
Abstract
Abstract
Background:
Complex decongestive therapy (CDT) is a regimen of physical treatment for lymphedema. Its effectiveness is unknown in advanced cancer patients. This study evaluates effectiveness of CDT in this population.
Method:
This is a prospective observational cohort study for 18 months of advanced cancer patients with lymphedema, who received three or more CDT interventions. Measurements were taken before the first (T1), third (T3), and sixth (T6) treatments as follows: limb volume using circumferential measurements, quality of life (QOL) using qualitative questions, skin quality using a locally developed scale measuring color, thickness, and texture. The treating physiotherapists collected data. Analysis was carried out using Microsoft Excel and SPSS.
Results:
Twelve patients, age range 42–73 years (median 69.5) were included. Survival from last recorded treatment ranged from 3 to 262 days (median 40). At T3 (n = 21 limbs), volume reduction was significant (Wilcoxin Signed Rank Test Z = −2.5, p = 0.01, r = 0.5). At T6 (n = 13 limbs), volume reduction was significant (Z = −2.4, p = 0.013, r = 0.66). At both time points, there were significant reductions in abnormal skin thickness and surface, but not color. Improvements occurred independent of volume changes. QOL changes included better function, improved limb aesthetics, and less pain and tightness.
Conclusion:
For the first time, this study shows that CDT is effective for a cohort of palliative cancer patients with limited survival. Improvements in limb volume, skin quality, and lymphedema-related QOL were recorded. Valid skin and QOL measures need to be developed. Larger, blinded trials need to be conducted to determine which patients benefit from CDT.
Introduction
L
Management is based on complex decongestive therapy (CDT), 2 which has proven effective in cancer populations without advanced disease. 7 CDT comprises skincare, exercise, compression (bandaging and/or garments), and lymphatic massage. In PC patients, reported benefits include volume reduction, improved function, and improved skin integrity,5,8,9,10 but effectiveness remains unproven.
The only systematic review found on lymphedema in PC patients 11 reported limited evidence to support CDT, based on three mixed-population studies. Our search revealed just one retrospective study specifically researching CDT in PC patients, 12 which reported effectiveness in reducing pain and dyspnea.
In PC patients, volume reduction is not always realistic. Goals of CDT may include maintenance/improvement in quality of life (QOL) or skin integrity. 13 Our pilot study, the first known, aims to measure effectiveness of CDT on limb volume, skin quality, and QOL in advanced cancer patients with lymphedema.
Methodology
A prospective longitudinal pilot study was conducted for 18 months (August 2013–January 2015) in Milford Care Centre (Limerick, Ireland). This is a specialist PC service comprising both inpatient and day units, as well as a hospice-at-home service. The edema service is provided by PC physiotherapists, trained as lymphedema therapists. Management is physiotherapy led, in consultation with medical staff as required. Ethical approval was granted by the Ethics Committee of the University Hospital Limerick in June 2013.
Population
PC patients referred to the edema service. Recruitment was conducted by the treating physiotherapists. Inclusion and exclusion criteria are outlined in Table 1.
CDT, complex decongestive therapy.
Intervention
We used an individually tailored program of CDT using a range of the following: bandaging, lymphatic massage (also known as manual lymphatic drainage [MLD]), compression garments, kinesiotaping, exercise, deep breathing techniques, education, and skincare.
Outcome measures
Measurements were recorded by the treating physiotherapist before the initial treatment (T1), before the third (T3) and sixth (T6) treatments.
Limb volume
The gold standard is circumferential measurement of limbs.14,15 Measurement points were as follows:
Arm: knuckles, styloid process, elbow crease, 10 cm above elbow.
Leg: base of fifth metatarsal, around malleoli, widest point of calf, tibial tuberosity, 10 cm above tuberosity, 20 cm above tuberosity.
Volume was calculated using truncated cone measurements
16
:
h = segment length (between measurement points)
C and c are circumferences at each end of segment.
Difference in volume (mL):
Skin changes
Our lymphedema team clinically reports skin changes post-CDT in three domains: color, thickness, and surface. A suitable clinical tool was not found, therefore, one was developed to measure abnormalities in these domains (Appendix Table A1). Reliability and validity studies have yet to be conducted. Inter-rater reliability was not a factor.
QOL changes
The Lymphadema Quality of Life Questionnaire (LYMQOL) 17 was chosen, the shorter of two lymphedema-specific QOL tools available. However, the first three patients required assistance to complete, thereby rendering results invalid. Thereafter, two qualitative questions were asked of subsequent patients at T3 (n = 9) and T6 (n = 5).
“Have you noticed any changes since receiving the lymphedema treatment?”
“If so, what changes have you noticed?”
