
Abstract
Abstract
Background:
Actions in preparation for death and talks about death between advanced cancer patients and their families are considered essential to achieve a good death. However, little is known about the prevalence of such actions compared with talks and their association with bereaved families' psychological morbidity.
Objective:
To clarify the prevalence of bereaved families having acted in preparation for death and talked about death with their loved one, and to explore their associations with bereaved families' depression and complicated grief (CG).
Design:
A nationwide survey.
Setting/Subject:
A total of 999 bereaved families of cancer patients admitted to 133 inpatient hospices in Japan.
Measurements:
The prevalence of families' actions in preparation for and talks about death, Patient Health Questionnaire (PHQ)-9, and Brief Grief Questionnaire (BGQ).
Results:
Among 678 bereaved families (response rate = 68%), 513 (76%) acted in preparation for death, and 315 (46%) talked about death with their loved one. Those who acted and talked were significantly less likely to suffer depression (PHQ-9 ≥ 10) than those who neither acted nor talked (odds ratio [OR], 0.405; 95% confidence interval [CI], 0.195–0.845; adjusted p = 0.016). Families who acted were significantly less likely to suffer complicated grief (CG; BGQ ≥8), whether they talked (OR, 0.394; 95% CI, 0.185–0.84; adjusted p = 0.016) or not (OR, 0.421; 95% CI, 0.191–0.925; adjusted p = 0.031).
Conclusions:
Most families acted in preparation for death, and those who acted were less likely to suffer depression and CG. Clinicians may minimize families' later psychological morbidity by helping patients and families act in preparation for death.
Background
A
Recent observational studies have shown the beneficial effects of end-of-life (EOL) discussions with advanced cancer patients not only on patients' quality of life and quality of care but also on bereaved families' mental health.6,7 Population-based studies have also revealed that families who had talked about death with their loved ones dying of cancer had better preparedness for the moment of death, whereas families who had not talked about death and who had not been able to spend as much time as they wished with their loved ones had a higher risk of feeling guilt or regret.8,9 Several guidelines recommend EOL discussions with advanced cancer patients.10–12 In addition to EOL discussions, actions in preparation for death (e.g., spending enough time, seeing people whom one wants to see, repairing relationships, having finances in order, and making funeral arrangement) have been considered essential components of a good death.1–5 Such actions could lead to achieving a good death and potentially result in better mental health for family members, irrespective of whether or not patients and their families have talked about death. Nonetheless, to the best of our knowledge, no study has systematically explored the prevalence of actions in preparation for death compared with that of talks about death with their loved one. Furthermore, although greater perception of preparedness for death has been shown to be associated with less depression and/or complicated grief (CG) among bereaved families,13–17 little is known about whether actions in preparation for death and/or talks about death, modifiable behaviors based on such preparedness, are associated with bereaved families' psychological morbidity.
Thus, the primary aim of the present study was to clarify the prevalence of bereaved families having acted in preparation for death compared with them having talked about death with their loved one. Our secondary aim was to preliminarily explore the associations between whether or not bereaved family members had acted in preparation for death and/or talked about death with patients and their depression and CG.
Methods
This study was conducted as a part of the Japan Hospice and Palliative Care Evaluation (J-HOPE)-3 study, a cross-sectional, anonymous, self-report questionnaire survey. 18 The detailed methodology of this survey was described elsewhere.18,19 In brief, the main study took place between May and July 2014, and included bereaved family members of cancer patients who had died in 133 inpatient hospice/palliative care units (PCUs).
Participants
This study included a subpopulation of the main study: bereaved family members of cancer patients who had died in 133 PCUs. Potential subjects were bereaved family members of cancer patients who died before January 2014 in each of the participating institutions. In Japan, PCUs are involved in ∼10% of all cancer deaths. 20 The inclusion criteria included the following: (1) the patient died of cancer; (2) the patient was aged 20 years or older; (3) the patient had been admitted to a PCU for more than three days; and (4) the bereaved family member was aged 20 years or older. The exclusion criteria were as follows: (1) the bereaved family member could not be identified; (2) the potential participant would have had serious psychological distress, as determined by the primary physician and a nurse; and (3) the potential participant was incapable of completing the self-reported questionnaire because of cognitive impairment or visual disability.
