
Abstract
Abstract
Background:
Simpler alternatives to traditional advance directives that are easy to understand and available in multiple formats and can be initiated by patients and families will help facilitate advance care planning. The goal of this study was to compare the acceptability of the letter advance directive (LAD) to the traditional advance directive (TAD) of the state of California.
Design, Setting, Participants, and Measurements:
A web-based, randomized controlled trial was conducted, in which the participants were randomized to one of two types of advance directives (ADs): the LAD (intervention) or the TAD (control). Primary outcomes were participant ratings of the ease, value, and their level of comfort in the AD document they completed.
Results:
A total of 400 participants completed the study, with 216 randomized to the LAD and 184 to the TAD by a computerized algorithm. Overall, participants preferred the LAD to the TAD (success rate difference [SRD] = 0.46, 95th percentile confidence interval [CI]: 0.36–0.56, p < 0.001). The participants felt that, compared to the TAD, the LAD was easier to read and understand (SRD = 0.56, CI: 0.47–0.65, p < 0.001); better reflected what matters most to them (SRD = 0.39, CI: 0.29–0.48, p < 0.001); helped stimulate their thinking about the types of treatments they wanted at the end of life (SRD = 0.32, CI: 0.23–0.42, p < 0.001); allowed them to describe how they made medical decisions in their family (SRD = 0.31, CI: 0.21–0.40, p < 0.001); and could help their doctor(s) (SRD = 0.24, CI: 0.13–0.34, p < 0.001) and their families (SRD = 0.19, CI: 0.08–0.28, p < 0.001) understand their end-of-life treatment preferences.
Conclusions:
Patients reported the letter advance directive to be a better alternative to the traditional advance directive form.
Introduction
A
Advance care planning (ACP) is an ongoing process by which patients, their families, and the clinicians caring for them reflect on the patient's values and goals of care and use this information to inform the patient's current and future medical care. These plans can then be documented in an advance directive (AD). In fact, ADs were originally developed to give patients prospective autonomy11,12 and control over future medical decisions about EOL care. When they are no longer able to speak for themselves, the AD can guide their proxy decision makers and their doctors to make future decisions honoring the patient's recorded wishes and values. AD specifying treatment limits has been shown 13 to help patients defend against burdensome treatments, especially in geographic regions where physicians seem to dispense high-intensity treatments at the end of life. Despite multiple efforts to educate the public about the vital importance of ACP and documenting their care preferences, the social awareness about AD (and thus, their completion rates) remains poor 1 in all populations, including that of older adults.
State-issued “traditional advance directives” (TAD) are the current standard of care. Each state in the United States has verbiage specific to the state government. However, the basic information in the state-approved AD form of all states is similar. Unfortunately, the traditional advance directives are written at a high level of literacy and it is unclear how well it may be suitable for patients from diverse cultures and languages. Concerns have been raised14,15 that patients from ethnic minorities and those with lower education and literacy skills are less likely to complete AD. In the absence of knowledge of the patients' goals and values for EOL care, doctors and the patient's proxy are left to blindly make major medical decisions on behalf of seriously ill patients, who may then be subjected to ineffective and burdensome treatments16,17 at the EOL.
Currently, AD documentation is mostly initiated by clinicians. While doctors agree that ADs are important,18–20 they also report many barriers 21 to conducting EOL conversations with patients. In our prior work we have shown that diverse patients endorse the great importance of having EOL conversations but also report multiple barriers 22 to engaging their doctors and their family members in such discussions. One strategy to help patients from diverse backgrounds overcome barriers to ACP is to provide access to a simple AD form written in a question and answer format that is easy to read, understand, and complete in one of many common languages. The questions prompt patients to respond to key issues and the template allows the completed document to be printed as a letter from the patient to the doctors describing their care preferences.
In an effort to create a simple alternative to the traditional advance directive, we worked in close collaboration with patients from diverse backgrounds to design, develop, pilot, and refine a letter advance directive (LAD) that uses a question and answer template to help patients write a letter to their doctor(s) about their care preferences. Fortunately, the law allows for simpler alternatives like the LAD as long as they comply with the legal requirements related to witnessing or notarization. Such simple alternatives should be designed in conjunction with patients and be available in multiple languages and formats that is feasible for patients and families to initiate and complete by themselves. They can use the completed document to have a focused discussion with the providers, clarify finer points, upload it into the electronic medical records, retain a copy for their records, and update as necessary. In fact, the recent Institute of Medicine report on Dying in America 1 recommended that online ADs should be utilized to elicit patients' wishes and identify their healthcare proxies and other relevant information to remedy some of current national problems related to AD.
In this article, we report the results of a randomized study comparing the State of California's traditional advance directive (TAD) to an alternative directive (LAD) written in the form of a letter from the patient to the doctor, which is available electronically, as well as in print.