Data analysis
Results were filled out by the treating physiotherapist on paper and transferred to a password-secured Microsoft Excel sheet. Statistical analysis used Excel and SPSS. Qualitative information was analyzed using thematic analysis. 18
Results
In 18 months, there were 141 new referrals to the edema service, 17 agreed to participate in the study, 12 were included for analysis after attrition (Fig. 1). All had advanced cancer, median survival 40 days from final treatment (Table 2). At T3, 12 patients (21 limbs) were included, and at T6, 6 patients (13 limbs) were included. CDT comprised a variety of interventions (Fig. 2).

Recruitment.
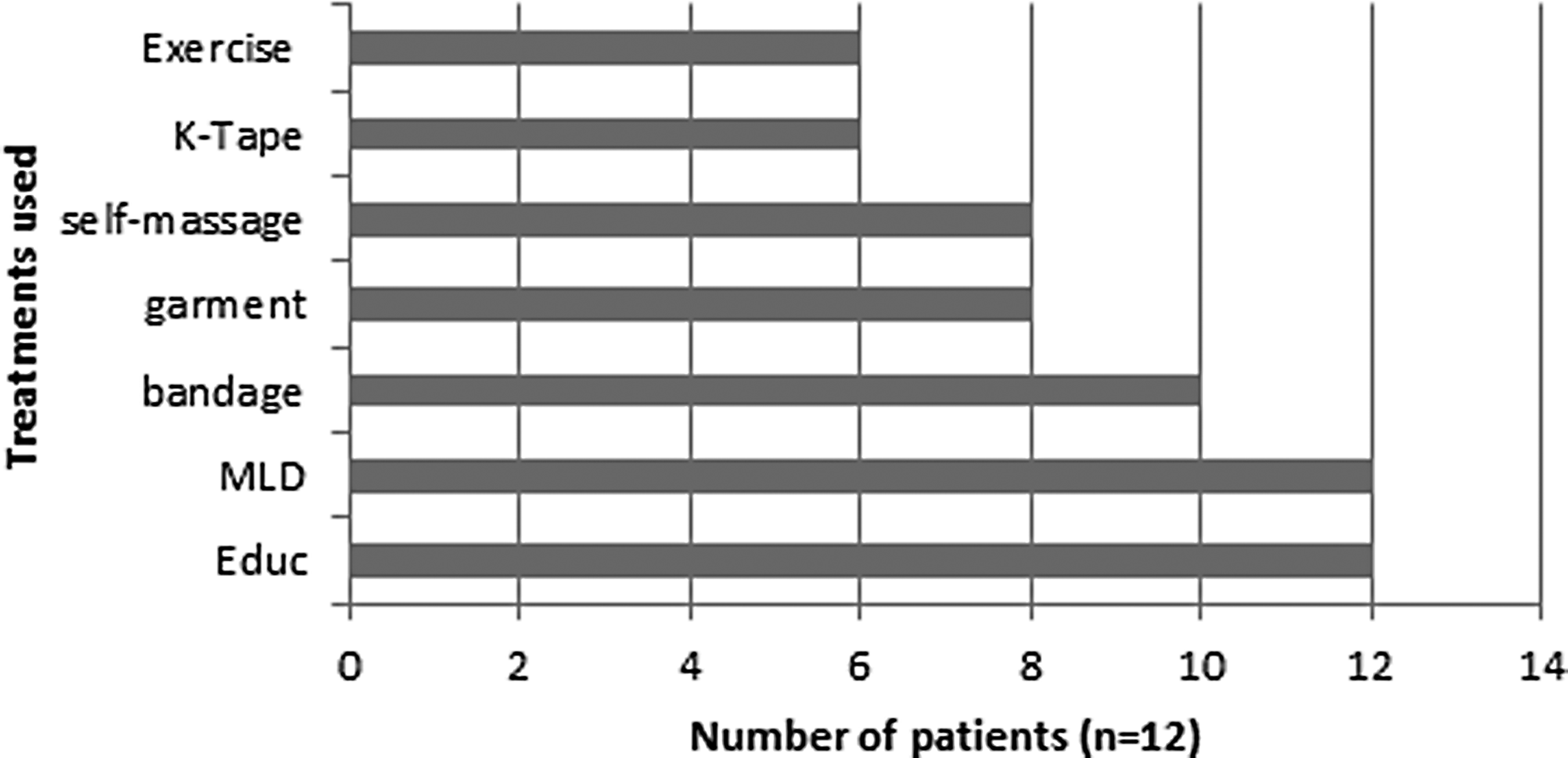
Treatments used as part of CDT.
Volume reduction
At T3: 16/21 limbs reduced in volume, median reduction was 443 mL (5.3% volume). Wilcoxin Signed Ranks Test showed significant change (Z = −2.5, p = 0.01, r = 0.5). At T6, 11/13 limbs reduced in size, median reduction was 658 mL (9%), which was significant (Z = −2.4, p = 0.013, r = 0.66). See Table 3. There was no correlation between volume reduction and survival at T3, but a strong correlation at T6 (Pearson's correlation coefficient r = −0.7, p = .001).
