
Abstract
Abstract
Background:
Red Blood Cell (RBC) transfusions are commonly used in palliative care. RBCs are a finite resource, transfusions carry risks, and the net effect (benefits and harms) is poorly defined for people with life-limiting illnesses.
Objective:
To examine the indications and effects of RBC transfusion in palliative care patients.
Design:
This international, multisite, prospective consecutive cohort study.
Setting/Subjects:
Palliative care patients undergoing RBC transfusion.
Measurements:
Target symptoms (fatigue, breathlessness, generalized weakness, or dizziness) were assessed before transfusion and at day 7 by treating clinicians, using National Cancer Center Institute Common Terminology Criteria for Adverse Events. Assessment of harms was made at day 2.
Results:
One hundred and one transfusions with day 7 follow-up were collected. Median age was 72.0 (interquartile range 61.5–83.0) years, 58% men, and mean Australia-modified Karnofsky Performance Status (AKPS) of 48 (standard deviation [SD] 17). A mean 2.1 (SD 0.6) unit was tranfused. The target symptoms were fatigue (61%), breathlessness (16%), generalized weakness (12%), dizziness (6%), or other (5%). Forty-nine percent of transfusions improved the primary target symptom, and 78% of transfusions improved at least one of the target symptoms. Harms were infrequent and mild. An AKPS of 40%–50% was associated with higher chances of symptomatic benefit in the target symptom; however, no other predictors of response were identified.
Conclusions:
In the largest prospective consecutive case series to date, clinicians generally reported benefit, with minimal harms. Ongoing work is required to define the optimal patient- and clinician-reported hematological and functional outcome measures to optimize the use of donor blood and to minimize transfusion-associated risk.
Introduction
A
Anemia may contribute to symptoms, including chronic breathlessness and fatigue, limiting quality of life and function. 6 Reversing anemia through red blood cell (RBC) transfusion may help optimize function and reduce key symptoms. Transfusions are administered in 5%–18% of palliative care patients, with higher rates in hematological patients, inpatients, and those managed by oncological services.7–11
Evidence addressing the net effects (benefits and harms) of RBC transfusions in palliative care is limited, highlighted in two recent systematic reviews.1,2 These reviews found that most patients reported symptomatic benefit for a few weeks, low rates of adverse events, but no baseline predictors of the people most likely to benefit.
Concerns that need to be addressed in prospective studies include transfusion risks (minor circulatory overload, through to life-threatening complications such as lung injury, significant circulatory overload, sepsis, or blood group incompatibility). Transfusions used late in life may be associated with reduced survival, 12 and mortality rates of 13%–33% have been reported for these patients in the fortnight after RBC transfusion,8,13 likely reflecting the advanced stage of illness rather than a cause-and-effect relationship.
RBC transfusions are also relatively expensive; estimates of the cost of preparation and storage of one RBC unit are US$284 in Australia and US$210–343 in the United States,14,15 with the total cost (including administration) of a single unit of RBC transfusion in U.S. hospitals being between US$522–1183. 16 RBCs are also a limited resource, raising ethical challenges for palliative care clinicians in balancing individual patient needs and the wider societal requirements. 17
The aim of this study was to quantify prospectively in a multisite, consecutive cohort of hospice/palliative care patients the net clinical effects on anemia-related symptoms of RBC transfusions to help clinicians optimize future care. This study utilized the methodology of an international pharmacovigilance series, 18 but it is the first to examine a nonpharmacological intervention, and it complements the work of the International Haemovigilance Network. 19
Methods
This study collected data on RBC transfusions administered as part of a clinical routine by using an established methodology. 18 Patient demographics, disease, comorbidities (unweighted Charlson Comorbidity Index [CCI]), clinical phase, and functional state using the Australia-modified Karnofsky Performance Scale (AKPS) were collected.20–22
Benefits and harms were assessed by treating clinicians using the National Cancer Institute's Common Terminology Criteria for Adverse Events (NCI CTCAE) Likert scales, with a change of ≥1 considered as clinically significant.