Materials and Methods
Design of the letter advance directive
Focus groups were conducted in multiple languages (English, Chinese, Hindi, Russian, Spanish, Tagalog, Vietnamese, and Urdu) in community centers in the San Francisco Bay Area with medical interpreters to engage diverse patients and families in their preferred language. Working with them, we designed the letter advance directive (LAD) 23 in a question and answer format at a fifth grade reading level. The form was translated into seven languages 23 by medical interpreters and verified by back-translation for accuracy. The multilingual forms were reviewed and further edited by patients and families, including numerous older adults, for clarity of language and cultural acceptability (e.g., African American patients specifically recommended that the words “withhold” and “withdraw” be removed from the letter advance directive form as they felt uncomfortable signing a document containing those words). The final version of the LAD form is available in eight languages in print, as an interactive web-based form, an iOS application (accessible through iPhone/iPads), and an Android application (accessible on Android devices).
The LAD form is available online (http://med.stanford.edu/letter/advancedirective.html). When a patient answers the questions on the form and clicks the “print” button, a computer program automatically renders a prefilled AD with a supplemental letter to the doctor that documents the patient's preferences for EOL care. Implementation support for the LAD is provided by the American Medical Association through their Steps-Forward 24 portal. In this article, we report the results of a randomized clinical trial comparing the electronic English version of the LAD form to the TAD available online. The TAD was chosen as the comparator as it is a standard form approved by the State of California and as it is used widely in this densely populated and diverse state.
Study design
In 2015, the Stanford Institutional Review Board approved a study to evaluate the effectiveness of the Letter Project Directive in print and electronic formats and its ease of use and acceptability for patients from diverse backgrounds. This is a web-based, double-blind randomized control trial.
Participants
The project link was posted on the Letter Project portal (http://med.stanford.edu/letter.html) and disseminated through social media outlets; electronic list serves to recruit participants. Adults who were willing to participate were screened online to determine if they met the inclusion criteria for the study (must live in the United States, be 40 years or older, and must be able to read and respond online to questions posed on a secure platform).
Randomization and measures
Consenting participants (Table 1), who met the inclusion criteria and completed all baseline measures, were randomized (using a computer-generated algorithm) to complete an online version of either the California Probate Code Section 4700–470125 traditional California directive (TAD) or the letter advance directive (LAD). Self-reported race/ethnicity, gender, income, level of education, primary language, place of birth (in or outside United States), marital status, and importance ascribed to faith/religion/spirituality were obtained at baseline. All participants also completed the PROMIS Global Health 26 short form (a widely used 10-item instrument with a Global Physical Health component and Global Mental Health component that are valid and reliable). To ensure ability to read and respond accurately to online instructions, participants also completed two simple attention assessment tasks: (a) Click the number 100 on a zero to 100 linear scale and (b) Spell the word “survey.” A project manager with computer expertise monitored the study. The secure online system was programmed to ensure that a subject could only participate once. All questions in both arms were set at “force response” (i.e., participants who did not respond to all the questions were unable to submit their completed directive). The participants' states of residence were determined using their self-reported zip codes. The investigators had no direct contact with the participants.
Intervention
The LAD is available as an online fillable document written at a fifth grade level (Supplementary Data S1) and is available at the Letter Project portal 23 (http://med.stanford.edu/letter.html). The TAD (control) is available as an online fillable document written at a 12th grade reading level and is posted on the State of California's Department of Justice portal. 25 This form contains an overview and the purpose of AD; sections for designation of an attorney for healthcare; and instructions about EOL treatment choices, organ donation, autopsy, and treatment for alleviation of pain. Participants in both arms were allowed as much time as they needed to complete the assigned directive. Pilot testing showed that the average time taken to complete either form was about 12 minutes.
Outcomes
A set of seven questions were designed to assess the acceptability (two items), the usefulness of the AD document in capturing the participants' personal values and treatment preferences (three items), and its ability to assist the doctors and family members in making treatment decisions on their behalf (two items). These questions were formulated by discussions with multiethnic older adults and with multidisciplinary clinicians. Study participants used these seven questions to rate the AD form assigned to them (Table 2). The response category for each item was a five-point Likert scale ranging from “strongly agree” to “strongly disagree.”
p Values were calculated using the Mann-Whitney–Wilcoxon test, effect size reported is the SRD with the 95th percentile confidence intervals.
AD, advance directive; SRD, success rate difference.
