical professionals, fear of dependence, restricted financial resources, issues in sourcing, cultural attitudes, fear of diversion, international trade controls, and onerous regulation. 6 The WHA Assembly Palliative Care Resolution, the resulting UNGASS recommendations, as well as global campaigns by NGOs may have had a positive effect in the improvements in the reported availability of opioids.33–37 Colombia and Mexico in the UMIC group had all the medications available; Egypt, El Salvador, and Kenya within the LMIC group had four medications available; and Togo in the Low group had two medications available.
The availability of opioid medications may be improved through adequate supply management, better assessment of estimated needs, improvements in education, and the elimination of unduly restrictive barriers. 15 Specific legal and regulatory barriers have been described for opioids,32,38,39 and the WHO has published specific guidelines for ensuring access to controlled medicines, including opioids. 40 Palliative care training for undergraduate professionals may also improve skills and knowledge on how to adequately asses and treat patients with severe pain. 30
In 2013, the WHO updated the edition of the EML, creating a new section called Medicines for Pain and Palliative Care, which includes all the morphine formulations and lists oxycodone and hydromorphone as alternatives to morphine. 41 However, only 42% and 19.4% of the pharmacies that had morphine available also had oxycodone and hydromorphone available (n = 23 and 12, respectively). Oxycodone and hydromorphone are not available in LIC and only in a few pharmacies in LMIC.
Prices
Results show that the average price of a morphine IR tablet/capsule (10 mg) for one 30-day treatment was USD $13 higher per month in LIC than in HIC ($108 vs. $95.67). Higher costs in LIC are even more serious, considering their lower purchasing power.
Morphine injectable and oxycodone (SR and IR) were the highest-priced medications, both included in the WHO Model List of Essential Medicines (oxycodone as a substitute for morphine).
Results also show that for six formulations, UMIC had the highest prices for a 30-day treatment among the GNI groups (Table 4). This may not only reflect the fact that these countries have more purchasing power than countries in LMIC and LIC but also that the funding pool to cover healthcare expenditures is inadequate or not available as in HIC. This results in costs transferred to the patients, who have to pay out of pocket.
Methadone was priced lower than morphine in almost all the countries where available. It is important to note that methadone is often used in harm reduction programs as substitution therapy for dependence syndrome. However, its use as an analgesic is increasing, especially in palliative care.42,43
Some improvement was observed in relation to the first phase. The vast majority of the countries reported dispensing prices below the international reference price. This indicates that governments (in varying degrees) are subsidizing the morphine IR tablet and may reflect national efforts to improve access to patients in need. However, in Panama and Portugal (Bragas), patients have to pay a higher price (139% and 116%, respectively) than the price of the medication in the international market, indicating that all the licensing, procurement, importation, distribution, and other costs are transferred to the patient. This negatively impacts access and is not in accordance with the recommendations of the WHO and the WHA resolution, which call on governments to take the necessary steps to ensure access to analgesics for the relief of suffering.
Affordability
Measured in the number of days' minimum wages, this went up to 55 days in Bangladesh. All countries with lowest affordability were in the LIC or LMIC regions, with the exception of Panama (UMIC). Many people in these countries earn less than the minimum wages used in this study.
Measured in the number of days' minimum wages, treatment costs of oral morphine IR tablet went up to 55 days in Bangladesh. All countries with lowest affordability were in the LIC or LMIC regions, with the exception of Panama (UMIC). Many people in these countries live below the international poverty line of USD 1.25/day, 44 indicating that the number of working days needed to pay the cost of treatment may be higher than the results in this study and that pain treatment is accessible to only a few who can afford it.
These results continue to reflect the vast global inequities in access to pain treatment: the lower the income, the more working days required to pay for the treatment with oral morphine. These results are similar to those found in the first phase of OPW.
Limitations
OPW follows a methodology similar to the one used by HAI/WHO, but, as explained above, HAI does not include controlled medications in its reports. Opioids are internationally controlled, thus, availability as well as pricing are impacted by additional factors, such as markups resulting from safety and security measures required by the international conventions and national laws on the manufacturing, importation, distribution, storage, and dispensation. This survey is unable to determine the extent of the impact of these measures on the dispensed price of the medication. However, as we have noted in this article, national laws are often focused on the prevention of abuse, misuse, or diversion and not balanced toward access to opioids for medical purposes.
This study is based on the data collected from external collaborators, and it is not possible to determine how rigidly they followed the instructions. This study is a cross-sectional survey for a specific day in a specific location. The information reflects opioid availability in a specific pharmacy on this day so no inferences regarding availability in the whole country are possible. Although results indicate that several opioids and formulations were not available at the time of the survey, it does not imply that these opioids are never available in such locations. Out of stock occurs frequently, especially in LIC and MLIC, so the results on availability might differ in a longitudinal survey. However, the results reflect the situation that patients in need of opioids may face in any given day.