Negative values show reduction in volume.
Skin changes
Post-CDT, abnormal skin color did not change (Fig. 3). Skin thickness reduced significantly at T3 (Wilcoxin Signed Rank Test Z = −3.354, p = 0.001, r = 0.73) and at T6 (Z = −3.247, p = 0.001, r = 0.9). Surface abnormalities reduced significantly at T3 (Z = −2.71, p = 0.007, r = 0.6) and T6 (Z = −2.55, p = 0.011, r = 0.71). Changes occurred with and without volume reduction. No correlation was found using Pearson's product between skin improvement and extent of volume reduction at T3 or T6.
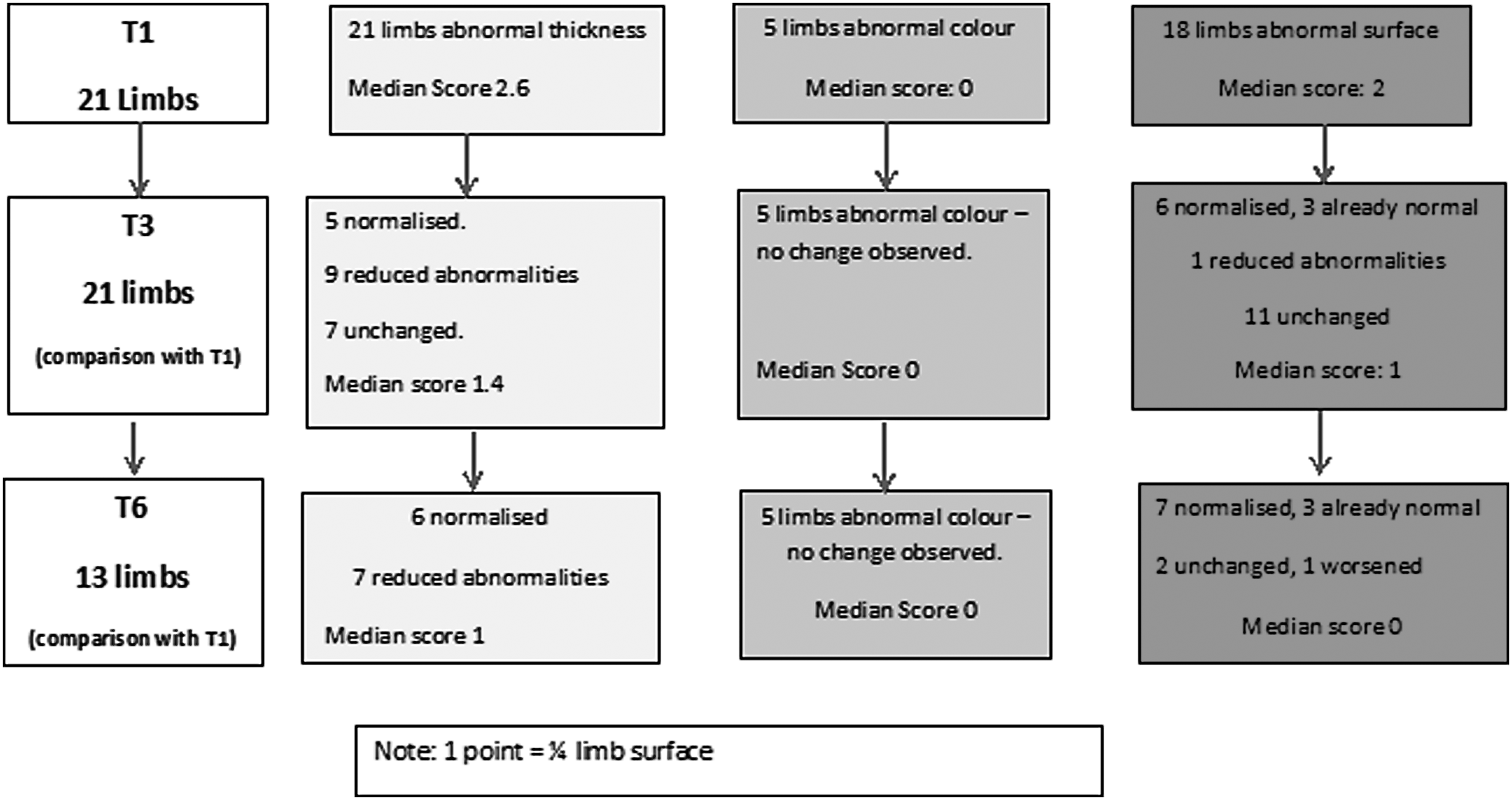
Skin changes at T3 and T6.