An expert committee defined target symptoms (fatigue, breathlessness, generalized weakness, or dizziness) and harms (fever, infusion-related reaction, infusion site extravasation, hemolysis, heart failure, edema limbs, allergic reaction, and anaphylaxis). Clinicians were asked to nominate a primary symptom that RBC transfusion was targeting. Symptoms were assessed at baseline and day 7 for benefits on the basis that transfusions in the palliative setting should give benefits within a few days and be maintained beyond a few days. Harms were assessed at baseline, day 2 and on an ad hoc basis throughout the 7 days on the basis that the majority of harms would be transfusion related and would present early.
Nonidentifying data were then entered pro forma by using a 128-bit encrypted web portal (www.caresearch.com.au). Descriptive statistics were used for patient characteristics. Logistic regression was performed for target symptom benefit and benefit in any symptom using age, sex, AKPS, phase, CCI, and baseline hemoglobin. Post hoc analysis included a comparison of different strata of AKPS on transfusion response by using the chi-squared test. A p-value <0.05 was considered statistically significant. Analyses were performed in SPSS version 24 (IBM Corp., Armonk, NY).
Ethical approval was obtained for each participating site, either as ethical waivers (as quality assurance work) or approval as low-risk research.
Results
Seventeen sites (inpatient hospice/palliative care units, consultative services, and ambulatory clinics) in five countries entered data (January 2014–September 2015). At baseline, 141 patients were included, 131 had day 2 toxicity data, and 101 had day 7 benefit data (Table 1).
AKPS, Australian-modified Karnofsky Performance Status; BMI, body mass index; CCI, Charlson Comorbidity Index; IQR, interquartile range; RBC, red blood cell; SD, standard deviation.
Patients had a mean 2.1 (standard deviation 0.6) units of RBC transfused, and the predominant primary target symptom was fatigue [62/101 (61%)].
Benefit in the primary target symptom was found in 46/101 (49%; range 42%–67%; Table 2) and in any target symptom in 79/101 (78%). Changes in primary target symptom ratings are shown in Table 3. One target symptom improved in 30/101 (30%), two symptoms in 21/101 (21%), three symptoms in 18/101 (18%), and four to five symptoms in 10/101 (10%).
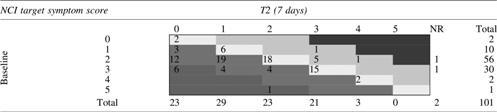
 represents improvement,
represents improvement,  indicates stable symptoms, and
indicates stable symptoms, and  /
/ represents deterioration.
represents deterioration.
NCI, National Cancer Institute; NR, not reported.
Harms at day 2 were few [16/131 (12%; Table 4)], and severity was mild. A further four patients had ad hoc reports of harm. Harms included a delayed allergic reaction, an infusion-related reaction, delirium, constipation, seizure, and vomiting.
Other included delirium (2), hypotension (1), leg cramp (1), nausea and vomiting (1), bruising (1), and not specified (1).
The maximal benefit in the primary target symptom was found at an AKPS of 50 (Fig. 1a–c), with benefits increasing with higher levels of function. Patients receiving transfusions with a baseline AKPS of 20–30, 40–50, and 60–70 had benefits in the primary target symptom of 36%, 66%, and 41%, respectively (p < 0.03). Conversely, there was a small reduction in benefit rates with increasing baseline hemoglobin.

Logistic regression found no impact of any baseline factors on benefit target symptoms.
Discussion
In the largest prospective series of RBC transfusions in palliative care patients to date, 49% of patients reduced their primary target symptom, with 78% benefiting from any target symptom. Fatigue was the most common symptom targeted. There were no clear predictors of response by primary target symptom, baseline hemoglobin, and phase, though increasing function may have some impact. Harms to patients were infrequent and minimal.