Procedure
The questionnaires for the present study were randomly sent to the bereaved family members identified by each participating institution. The return of a completed questionnaire was considered consent to participate in the study. A reminder was sent to nonresponders one month after the questionnaire had been sent out. The ethical and scientific validity of the study was approved by the institutional review board of all participating institutions.
Measurements
The questionnaire for this study was developed by the authors on the basis of a systematic literature review, interviews with 11 bereaved family members before the survey, and extensive discussions among the authors.1–5,21–27 The questionnaire included patient's and family's background characteristics; the presence or absence of actions in preparation for death and talk about death; examples of such actions; the Patient Health Questionnaire (PHQ)-9; and Brief Grief Questionnaire (BGQ). Due to the lack of previously validated instruments with respect to actions in preparation for death and talk about death, these endpoint parameters were developed by the authors in similar ways to previous surveys.1–5,21 Content validity was confirmed by pilot testing. The primary endpoint was the prevalence of bereaved families having acted in preparation for death, compared with them having talked about death with their loved one.
Actions in preparation for death
“Actions in preparation for death” was defined as something done or performed by families to help achieve a good death of their loved one based on explicitly or implicitly shared understanding of terminal awareness.1–5,27 The questionnaire asked the family members: “Have you acted in preparation for death?” The response categories were “never,” “acted a little,” “acted,” and “acted a lot.” The latter three responses were considered as having acted in preparation for death. To clarify the nature of actions, we showed the following examples and asked if these actions had been taken: “increased the time spent with the patient (e.g., being together at home or in a hospital room, and traveling)”; “repaired relationship with the patient”; “helped the patient meet those who s/he wanted to meet”; and “asked what the patient wanted after his/her death, such as funeral arrangements and financial affairs.”1–5,27
Talk about death
“Talk about death” was defined as conversations between the dying patient and his/her family about the impending death based on previous studies.1,4,21 The questionnaire asked the families: “Have you explicitly talked about death with the patient?” 21 The response categories were “never,” “talked a little,” “talked,” and “talked a lot,” and the latter three responses were considered as having talked about death.
Patient Health Questionnaire-9
The PHQ-9 is a widely accepted, valid, and reliable self-report tool that consists of nine items to measure the severity of depression.28–30 The Japanese version of the PHQ-9 has been validated. 31 Each item concerns the extent to which a particular depressive symptom has bothered the respondent in the preceding two weeks. Responses are provided on a four-point Likert scale ranging from 0 (not at all) to 3 (nearly every day), with total scores ranging from 0 to 27. A total score of 10 or greater is positive for moderate/severe depression. 28 We have decided to consider participants with PHQ-9 scores ≥10 as those having depression.
Brief Grief Questionnaire
The BGQ is a validated self-report tool to detect CG. 32 The BGQ consists of five items with a CG-related status (difficulty accepting the death of a loved one; grief interfering with life; troubling images or thoughts about the death; avoiding things related to the deceased; feeling cut off or distant from other people). Each item is evaluated on a three-point Likert scale ranging from 0 (not at all) to 2 (a lot), with total scores ranging from 0 to 10. A total score of 8 or higher indicates that the respondent is likely to develop CG, scores of 5–7 indicate subthreshold CG, and scores of <5 indicate that the respondent is unlikely to develop CG. The Japanese version of the BGQ was validated previously. 33 In this study, participants with BGQ scores ≥8 were defined as having CG.
