
Abstract
Abstract
Background:
Compared with nociceptive pain, neuropathic pain is a challenging diagnosis to make and successfully treat in children with cancer.
Objective:
The objective of this case report was to see whether very-low-dose methadone (VLDM) (defined as <50% of accepted starting analgesic dose of methadone for children) would be an effective strategy to treat refractory neuropathic pain due to vincristine in two children with acute lymphoblastic leukemia.
Methods:
This case report is based on the clinical experience and parent-reported outcomes of two children with refractory neuropathic pain who received VLDM.
Results:
Based on parent/caregiver-reported outcome scores over a one-year period, both children's refractory neuropathic pain syndrome was successfully treated with the addition of VLDM to their pre-existing regimen of gabapentin. Neither child suffered any adverse effects from methadone.
Conclusions:
VLDM shows promise as an effective, safe, and inexpensive way to treat refractory neuropathic pain in children with cancer.
Introduction
C
Neuropathic pain is triggered and sustained by the upregulation and activation of N-methyl-
This may interest pediatricians, as there is often hesitation and anxiety to use methadone due to its complex pharmacokinetics and pharmacodynamics. 11 Adult studies document the use of very-low-dose methadone (VLDM) combined with haloperidol as an effective regimen to treat pain.12,13 Based on these adult studies, we hypothesized that doses lower than the standard starting doses of methadone (0.1 mg/kg/dose q12 hours5,14) may be beneficial in the treatment of refractory neuropathic pain in children.
Case Reports
Patient 1
A 19-month-old boy with acute lymphoblastic leukemia (ALL) receiving maintenance chemotherapy, including vincristine, was referred to pediatric supportive care (PSC) for insomnia. The parents had consistent bedtime rituals with good sleep hygiene. His mother reported no difficulty with initiation of sleep, but he struggled with maintenance of sleep. He would wake for ∼60 minutes and would be consoled by his parents with holding, massage, acetaminophen, and provision of a bottle. Sleep would resume for ∼90–120 minutes only for the cycle to repeat. There was no excessive daytime somnolence, and he would take 2 naps/day. He would not awake during daytime naps. The initial parental assessment of symptom severity is seen in Figure 1.
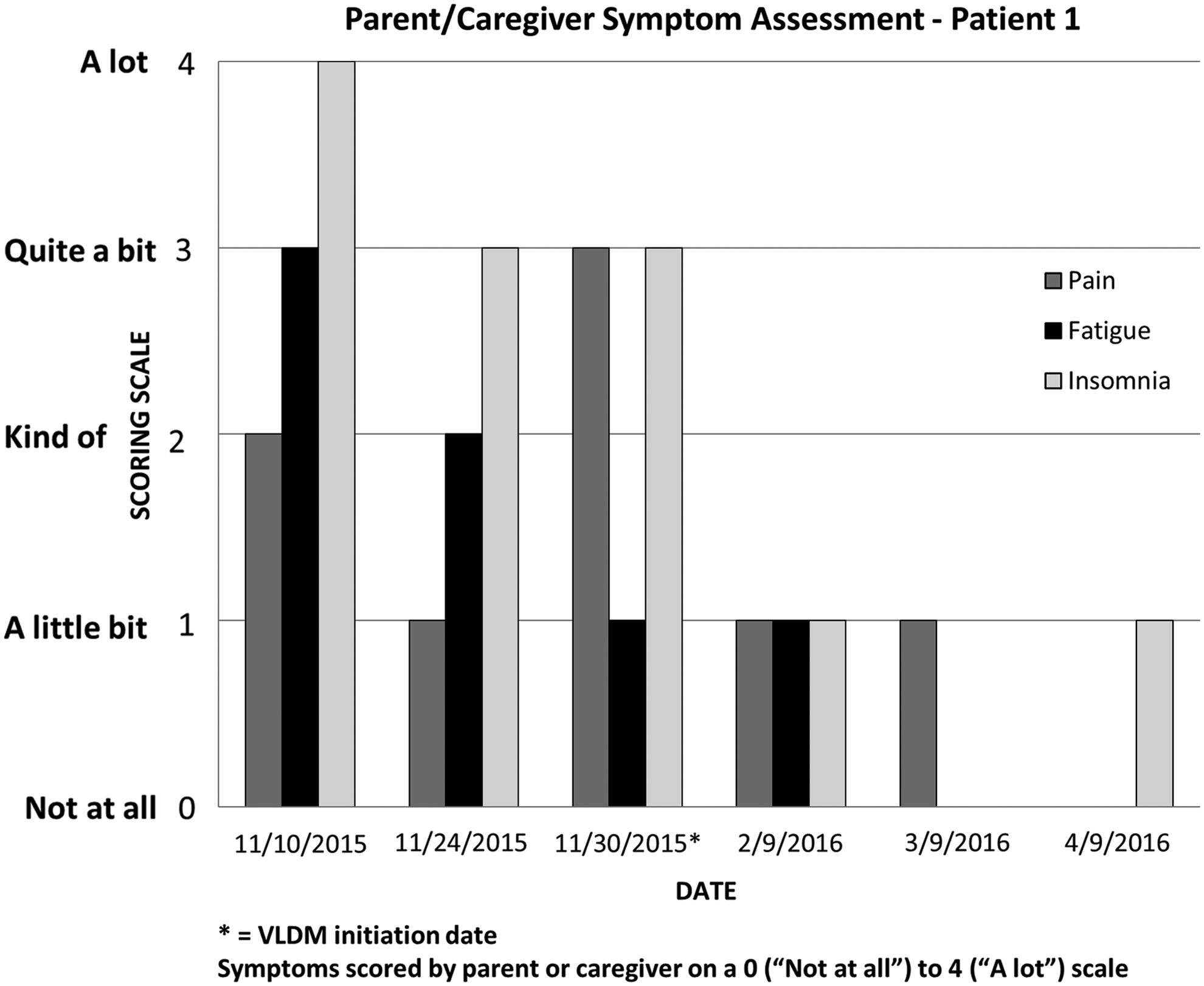
Parent/Caregiver Symptom Assessment, Patient 1: Symptoms scored by parent or caregiver on a 0 (“Not at all”) to 4 (“A lot”) scale.