Subjective improvement has been reported after RBC transfusion in palliative care (51%–94%), but when self-reported assessment tools are used for fatigue, breathlessness, and well-being, a less consistent picture emerges.3,7,10,11,13,23 Clinicians commonly report improvement after RBC transfusion in 65%–89% of patients.3,8,9,11
Many harms were unlikely related to RBC transfusion. Previously reported harm rates are 6%–8%, though these rates do not always reflect systematic collection, nor incorporate severity.3,13
The lack of predictors of response to palliative RBC transfusion has been previously reported. 1 Although this finding may be true, it may also be due to small study sizes or widely varying patient populations studied.
The finding that patients with an AKPS of 40%–50% responded to RBC transfusions more often than those with lower or higher AKPS warrants further study. Three studies have shown no improvement in functional levels after RBC transfusions, using the Barthel Index and AKPS.7,11,13 Without a control arm, it cannot be established whether these people had current levels of function better maintained.
To date, the choice of an optimal outcome measure for RBC transfusions in palliative care patients remains elusive but would ideally incorporate self-report globally, symptom-specific and quality-of-life measures, and functional changes.
In addition to Phase IV studies such as this, ultimately addressing the net effect of RBC transfusion patients in palliative care would require a comparison arm. A possible study design to address this question, as used for other clinical questions, is to compare a generous versus conservative threshold for transfusion.
Clinically, RBC transfusions in palliative care patients require a careful, mechanistic-based approach, accounting for the context of the patient, their comorbidities, prognosis, and their goals of care. Basic investigations of treatable causes for anemia in palliative care are not routinely undertaken—9% of patients having transfusions in one study had hematinics checked (B12, folate, ferritin, or combination). 8 By contrast, another study of anemic palliative care patients found occult folate and B12 deficiency in nearly 30% and 7% patients, respectively. 4 Could the use of erythropoietin for those with renal dysfunction, or iron supplementation for those with absolute or functional iron deficiency, ameliorate the need for transfusions in some sub-groups?
Limitations
Data beyond seven days were not gathered. A Cochrane review of RBC transfusions in advanced cancer found that the benefit lasted around 14 days. 2 Other concurrent treatments or changes in clinical condition that may have affected the symptom scores were not collected. The NCI CTCAE only uses a 3-point rating scale (5 point for breathlessness) without psychometric validation; however, evidence demonstrates favorable validity, reliability, and responsiveness in a large cohort study. 24
The incomplete data of benefit for 39 patients limit the generalizability. Reporting of harms beyond day 2 was ad hoc and is unlikely to reflect all harms.
Conclusion
In palliative care patients, clinicians believed that RBC transfusion gave subjective improvement to three-quarters of patients, with minimal harm. The optimal methodology to measure the net effect of transfusions remains challenging. Future studies should examine treatable causes of anemia and consider objective measures of response to transfusions, such as activity monitors.
Footnotes
Acknowledgments
Thanks go to the patients, clinicians, and sites for their participation. Participating sites include: Braeside Hospital, Sacred Heart Hospice, St Vincent's, Sydney, Calvary Health Care, Greenwich Hospital, St. Vincent's Health, Barwon Health, Royal Melbourne Hospital, Southern Adelaide Palliative Services, Wolper Private Hospital, Prince of Wales Hospital, Mercy Hospice, NZ, National Cancer Centre Hospital, Japan, Grey Nuns Hospital, Edmonton, Canada, St Catherine's Hospice, Scarborough, UK, Marie Curie Hospice, Bradford, UK, Sue Ryder Leckhampton Court Hospice, Cheltenham, UK, Hayword House Macmillan Specialist Palliative Care Cancer Unit, Nottingham, UK, and St Gemma's Hospice, Leeds, UK. The Australian Palliative Care Clinical Studies Collaborative is supported by funding from the Palliative Care Branch of the Australian Government's Department of Health.
Author Disclosure Statement
No competing financial interests exist.