Statistical analyses
We used descriptive statistics to summarize the participants' background, and calculated the rates of their responses. We also conducted chi-square analyses and t tests for categorical and continuous variables, respectively. When comparing PHQ-9 and BGQ scores, we made adjustments using demographic factors that have previously been shown to contribute to postbereavement depression and CG (i.e., patient's age, sex, primary cancer site, marital status, living situation, and annual income; bereaved family's age, sex, relationship with the patient, education, social support, and religion).15,16,34–46 Finally, we conducted analyses of variance to explore the associations between the levels of actions in preparation for death and the PHQ-9 and BGQ scores.
Assuming that 50–70% would have had acted in preparation for death or talked about death, 559–666 subjects would be sufficient to calculate an accuracy to within a 10% width with 99% confidence intervals (CIs).
We conducted all statistical analyses using SPSS version 21.0 (IBM Japan Institute, Tokyo, Japan). p < 0.05 was considered significant in all analyses.
Results
A total of 999 bereaved family members from 133 PCUs were included. Of them, 750 bereaved family members returned the questionnaire, and 72 refused to participate. Thus, responses from 678 participants were analyzed (response rate, 68%). The mean length between the day of death and the day when the first questionnaire was sent was 236 (standard deviation, 102) days. The characteristics of the deceased patients and bereaved family members are summarized in Table 1.
Values are mean ± standard deviation, or n (%). Total percentages do not equal 100% because of missing values.
SD, standard deviation.
Prevalence of actions in preparation for death and talks about death
In total, 513 (76%) participants acted in preparation for death, while 115 (17%) did not (Fig. 1). On the contrary, a total of 315 (46%) participants talked about death to a varying extent with the patient, while 332 (49%) did not (Fig. 1). With respect to contents of actions, 432 (64%) participants “increased the time spent with the patient (e.g., being together at home or in a hospital room, and traveling)”; 397 (59%) “helped the patient meet those who s/he wanted to meet”; 237 (35%) “asked what the patient wanted after his/her death, such as funeral arrangements and financial affairs”; and 201 (30%) “repaired the relationship with the patient.”
