
Abstract
Abstract
Background:
Employment-related issues have been largely overlooked in cancer patients needing palliative care. These issues may become more relevant as cancer evolves into more of a chronic illness and palliative care is provided independent of stage or prognosis.
Objective:
To characterize the employment situations of working-age palliative care patients.
Design:
Cross-sectional survey setting/subjects: Consecutive sample of 112 patients followed in palliative care outpatient clinics at a comprehensive cancer center.
Measurements:
Thirty-seven-item self-report questionnaire covering demographics, clinical status, and work experiences since diagnosis.
Results:
The commonest cancer diagnoses were breast, colorectal, gynecological, and lung. Eighty-one percent had active disease. Seventy-four percent were on treatment. Eighty percent recalled being employed at the time of diagnosis, with 65% working full time. At the time of the survey, 44% were employed and 26% were working full time. Most participants said work was important, made them feel normal, and helped them feel they were “beating the cancer”. Factors associated with being employed included male gender, self-employed, and taking less than three months off work. Respondents with pain and/or other symptoms were significantly less likely to be working. On multivariate analysis, only pain (odds ratio [OR] 8.16, p < 0.001) and other physical symptoms (OR 5.90, p = 0.012) predicted work status; gender (OR 2.07), self-employed (OR 3.07), and current chemotherapy (OR 1.81) were included in the model, but were not statistically significant in this small sample.
Conclusion:
Work may be an important issue for some palliative care patients. Additional research is needed to facilitate ongoing employment for those who wish or need to continue working.
Introduction
P
Studies of return-to-work (RTW) in disease-free cancer survivors indicate a complex transition back impacted by various medical and nonmedical factors, including type of cancer, treatment modalities used, occupational category, and workplace environment.6,7 The issues facing patients with active disease on treatment are likely to extend beyond those of the disease-free survivor, 8 and include impact on work ability of pain, other symptoms, and side effects of narcotics; frequency of medical appointments; coping with the risk of progression; development of uncontrollable disease; and the possibility of dying. These issues fall within the scope of palliative care.
The aim of this exploratory study was to survey the perspectives on the work life of contemporary palliative care patients. Secondary aims included to document changes in work status during the illness trajectory and to identify predictors of remaining in employment in this situation.
Methods
Consecutive patients being followed in two Pain and Palliative Care (PPC) clinics at a Memorial Sloan Kettering Cancer Center (MSKCC) in New York were offered to complete the survey if they were aged 25–65 years when diagnosed, spoke English, and had ever been in paid employment. The survey instrument consisted of a 37-item self-report questionnaire developed by the authors for the purposes of the study. It inquired about demographics, cancer details, and work-related issues such as occupation, employment history, attitudes toward work, and factors affecting work ability. The MSKCC Institutional Review Board (IRB) deemed the study to be exempt research and respondents were required only to give verbal consent on the condition that the surveys were anonymous and not linked to the medical record. Descriptive statistics were used to summarize responses. Simple comparative statistics (e.g., t-tests, Fisher's exact tests) were used for group comparisons. Univariate and multivariate analyses using logistic regression tested for associations between current work status and demographics, cancer history, and the various work-related issues. Statistical analysis with a two-sided significance threshold of p < 0.05 was performed using SPSS Version 9.4
Results
Of 112 distributed surveys, 105 (94%) were completed. Among respondents, 81% had “active” cancer, implying it was neither cured nor in remission, and 74% were undergoing treatment, of which 54% were receiving chemotherapy. Breast, colorectal, gynecological, and lung primaries were commonest. Respondents worked in a variety of industries. Managerial or professional specialties (e.g., accountants, IT specialists, attorneys, teachers, and health practitioners) dominated, reported by 35 (34%) respondents and 59% of current workers. Most occupations were not physically demanding. More than 60% worked for large organizations subject to the Americans with Disabilities Act (ADA) and the Family and Medical Leave Act (FMLA). Nineteen percent were self-employed.