Other pediatric oncology providers attempted to maintain sleep with melatonin, diphenhydramine, lorazepam, and amitriptyline. Melatonin [2.5 mg po qHS (0.25 mg/kg/dose) for 14 days] and amitriptyline [2.5 mg po qHS (0.25 mg/kg/dose) for 20 days] were tried but stopped due to lack of efficacy. Lorazepam [0.4 mg po qHS (0.05 mg/kg/dose) for two doses] and diphenhydramine [10 mg po qHS (0.1 mg/kg/dose) for 3 doses] were tried but stopped due to paradoxical reactions.
With a presumptive diagnosis of insomnia, olanzapine 0.5 mg po qHS (0.05 mg/kg/dose) was initiated, but it did not help after seven days. Titration to 2.5 mg po qHS (0.25 mg/kg/dose) for six days did not improve the maintenance of sleep and so it was discontinued.
At follow-up, the mother reported that the child did not like pajama bottoms put on at night, crying as if in pain; he did not mind looser fitting jeans during the morning or daytime hours. The mother also noted delay in the gross motor skill of walking despite receiving physical therapy. He plateaued at the level of pulling to stand and “cruising.” The physical exam was significant for the gross motor delay of independent walking. Cranial nerves and muscle tone were normal, patellar deep tendon reflexes were 1+ bilaterally, and there was no foot drop. Sensory examination could not be performed due to the developmental language capacity of the child.
Vincristine (0.75 mg/m2 body surface area) was given monthly according to the Children's Oncology Group protocol AALL-0631. Considering insomnia secondary to neuropathic pain from vincristine, amitriptyline 2.5 mg po qHS (0.25 mg/kg/dose) was restarted and added to the child's gabapentin dose of 45 mg/kg/day. No clinical benefit was observed after 14 days. The dose was increased to 5 mg po qHS (0.5 mg/kg/dose) but discontinued after 16 days as it was not effective.
After discussion with the family, VLDM (defined as <50% of the accepted starting dose of 0.1 mg/kg/dose) was initiated at 0.3 mg po q12 hours (0.03 mg/kg/dose). Within three days, the mother reported that the child's sleep improved—there were fewer awakenings, and time awake was shorter. Within seven days, the child slept through the night and began to walk unassisted. The PSC note documents, “[H]e is sleeping through the night. He allows his mother to place full length pajamas on him, and cover him with a blanket at night which they previously had been unable to do.”
Four months after initiation of VLDM, he continued to have low scores of pain, fatigue, and insomnia (Fig. 1). He did not have any adverse side effects, including excessive somnolence, myoclonus, or respiratory depression. A brief increase in pain scores was observed with an attempted wean of gabapentin, but it again decreased after gabapentin returned to 45 mg/kg/day. One year after initiating VLDM therapy, the patient completed vincristine, and gabapentin and methadone were sequentially weaned off over a six-week period without return of the original pain syndrome.