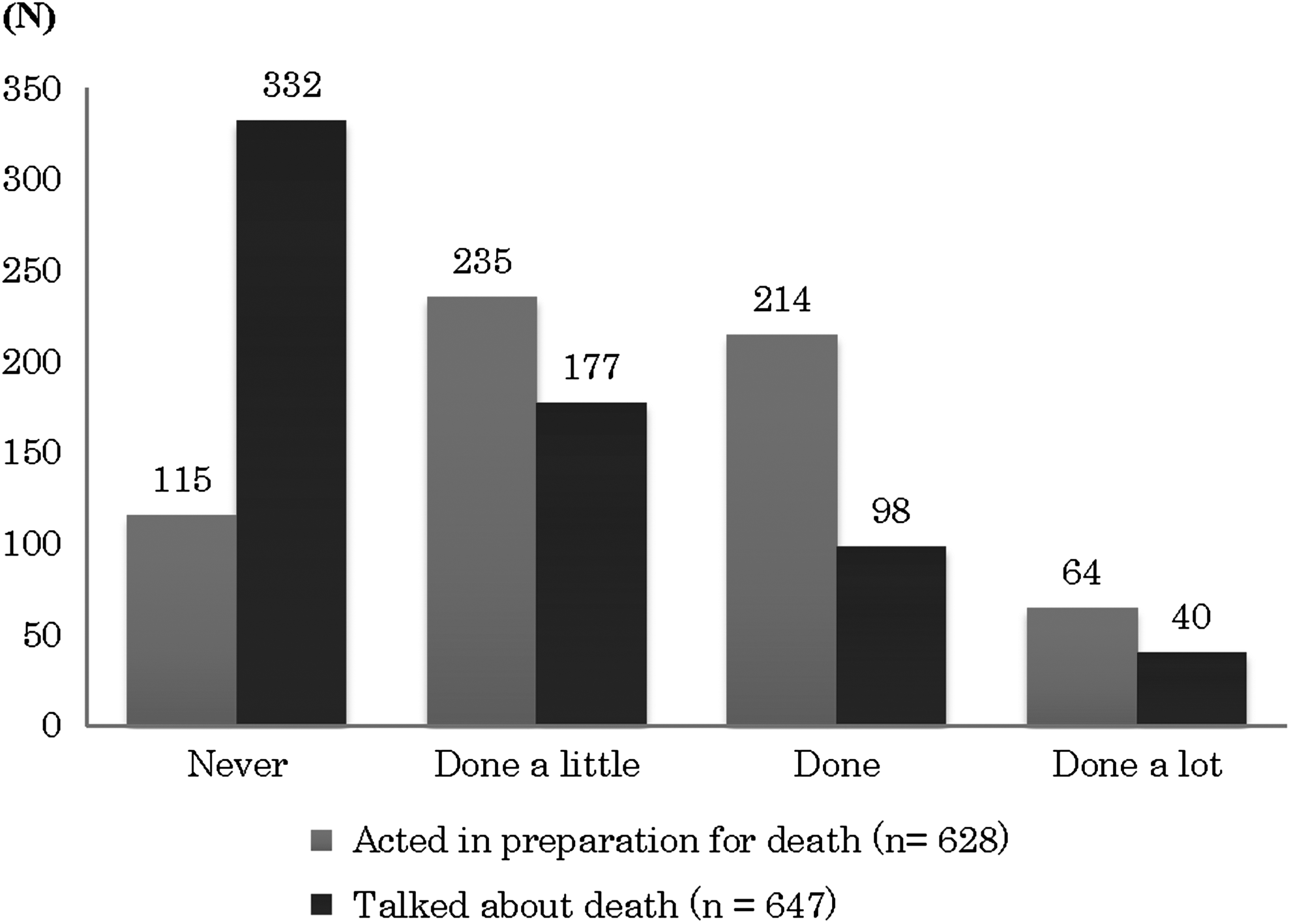
Prevalence of bereaved family members' having acted in preparation for death and talked about death with the patient.
Associations between actions/talks and depression/grief
Table 2 summarizes the associations between whether or not bereaved family members had acted in preparation for death or talked about death and the prevalence of depression or CG. Bereaved families who had acted and talked were significantly less likely to suffer depression compared with those who had neither acted nor talked (odds ratio [OR], 0.405; 95% CI, 0.195–0.845; adjusted p = 0.016). Those who had not acted but talked were the most likely to suffer depression (OR, 1.897; 95% CI, 0.682–5.28; adjusted p = 0.220); and families who had acted were significantly less likely to suffer CG, whether they had talked (OR, 0.394; 95% CI, 0.185–0.84; adjusted p = 0.016) or not (OR, 0.421; 95% CI, 0.191–0.925; adjusted p = 0.031) compared with those who had neither acted nor talked. Those who had not acted but talked were the most likely to suffer CG, although the prevalence was not significantly different from that in those who had neither acted nor talked (OR, 1.252; 95% CI, 0.429–3.651; adjusted p = 0.681).
Total percentages do not equal 100% because of missing values. Acted: sum of “acted a little,” “acted,” and “acted a lot” in preparation for death. Talked: sum of “talked a little,” “talked,” and “talked a lot” about death.
p-Values were adjusted for the following demographic factors: patient's age, sex, primary cancer site, marital status, living situation, and annual income; bereaved family's age, sex, relationship with the patient, education, social support, and religion.
BGQ, Brief Grief Questionnaire; CI, confidence interval; OR, odds ratio; PHQ-9, Patient Health Questionnaire-9; Ref, reference.
Overall, higher levels of actions in preparation for death were significantly associated with lower PHQ-9 (p < 0.001) and BGQ scores (p = 0.002) (Figs. 2 and 3).