Quality of life
A total of 9 of 12 subjects were asked about changes post-CDT. At T3, all nine reported positive changes, one of whom had worsening edema.
The most common theme was symptom improvement. Patients reported reductions in pain/tightness, more comfort, feeling looser, lighter, and skin was softer.
“My tummy feels lighter. It's easier to breathe.”
The patient with worsening edema also reported reduced pain and tightness.
The second most common theme was functional improvement. It was easier to move, walk, and to do specific tasks.
“I can use my mobile phone again.”
Lastly, changes to bodily appearance were reported. Limbs were smaller, bony areas emerged, and a sense of normalcy returned. It was easier to apply clothing/shoes.
“It looks like a lady's leg again.”
At T6, five of six remaining patients were questioned about reported changes. The mentioned themes were reiterated, however, one subject, with worsening lymphedema, noticed that applying clothing was harder.
Discussion
The benefits of CDT for lymphedema are well established in cancer survivors, but not in PC patients. This study, the first known, observed the effects of individually tailored CDT in a convenience sample of 12 PC cancer patients with limited survival.
In general, CDT was well tolerated, being discontinued once the burden outweighed the benefits. There was attrition of five patients before T3, and five patients before T6. There was predominance of lower limb lymphedema (21 legs, 2 arms), concurring with two previous studies.19,20
Limb volume
At both time points, there was statistically significant median reduction in volume. The extent of volume reduction was not linked at T6, in that those with larger reductions had longer survival times. Results suggest that patients with limited survival can achieve volume reduction with CDT, and that some may benefit more than others.
Skin quality
The biggest issue in recording changes to skin quality was lack of a suitable measurement tool, as reported previously. 13 Our tool, although not yet validated, showed improvements in texture and surface of skin, but not color (Fig. 3). Improvements did not correlate with volume reduction and even occurred when limb volume increased. This suggests that CDT may be worthwhile in PC patients for improving skin integrity, even without expected volume change.
Lymphedema-specific QOL
Improving QOL is a major goal of treating lymphedema in PC patients. 13 Measurement remains a challenge, as existing lymphedema-specific tools proved unsuitable.Our qualitative questions, introduced ad hoc, had no research to guide them. In particular, our questions did not allow for emotional responses to treatment, treatment burden, or for broader themes to emerge. However, valuable information was elicited: CDT reduced discomfort, improved function and limb aesthetics, and there was a return toward normalcy.
These findings prompt the development of a lymphedema-specific QOL tool for PC patients. Qualitative research is needed on the experience of CDT in PC patients to guide this.
Limitations and suggestions
Our pilot study has a number of limitations, which should be addressed by future studies. Clinical tools to measure both skin integrity and lymphedema-specific QOL need to be developed, while keeping patient burden to a minimum.
We used a convenience sample of patients, and sample size was small. Larger studies would allow for more rigorous statistical analysis of effectiveness. The treating physiotherapists both recruited and recorded results; therefore, gatekeeping and bias toward reporting good effects were possibilities. Independent recruitment and blinding of researchers are obvious requirements for future studies.
This study was pragmatic, with varying treatment regimens and time frames, which could be standardized in future trials. It would be beneficial to note albumin levels and physical function at initial time point to determine whether these affect volume reduction or predict completion of program.
Despite these limitations, results suggest that advanced cancer patients with limited survival may obtain multiple benefits from CDT.
Conclusion
Lymphedema management of PC patients using CDT has no research to prove its effectiveness, despite widespread clinical use. This prospective pilot study, the first known, evaluates the effects of CDT on lymphedema in patients with advanced cancer and with poor survival. The biggest obstacle was lack of valid tools to evaluate changes in lymphedema-specific QOL and skin quality. Volume reductions occurred in this population and skin quality improved. QOL improvements included increased function, symptom reduction, and normalization of limb aesthetics. Further research is warranted.
Footnotes
Acknowledgments
The authors thank their physiotherapy colleagues, who assisted with data collection. They also thank Dr. Jean Saunders (University of Limerick) for statistical advice and to Dr. Judy Pettigrew (University of Limerick) for her advice on qualitative analysis.
This article was presented in abstracts at the 9th World Research Congress of the European Association for Palliative Care, Palliat Med, June 2016, vol. 30, no. 6, NP83.
Author Disclosure Statement
No competing financial interests exist.
| Skin condition: (1) <25%, (2) 25–49%, (3) 50–74%, (4)>75% |
T1 | T3 | T6 |
|---|---|---|---|
| Color: normal, red, pink, brown (%) | |||
| Thickness: normal, thin, pitting edema, nonpitting (hard) (%) | |||
| Surface: normal, dry, shiny, hyperkeratosis, lymphoceles, papillomatosis, lymphorrhea (%) |