Statistical analyses
We estimated that with a sample size of 200 patients assigned to the LAD (intervention) and 200 assigned to the TAD (control), and using a 5% two-tailed test, the study would have more than 99% power to detect a between-group difference of moderate or large effect size. All patients who underwent randomization and who were assigned to the intervention or the control were included in the analyses. The Mann-Whitney–Wilcoxon test was used to determine the p values and the effect size 27 to assess the impact of the LAD compared to the TAD. The effect size used was success rate difference (SRD). 27 SRD is defined as the probability that a LAD rating is more favorable than a TAD rating, minus the probability of the opposite. SRD values range from −1 (most favorable to TAD) to +1 (most favorable to LAD) with a null value of zero, with magnitudes of SRD = 0.1, 0.3, and 0.4 regarded as small, medium, and large effect sizes, respectively. All analyses were conducted using SAS Version 9.4, Cary, North Carolina. On an exploratory basis, we used recursive partitioning method to identify the characteristics that distinguished those who had from those who had not completed an AD before entering the study.
Results
Participant enrollment and baseline characteristics
Four hundred participants (see Fig. 1 for participant flow) who completed the baseline measures were randomized either to the LAD (intervention) or the TAD (control). Participants were from 41 different U.S. states, 197 men, 203 women, age range 40–90 years, mean (SD) = 56.7 (10.6). Both the intervention and control groups were similar in sociodemographic characteristics (Table 1) and self-reported health status as measured by the PROMIS Global Health 26 short form. Overall, 23% (92/400) had completed ADs before entering the study and they were more likely to be older (recursive partitioning analyses determined a cut point of participants who were ≥62 years old).
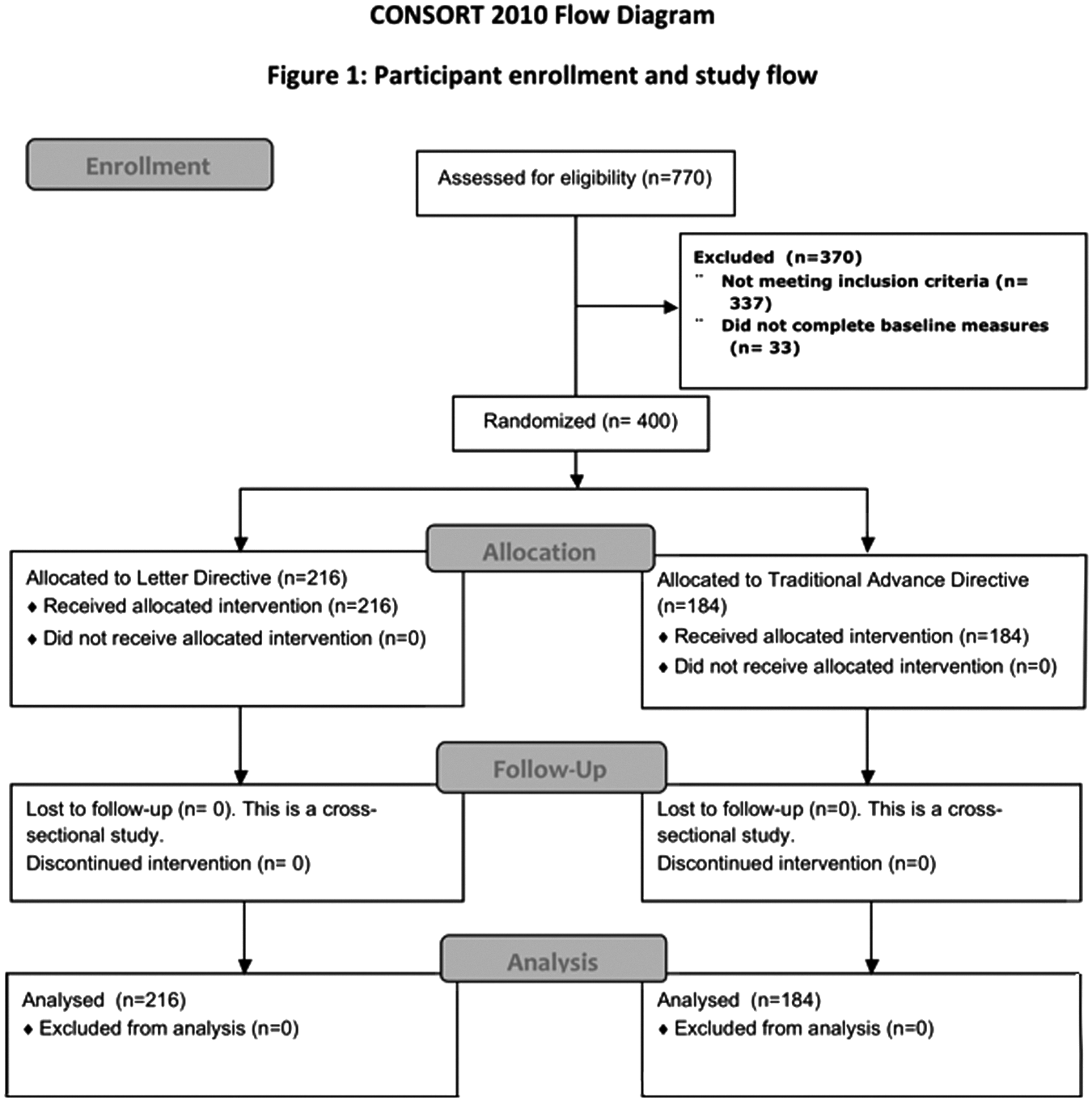
CONSORT diagram of participant enrollment and study flow.