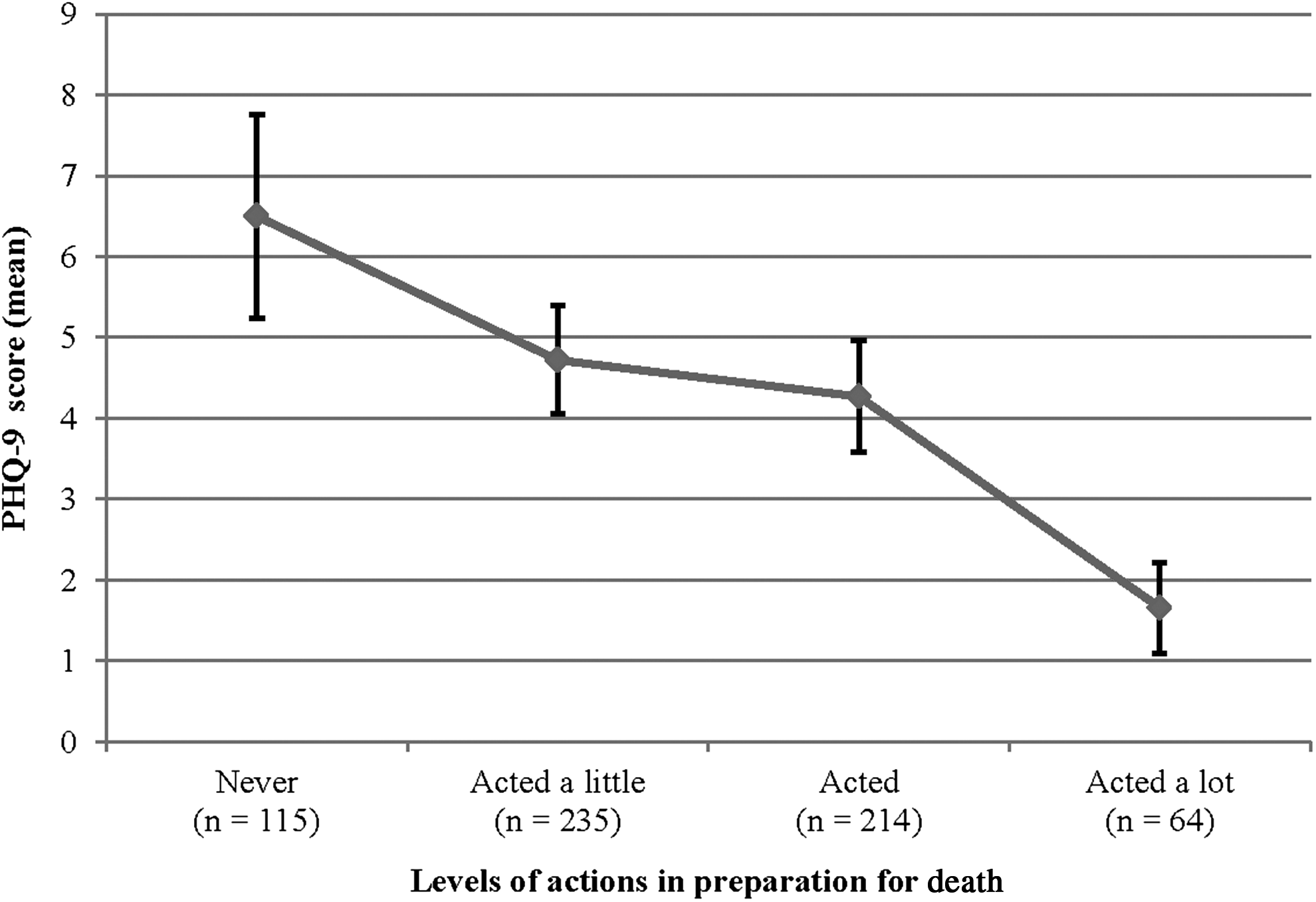
PHQ-9 scores of bereaved family members with various levels of action in preparation for death. Bars indicate 95% confidence intervals. PHQ-9, Patient Health Questionnaire-9.
