
Abstract
Abstract
Background:
It is unknown how many hospice enrollees elect to be full code and if this is associated with higher hospice live discharge rates.
Objective:
To measure the rates of hospice enrollees electing full code, the characteristics predicting full code status, and the association of full code status with various hospice live discharge patterns.
Design:
Retrospective cohort study of electronic medical record data.
Setting/Subjects:
A total of 25,636 decedents enrolled in two Michigan hospices between 2009 and 2014.
Measurements:
Code status was defined as full code versus do-not-resuscitate (DNR) orders. Covariates include demographics, location (home, hospice facility, nursing home, and hospital), primary diagnosis, and length of stay. Hospice live discharge was defined as short (0–14 days), medium (15–179 days), and long (>179 days).
Results:
A total of 12.9% of hospice enrollees elected full code status. This was significantly (p < 0.05) predicted by male sex, younger age, nonwhite race, home setting of care, and cancer diagnosis. Those with full code status had 1.76 times the adjusted odds of hospice live discharge compared with those with DNR orders (95% confidence interval [CI] 1.44–2.16) and 2.47 times the odds of short live discharge (95% CI 1.69–3.62) with no significant difference in long live discharge. The association of full code orders with hospice live discharge was stronger for nonwhite enrollees, with a live discharge rate of 23.8% versus 11.6% for African Americans with full code versus DNR orders.
Conclusions:
Those electing full code status on admission to hospice are at high risk of live hospice discharge after short enrollments, particularly nonwhite enrollees.
Background
D
One consequence of the PSDA is that individuals electing to forego curative treatments through the Medicare hospice benefit may simultaneously elect full code status. It is unknown how many hospice enrollees currently elect full code status, how they make this decision, and how full code status affects their clinical course. Two studies from 2007 indicated that ∼20% of hospice patients had full code orders in place,5,6 but the landscape of hospice has shifted dramatically in the last decade. 7 One single-site study found that full code status was independently associated with longer hospice length of stay. 8 However, another study found the opposite result: completion of advance directives as a whole at the initiation of hospice has been associated with longer hospice length of stay and lower likelihood of inpatient death, although the content of advance directives was not assessed. 9
The paradox of not only electing full resuscitation but also electing a comfort-focused care plan through the hospice benefit may indicate a gap in patient understanding or decision-making support. One signal for problematic decision making in hospice enrollment is hospice live discharge, 10 which occurs in approximately one in five hospice enrollees.11,12 While the majority of hospice live discharges occur due to the patient's condition stabilizing, in nearly 20% of cases, the patient/family decides to pursue more aggressive treatment or to leave hospice care for other reasons (termed hospice revocation), 13 with hospice discharge to pursue life-prolonging therapies more common in African American patients. 14 Two separate studies have demonstrated that one-third of patients discharged from hospice die within the next 6 months,15,16 indicating that for many, continued hospice care might have been beneficial. Hospice live discharge is predicted by longer length of stay,13,17 nonwhite race, and specific diagnosis such as dementia (for live discharge after long hospice stay) or heart failure (for discharge after shorter hospice stay). 11 Hospice live discharge has been described as an experience of suffering and abandonment by family members and patients. 18
This study aims to describe the rates and predictors of DNR orders in hospice. In addition, we aim to assess if the absence of DNR orders is associated with higher live discharge rates to evaluate the potential of absent DNR orders at hospice enrollment as a trigger for further research and support.
Methods
Study design and sample
We relied on data sourced from the electronic medical records of two Michigan nonprofit hospices. This study included individuals enrolled in hospice between January 1, 2009, and December 31, 2014. Individuals were excluded if there were no complete data for whether they were DNR orders or full code as this was due to an electronic medical record data entry error. The study was determined to be exempt from review by the University of Michigan Institute Research Board.
Measures
Outcome variables
The presence of DNR orders was captured from a data field within the electronic medical record. This was defined as both finalized DNR orders (signed by the attending physician as well as patient/family) and DNR orders that were signed by the patient/family, but awaiting attending physician signature.
Hospice live discharge was categorized by the length of stay preceding discharge: short (0–14 days), medium (15–179 days), and long (>179 days), as has previously been done in the hospice live discharge literature. 11 This method differentiates between short hospice discharges that are more likely to occur because of patient/family preferences for aggressive care or dissatisfaction with hospice versus long hospice discharges that are more likely to occur because the patient's health improves or stabilizes.
Independent variables
Covariates extracted from the electronic medical record included sex, age, race, diagnosis at admission to hospice, location at admission to hospice (home, hospital, nursing home, residential hospice facility), year, and medical condition listed as indication for hospice enrollment. Medical conditions were then categorized as cancer, lung disease, dementia/failure to thrive, heart disease, neurologic conditions (including stroke, multiple sclerosis, and amyotrophic lateral sclerois), sepsis or infectious conditions, renal disease, gastrointestinal or hepatic disease, and other.