The study is based on a sample of data of a local pharmacy in the countries included in the study, which is not representative of the whole country. Indeed, we found international differences such as in India, where the affordability for morphine IR tablets varies from 1.76 (New Delhi 1) to 40.56 (Mumbai). However, the fact that pharmacies were located near to major treating centers may suggest that other pharmacies distant from hospitals may have even fewer medications in stock.
We used DDDs provided by WHO, but these may lead to an underestimation of costs due to two reasons: First, the DDD for each opioid does not correspond to the accepted equianalgesic conversion ratios. For example, a DDD of 100 mg oral morphine is not equivalent to 75 mg oral oxycodone (which is the DDD for oxycodone), but rather to 50 to 66 mg of oxycodone. In addition, as their disease progresses, many patients will likely need higher doses than these DDDs. Thus, the total amount of medication needed to treat may be higher, resulting in higher cost for treatment.
Conclusion
OPW is the only global monitoring mechanism to report the dispensing price of opioids and as such serves as a unique source of information on how prices affect access. This study indicates that patients in LIC and MIC have less access to opioid medications and highlights the need to continue efforts at improving access, availability, and affordability. There is an urgent need for revision of national medicine policies regulating access to opioids. Collaborative efforts should be made by governments, healthcare administrators, pharmacists, and prescribers to ensure that opioids are available. Governments and policy makers need to take the necessary steps to ensure that patients are able to receive the treatment they need. Prices can be reduced by strategies such as manufacturing oral morphine in the country, eliminating taxes and tariffs, eliminating red tape, regulating price increases, and regularly monitoring the distribution chain to maximize efficiency in the use of resources. Additional research needs to be developed to identify the reasons behind some of the differences in prices among the medications.
Footnotes
Acknowledgments
The following individuals contributed to the second phase of OPW: IAHPC webmaster: Danilo Fritzler provided the technical support and guidance in the data collection and reporting processes. Participants (in alphabetical order by country, last name, first name): Laska, Irena (Albania); Tadevosyan, Artashes (Armenia); Munroe, Margo (Bahamas); Biswas, Fazle Noor (Bangladesh); Mariam, Lubna (Bangladesh); Djossou, Koumagnon Alfred (Benin); Honorato Giardini, Mariana (Brazil); Barbosa, Maria (Brazil); Ferreira Arcuri, Juliano (Brazil); Ralph, Christopher (Canada); Franco, Martha (Colombia); Medina, Andrea (Costa Rica); Carvajal, Gabriel (Costa Rica); Gómez García, Wendy Cristhyna (Dominican Republic); Kamal, Sherif (Egypt); Abdelgawad, Omar (Egypt); Lopez Saca, José Mario (El Salvador); Ahmed, Ebtesam (Guatemala); Antonia, Laura (Guatemala); Vaszily, Éva (Hungary); Bhatnagar, Sushma (India); Mohan, Ravinder (India); Joad, Anjum (India); Ghoshal, Arunangshu (India); Sanghavi, Dr Priti (India); Tahmasebi, Mamak (Iran); Wright, Marie (Ireland); Kunirova, Gulnara (Kazakhstan); Waka, Mildred (Kenya); Mukosi, Gladys (Kenya); Weru, John (Kenya); Nduku, Gladys (Kenya); Osman, Hibah (Lebanon); Poniškaitienė, Marija Inesa (Lithuania); Aliou, Gadio Ndiaye (Mauritania); Templos Esteban, Luz Adriana (Mexico); Matos, Iraima (Mexico); Alvarez, Rosa (Mexico); Carafizi, Natalia (Moldova); Pogonet, Vadim (Moldova); Powys, Ruth (Nepal); Scholten, Willem (Netherlands); Griffiths, Emma (New Zealand); Soyannwo, Olaitan (Nigeria); Einen, Margrete (Norway); Camaño, Nisla (Panama); Kotlinska-Lemieszek, Aleksandra (Poland); Kluczna, Agnieszka (Poland); Gradalski, Tomasz (Poland); Feio, Madalena (Portugal); Encarnação, Paula (Portugal); Castro-Lopes, Jose (Portugal); Mugeni, Regine (Rwanda); Lam, Amanda (Samoa); Duraisamy, Balaji (Saudi Arabia); Brian, Matthias (Sweden); Sawatphanit, Sakkaphan (Thailand); Tengue, Koffi Anoumou (Togo); Ntege, Christopher (Uganda); Zirimenya, Ludoviko (Uganda); Murray, Scott (United Kingdom); Butner, Jenna (United States), DO, Thanh (Vietnam); and Chaila, Mwate Joseph (Zambia). This study was supported by grants to the IAHPC from the US Cancer Pain Relief Committee and Atlantic Philanthropies.
Author Disclosure Statement
No competing financial interests exist.