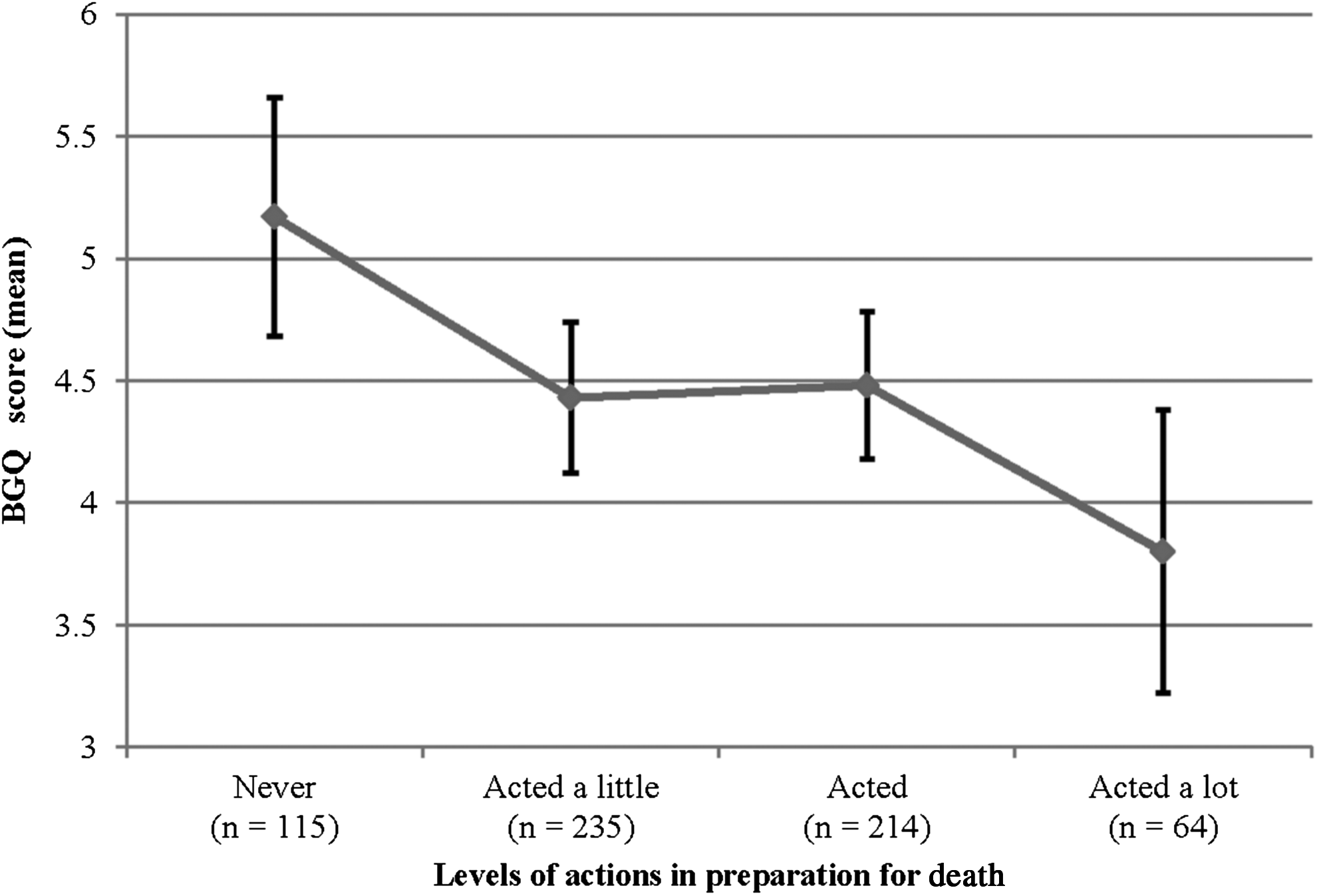
BGQ scores of bereaved family members with various levels of action in preparation for death. Bars indicate 95% confidence intervals. BGQ, Brief Grief Questionnaire.
Discussion
The present study is, to the best of our knowledge, the first study to clarify the prevalence of bereaved family members having acted in preparation for death, in addition to the prevalence of them having talked about death with their loved one; and it explored the associations between such actions and talks and their depression and CG. We generated several important findings.