Outcome assessment
A majority (89.4%) of the participants agreed or strongly agreed that they were more comfortable using the LAD compared to 72.8% for the TAD (p < 0.001, SRD = 0.30, 95th percentile confidence interval [CI]: 0.20–0.39). For all outcome measures, participants preferred LAD to the TAD. The SRD, confidence intervals, and p values are shown in Table 2. As responses to these questions were highly correlated (for all possible pairs of the seven questions, the Spearman's correlation coefficient ranged from 0.468 to 0.754), a principal components analysis was conducted; this analysis demonstrated that the seven questions reduced to a single factor that accounted for 33.4% of the total variance. Consequently, a composite outcome measure was calculated by averaging the responses of all seven questions for each subject. On the composite outcome, participants preferred the LAD compared to the TAD (SRD = 0.46, CI: 0.36–0.56, p < 0.001). Participants who were randomized to the traditional directive were twice as likely (39.7%) to refuse organ donation compared to the refusal rate of those who completed the letter advance directive (20.8%).
Discussion
In order for patients to receive preference-sensitive care at the EOL, clinicians need to help them identify various available treatment options so that they can weigh the risks and benefits of each choice and then document their wishes. If and when the patient loses the ability to make health decisions, both clinicians and the patient's proxy decision makers should honor the patient's expressed choices. The two common ethico-legal frameworks that guide proxy decision making for the incapacitated patient are substituted judgment and best interest standards. 28 In substituted judgment, the proxy should make decisions according to the patient's documented wishes. If the patient's wishes are not expressly conveyed, as is often the case in EOL decision making, the proxy should make an inference based on the patient's prior statements and values. If the patient's wishes are unknown, the proxy should use best interest standards and implement decisions after reflecting on the well-being of the patient. Traditional advance directives can place an undue burden16,17,29 on the proxy decision maker. Many offer only two choices: “choice-to-prolong” versus “choice-not-to-prolong,” both of which are umbrella terms that represent a variety of underlying treatments (ventilator support, nutritional support, dialyses, etc.). Each of these treatments can be instituted, withheld, or discontinued depending on the individual patient's circumstance and preferences. For example, in the letter advance directive, a patient can choose to have ventilator support and also describe the conditions under which such support should be discontinued. This flexible approach allows patients to express descriptive responses about time-limited trials of specific treatments with end points, thus clarifying their wishes and preferences (see Table 3 for exemplars). The letter advance directive also offers guidance to the doctor on what to do in event the proxy fails to honor the patient's stated choices.
The TAD does not inquire about these issues.
Making decisions about organ donation is a sensitive and challenging issue for many patients. Traditional advance directives offer only two choices such as opting in or out of organ donation. In many cultures,30,31 organ donation is a taboo topic. Patients may thus feel uncomfortable consenting to organ donation in their ADs. In addition to opting in or opting out, the letter advance directive provides a third option (unavailable in the traditional advance directive) by which patients can choose to have their proxy make decisions about organ donation after the patient's passing. Many participants who completed the letter directive deferred decision making to their proxy instead of categorically refusing to participate in organ donation. The LAD thus allows the opportunity for clinicians to approach the proxy about organ and tissue donation after the patient's death and can thus potentially increase the percentage of organ and tissue donors, an important public health benefit given the great national organ and tissue shortage.
Our study has limitations. It was an online study of adults who agreed to participate. We collected only demographic data and PROMIS Global Health as baseline measures to minimize the burden on respondents. Although the letter advance directive was developed in conjunction with and piloted on diverse community dwelling patients with limited English proficiency, this trial included only participants who were fluent in English and had the technical literacy to participate. The effectiveness of the letter advance directive needs to be tested in populations with lower levels of health literacy and limited English proficiency.
Conclusion
The letter advance directive is a simple document that patients and families can initiate by themselves. We compared the letter advance directive with the traditional advance directive document and found that participants preferred the letter as it is easy to read and understand and allowed patients to express what matters most to them, as well as their specific choices for treatments at the EOL. We acknowledge that patients' treatment preferences may change over time. Thus, longitudinal studies that document changes in preferences over time using the letter advance directive are the natural next step. Further research needs to be done to determine if the letter advance directive is effective in the clinical arena and how providers use it to shape clinical care provided to patients.
Footnotes
Acknowledgments
The Letter Project received the Practice Innovation Challenge Winner award from the American Medical Association (AMA) and the Medical Group Management Association (MGMA).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.