Analyses
Descriptive statistics were used to characterize the demographic, illness, and hospice stay characteristics of those in hospice with and without a DNR order. A multivariable logistic regression model measured the association of these variables with DNR versus full code order. A multivariable logistic regression model then examined the association of all characteristics as well as DNR orders with overall live discharge as well as very short, short, medium, long, and very long live discharge. All models used robust standard errors that adjusted for clustering of patients within hospices. All analyses were done in Stata, version 14 (StataCorp, College Station, TX).
Results
A total of 25,636 Michigan hospice enrollees between 2009 and 2014 were included in the study, with an additional 2497 excluded due to missing DNR status. A total of 12.9% of hospice enrollees elected full code orders.
As demonstrated in Table 1, those with full code orders were more likely to be male (49.8% vs. 42.8%, p < 0.001), younger (mean age of 71.54 years vs. 80.35 years, p < 0.001), African American (15.7% vs. 5.7%, p < 0.001), with cancer diagnoses (53.1% vs. 37.2%), and residing at home (80.5% vs. 63.0%, p < 0.001). In the adjusted logistic regression analysis model, including other covariates (Table 2), we see that all tested covariates predict full code status, with the exception of there being no significant difference between full code election between whites and those reporting their race as neither white nor African American.
DNR, do-not-resuscitate.
Models adjusted for all other covariates as well as year.
Natural log of age.
Ref, reference.
Table 3 demonstrates the difference in odds of any live discharge and live discharge by type (short, medium, or long) as predicted by full code status and all other covariates. While full code status was associated with overall higher rate of live discharge (adjusted odds ratio [AOR] 1.76, 95% confidence interval [CI] 1.44–2.16), this effect was strongest for short discharges occurring within 14 days after hospice enrollment (AOR 2.47, 95% CI 1.69–3.62) with no significant association of full code status and long discharges occurring 180 or more days after hospice enrollment (AOR 1.18, 95% CI 0.65–2.17). Similarly, there are very different patterns of other predictors and short versus long live discharge. Dementia is associated with greater odds of long discharge versus cancer (AOR 6.39, 95% CI 3.23–12.63), but no difference in short discharge. Hospital setting was associated with higher odds of short discharge (AOR 1.22, 95% CI 1.02–1.46), but lower odds of long discharge (AOR 0.04, 95% CI 0.01–0.17). Figure 1 demonstrates the predicted adjusted rates of short, medium, and long live discharges for those with full code versus DNR orders.
Adjusted rate of live discharge for hospice enrollees with full code versus do-not-resuscitate (DNR) orders for total population and by race. Black = full code; striped = DNR. Adjusted for age, sex, disease (cancer, dementia, or other), location of care (home, hospital, nursing home, or hospice), and year.
Data source: electronic medical record data from two nonprofit hospices, 2009–2014. Models also include an interaction term between race and full code status.
Age is in 10-year units.
AOR, adjusted odds ratio; CI, confidence interval.
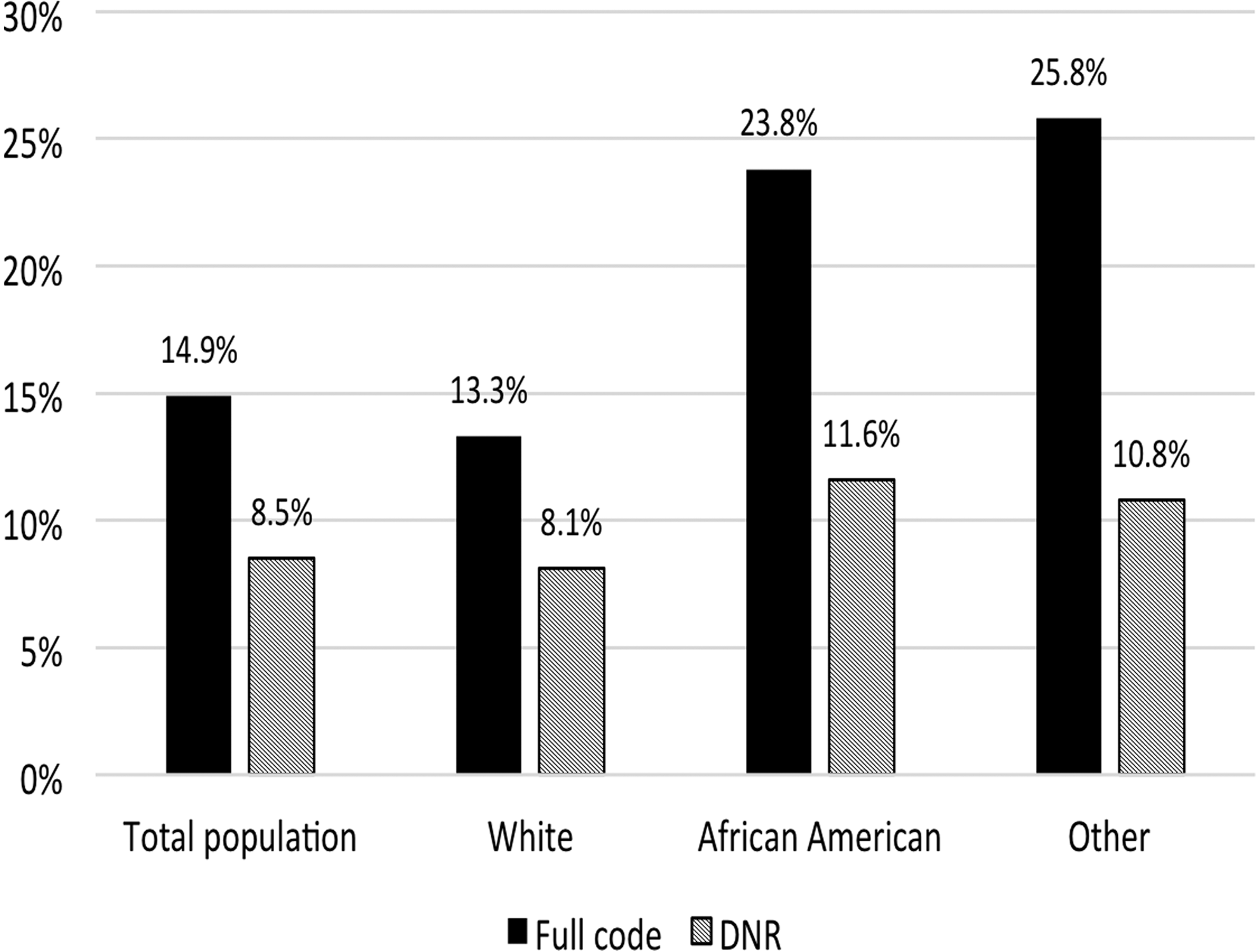
Testing for interactions revealed a significant interaction of race with full code status in predicting live discharge and so an interaction term was included in all logistic regression models for live discharge. Figure 2 demonstrates that while full code status was associated with predicted higher live discharge rates for the entire population (discharge rate of 14.9% for hospice enrollees with full code orders vs. 8.5% for those with DNR orders), the effect is particularly pronounced for nonwhite patients. African American patients with full code orders in place had a hospice live discharge rate of 23.8% versus the 11.6% rate for African Americans with DNR orders in place. Similarly, the live discharge rate for those describing their race as neither white nor African American was 25.8% if full code orders were in place versus 10.8% if DNR orders were in place.