The first and most important finding is that bereaved family members who had acted in preparation for death and talked about death were less likely to suffer depression, and those who had acted were less likely to suffer CG, compared with those who had neither acted nor talked. These findings are in line with previous studies showing that bereaved families who felt more prepared for their loved one's death and/or were able to spend as much time as they wished with their loved one had a lower risk of later experiencing depression, CG, and negative emotional reactions after his/her death.9,13–17 Actions are part of nonverbal communications, which could well complement verbal communication. 47 The potential interpretation of our finding is that families who acted might have been able to communicate what talking about death alone could not convey. In contrast, those who did not act might have had some conflicting situations that had prevented such nonverbal communications, which could be associated with later negative emotional reactions. Overall, these may indicate that taking actions in preparation for death, in addition to talking about death, is vital for bereaved family members from the viewpoint of their psychological morbidity.
The second important and novel finding is that bereaved family members had more frequently acted in preparation for death (76%) than explicitly talked about death with their loved one dying of cancer (46%). While the previous nationwide studies showed the bereaved family-perceived importance of actions in preparation for death as an essential component of a good death, the overall prevalence of such actions had never been elucidated.1–5 Our results can be explained by the previous finding that terminally ill patients were less likely to want to talk about the meaning of death as death approached. 4 Other potential interpretations of the higher prevalence of actions than talks are that the families may have tried to help their loved one achieve a good death by engaging in actions while protecting them from an explicit awareness of an impending death, and that families might have difficulty talking about death.2,3 Of interest is that almost half of bereaved families had not talked about death with their loved one at all. EOL discussions among patients and families as well as clinicians are internationally recommended,10–12 and the lack of EOL discussions could hinder shared decision making and appropriate advance care planning, which may lead to poor quality of care and quality of dying of patients. On the contrary, one could hypothesize that patients and their families might feel that a good death is achievable by acting in preparation for death with or without explicitly talking about death. Future studies should explore the impact of actions in preparation for death and talks about death on shared decision making, advance care planning, quality of EOL care, and quality of dying (e.g., life completion) of patients.
Clinical implications
Although having EOL discussions are generally recommended among terminally ill cancer patients and their families, our findings suggest that taking actions in preparation for death are also important for families. Our findings may be applicable not only in other Eastern countries where many patients, families, and clinicians feel reluctant to explicitly discuss EOL issues48,49 but also in Western countries where patients' and families' preparation for death is considered as important for a good death.1,4,5 Clinicians may minimize family members' later depression and CG by helping them fully act in preparation for death, whether or not the families have explicitly talked about death with their loved one.
Study limitations
Despite the strengths of the nationwide survey, our study has several limitations. First, this is a survey among bereaved family members with a moderate response rate (68%) conducted after an average of eight months of patients' death, which may have introduced both selection and response biases. We believe that this limitation is justifiable, as previous national surveys from U.S. and Japanese bereaved family members also reported similar response rates and intervals after death.1,50 Second, there may have been social desirability bias with a tendency for respondents to overreport having acted in preparation for death. Third, although we operationalized “actions in preparation for death” and “talks about death” based on prior literature, we performed no formal testing of the validity and reliability of these measurements.
In conclusion, this nationwide survey revealed that most bereaved family members of cancer patients had acted in preparation for death, and that those who had acted were less likely to suffer depression and CG. Clinicians may minimize family members' later psychological morbidity by helping patients and families fully act in preparation for death.
Footnotes
Acknowledgments
This study was conducted with the cooperation of Hospice Palliative Care Japan (HPCJ). The authors thank all participants and participating institutions for taking part in this study. This study was part of the J-HOPE Study, funded by Japan Hospice Palliative Care Foundation, and, in part, supported by Japan Society for the Promotion of Science KAKENHI Grant Number JP16K15418.
Author Disclosure Statement
The authors declare that there is no conflict of interests.
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.