Patient 2
A six-year-old boy with ALL in remission on maintenance chemotherapy, including vincristine, had a one-year history of vague pain in his legs and back that was presumed to be neuropathic pain. He was treated by his oncologist with gabapentin at 45 mg/kg/day, and morphine elixir 4 mg po q4 hours as needed (0.2 mg/kg/dose) was added due to paroxysms of pain. Initially, the child was taking 3–4 doses/24-hour period. This was not effective, and the child was referred to PSC for pain that was not responsive to μ-opioid agonists. The initial parental assessment of symptom severity is seen in Figure 2.
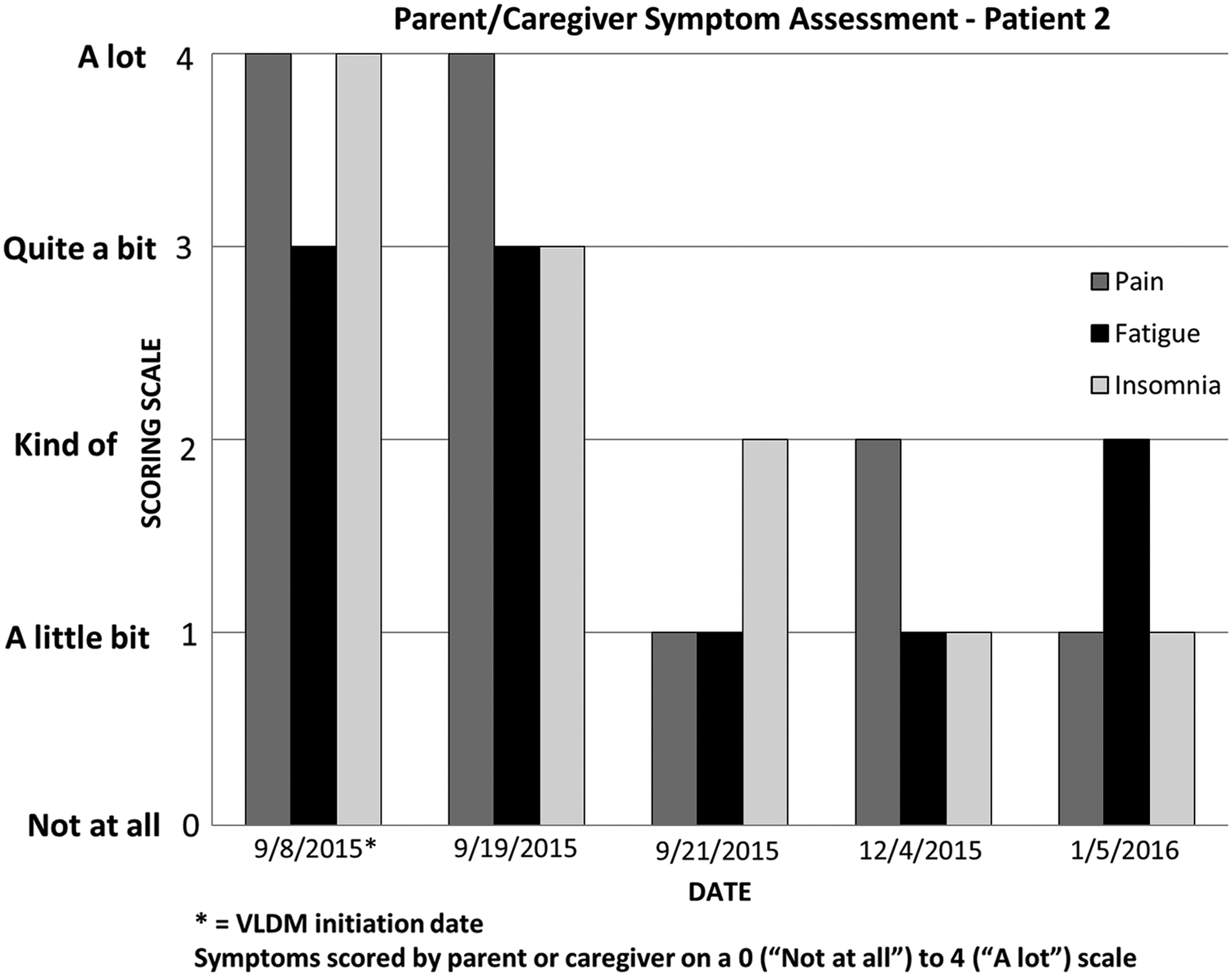
Parent/Caregiver Symptom Assessment, Patient 2: Symptoms scored by parent or caregiver on a 0 (“Not at all”) to 4 (“A lot”) scale.