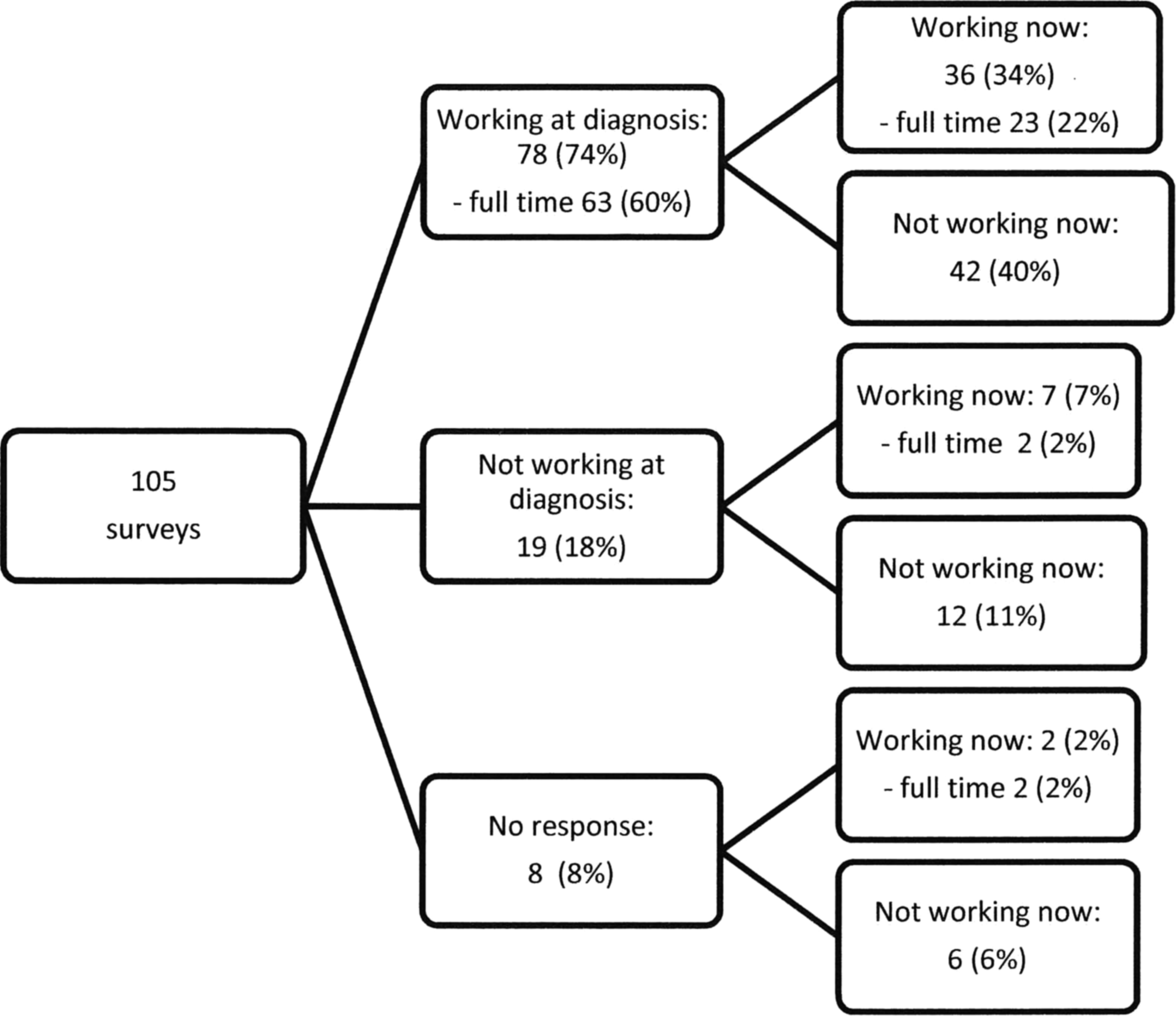
Eighty percent of respondents were employed when diagnosed, a median of two years earlier, with 65% working full time (Fig. 1). At the time of the survey, this number had fallen to 42%, with only 26% working full time and 47% working fewer hours than prediagnosis. Thirty (65%) current employees were being treated for cancer, but only 17% of chemotherapy recipients worked full time. Of the 99 respondents who reported their employment status both currently and before diagnosis, 45% had been stably employed, 39% had left employment, 13% had entered employment, and 8% were stably unemployed. Fifteen percent had worked throughout their cancer treatment, taking no time off. Forty percent of current workers wanted to work more, whereas 56% of unemployed respondents desired a job.
Work outcomes—time of diagnosis versus current
Patients' perspectives of their current work life are shown in Table 1, with the percentage (in bold) representing the two columns to its left, combined.
On univariate analysis, employment was significantly associated with male gender, being self-employed, taking less than three months off work after diagnosis, feeling normal, having fewer financial concerns, flexible work hours, and taking fewer absences. In contrast, being unemployed was significantly associated with the following: being in pain, fatigue, physical weakness, other physical symptoms, sadness, poor concentration, and side effects from pain medicines. In particular, patients with pain medicine side effects were four to five times less likely to be currently working than those without side effects (7/28 (25%) vs. 37/61(61%), odds ratio (OR) 4.83, (95% confidence intervals [CIs] 1.77–13.14), p = 0.0014). On multivariate analysis (n = 78), being in pain (OR 8.16, p < 0.001) and having other physical symptoms (OR 5.90, p = 0.012) remained statistically significant. Gender (OR 2.07), being self-employed (OR 3.07), and undergoing chemotherapy (OR 1.81) were also included in the model, but did not reach statistical significance.
Discussion
This exploratory survey revealed that almost half of 105 consecutive working-age patients attending these PPC clinics at MSKCC were currently in paid employment. This figure was surprisingly high and contrasts with the dearth of information on patients' employment issues in the palliative care literature. Work was important to most respondents and their identity. They had often taken little or no time away from the workplace since diagnosis. Many wanted to work more than they currently were, or to RTW if they were not currently employed.
The survey also revealed the impact of cancer and its treatment on employment. Forty percent of respondents who worked prediagnosis were now out sick, working part-time, or no longer in the workforce. This could reflect a change in their priorities or life choices, but may also indicate their inability to return to the workplace fully. Although occupational factors were not significant predictors of employment, the ORs for being employed currently favored managers or professionals, workers with flexible jobs in industries that were not very physically demanding, and employment in organizations protected by ADA and FMLA legislation. Other risk factors for not working are modifiable with good palliative care (e.g., symptoms and medication side effects).
As the prognosis of metastatic cancer improves, the opportunities and challenges for working in the face of metastatic disease are coming into sharper focus. 8 A recent study of the predictors of working or not in 683 patients with metastatic breast, colon, lung, or prostate cancer—of whom 34% were currently working—also showed performance status, symptom burden, and cancer treatment to be associated with work status. 8 In a recent systematic review of predictors of work outcomes in cancer patients, 7 advanced disease was a negative predictor of returning to work in several primary studies.9–13 So was receiving treatment, although 76%–100% worked prediagnosis, only 15%–56% worked while on treatment,2,8,14,15 and chemotherapy predicted for discontinuation of work. 16 However, none of these studies considered employment history, attitudes to work, and the work environment with the granularity presented here.
This exploratory study has many limitations. We only surveyed people about paid employment; arbitrarily excluding homemakers, volunteers, and nonemployed workers was not intended to diminish their desire to continue their endeavors while in palliative care. However, being employed and working are not synonymous, especially when one is on sick leave, which may be paid or unpaid. We do not have data on how many patients were screened or offered the survey. Our sample size of 105 completed surveys was a convenience sample that allowed us to finish this exploratory study in a meaningful timeframe. With a sample size of 105, we would be able to estimate a proportion with a maximum 95% CI half-width of 10. This means a margin of error of ±10%, which is acceptable for the exploratory nature of this study. Likewise, no adjustment was made for multiple testing. Because of the IRB's requirements, we could not verify the accuracy of the responses, in particular, the stage of disease, the cancer treatment, and the medication list. However, the validity of self-reported clinical data has been documented previously, and this approach is generally accepted in survey research.17–19 Recall bias is clearly relevant in this kind of survey, whereas the small sample size makes the results prone to type II errors. Lastly, these findings may not be generalizable beyond the setting of a comprehensive cancer center in a large American city.
Despite the limitations, the findings suggest work is important to many palliative care patients, and palliative care clinicians need to be competent in discussing work life with them. More research on this topic appears warranted. In particular, work outcomes could be relevant end points in some palliative care trials. Interventions to help patients to advocate for themselves in the workplace should be designed and evaluated. Multidisciplinary interventions combining vocational counseling with patient education, patient counseling, and biofeedback-assisted behavioral training or physical exercises have been shown to be most effective in enhancing RTW after cancer treatment, 20 and could be tested in this setting.
Footnotes
Acknowledgment
This exploratory research work was not supported by any grants. The authors were all employees of Memorial Sloan Kettering Cancer Center at the time of data collection.
Author Disclosure Statement
No competing financial interests exist.