With assistance from his mother, the child reported that he had pain in his cervical, lower thoracic and lumbar spine, bilateral tibia, and fibulas. The pain was unpredictable in onset, more common at night, and lasted 10–30 minutes. He and his mother reported few alleviating factors, including hot packs, cold packs, massage, acetaminophen, and morphine. The patient reported maximum pain intensity as 10/10 (Wong-Baker FACES scale) with baseline pain as 4/10. He described his pain as sharp with numbness/tingling, but no radiating pain. His mother noted that pain curtailed many activities, including sports and an inability to comfortably sit in a car for longer than two hours. Pertinent aspects of the child's physical examination included normal cranial nerves, normal muscle tone, muscle strength 5/5 in bilateral upper and lower extremities, patellar deep tendon reflexes 1+ bilaterally with no evidence of foot drop, but diminished pain and light touch discrimination at the level of the bilateral mid-tibia to feet. A diagnosis of refractory neuropathic pain was made, and VLDM was started at 1 mg po q12 hours (0.04 mg/kg/dose).
Four months after initiation of VLDM, he showed continued low scores of pain, fatigue, and insomnia (Fig. 2). His use of as-needed morphine decreased from ∼1–2 doses/24 hours in the first month of methadone therapy to none by the third month of therapy. His mother reported that 3 months after starting VLDM, he was able to tolerate a 15-hour car trip. The patient did not have any adverse symptoms, including excessive somnolence, myoclonus, or respiratory depression. One year after initiating VLDM therapy, he is on the same dose of methadone with continued good pain control (reflected in minimal as-needed morphine, and continued parent-reported low pain, insomnia, and fatigue scores). Methadone and gabapentin have not been weaned as he is still receiving vincristine.
Discussion
We describe the successful treatment of refractory neuropathic pain with the addition of VLDM to gabapentin. In both cases, the diagnosis of refractory neuropathic pain was complex. In the first child, the clustering of behavioral aspects of pain during nighttime hours initially led to a diagnosis of insomnia. It is reasonable to conclude that neuropathic pain was present during the induction phase, but insomnia related to neuropathy was only suspected after referral to PSC during the maintenance phase. Nocturnal worsening of pain is characteristic of neuropathic pain 15 and only with VLDM did these symptoms abate. In the second child, the initial lack of localization and timing of exacerbations made the diagnosis challenging. Figures 1 and 2 clearly show that the neuropathic pain syndrome in both cases was severely affecting function, as evidenced by high parent-reported scores of insomnia and fatigue. In these two patients, gabapentin alone failed to control pain and only after VLDM was added did their pain and functionality improve as reported by the parents. We did not feel that rotation from gabapentin to pregabalin was going to be beneficial, as the drugs have a similar mechanism of action. Due to its invasive nature, electromyography and nerve conduction studies are not performed in children unless there is a rapidly progressive and debilitating polyneuropathy that would lead to significant morbidity or mortality. The addition of VLDM continued to be effective and safe for months after treatment was initiated, and no evidence of opioid tolerance or adverse side effects of VLDM were observed.
Methadone is attractive for neuropathic pain in children for many reasons. Its oral bioavailability is high, estimated to be 80–90%. It is the only long-acting opioid available as a liquid, and its extraordinarily long half-life allows for a steady state that is similar to a continuous opioid infusion. This may be beneficial as the paroxysms of pain are often unpredictable in onset and duration. Finally, methadone has no active metabolites and cost is extremely low compared with other long-acting μ-opioid agonists.
Vigilance is needed to avoid toxicity as there are large variations in the pharmacokinetics. The potential of methadone to interact with other common pediatric medications metabolized via the cytochrome P450 3A4 pathway also needs to be considered. Although the frequency of a prolonged QTc interval in children and young adults receiving oral methadone is infrequent, 16 a baseline ECG to ensure a normal QTc before starting therapy would be prudent. Children whose QTc is greater than 460 milliseconds should be cautiously monitored or excluded.
As neuropathic pain tends to improve with time, periodic tapering or discontinuation of methadone and gabapentin is necessary.
Conclusion
These cases demonstrate the difficulty in assessing, diagnosing, and treating children with refractory neuropathic pain. The developmental limits of language make the diagnosis difficult, whereas a majority of pharmacologic mainstays of therapy are only readily available as tablets that cannot be swallowed by young patients. Prospective research is needed, but our findings suggest that children with refractory neuropathic pain may benefit from VLDM in a cost-conscious, effective, and safe manner.
Footnotes
Author Disclosure Statement
No competing financial interests exist.