Adjusted rates of short, medium, and long live discharges for hospice enrollees with DNR versus full code orders. Black = full code; striped = DNR. Adjusted for age, sex, disease (cancer, dementia, or other), location of care (home, hospital, nursing home, or hospice), and year.
Discussion
Our study indicates that the 12.9% of hospice enrollees who are full code are at a heightened risk for hospice live discharge, regardless of gender, race, or disease process. Furthermore, these live discharges are more likely to be after short stays, indicating the patient or family is either dissatisfied with hospice or prefers aggressive care, and not long stays, more likely in the case of recovery or stabilized illness. Finally, we demonstrate that while African American patients are more likely to have full code orders in place, the association of full code orders with hospice live discharge is stronger for nonwhite than for white patients. This work implies that the population of hospice enrollees electing full code orders is a potential target for improved communication and decision-making support.
Very little is known about the reasons why patients elect full resuscitation status while electing the hospice benefit. It is possible that patients do not understand the benefits and burdens of CPR for frail terminally ill people. Alternatively, patients and families may desire some modicum of control and see not signing DNR orders as a way to maintain either control or hope for recovery during a difficult time. Finally, an unwillingness to sign DNR orders and hospice live discharge may represent a gap in trust between patients and hospice clinicians. These explanations represent reasons why increased decision support could help patients rethink their code status and possibly change the trajectory of their hospice care.
It is also possible that the patterns we observe are due to the decision for hospice benefit election being in itself problematic. Patients may need additional support at home that hospice provides, but have preferences for aggressive care not consistent with the hospice benefit. They may therefore elect hospice, but maintain full code orders, and then, at the time of health decline, opt back into disease-targeted treatments. This indicates more a failure of policy than patient decision making. There is hope in efforts such as the Medicare Care Choices Model 19 that allows patients to access both disease-targeted and palliative care, although there is great need to enrich supportive care services for all patients with serious illness.
There are several next steps for both intervention and further research that result from this study. Clearly, there is a need to understand the motives and reasoning of patients electing full code in hospice. Regardless of this, live discharge rates are an important quality measure for hospices, and this work shows that those with full code on enrollment have a higher risk of live discharge. At minimum, flagging patients who are full code at hospice enrollment provides an opportunity to target supports to this high-need population in a trackable and systematic way. It is possible that increasing support around resuscitation decisions or goals of care decisions in general could lower live discharge rates, especially those occurring soon after hospice enrollment.
Our study has several limitations. First, this is a retrospective review limited to data collected by the electronic medical record for clinical and billing purposes and not specifically for the purpose of this study. We therefore do not have detailed information about a range of treatment preferences, although clearly even our simple variable of DNR versus full code orders predicts a clinical outcome. Second, limitations of the EMRs did not allow us to differentiate between patients who converted to DNR status during their stay on hospice care, meaning that our numbers likely underestimate the number of patients who do not initially complete a DNR at the time of admission to hospice. We therefore likely underestimate the impact of having a full code order in place throughout the duration of the hospice enrollment. We also do not have data on proxy or guardian status, which is common and may impact how DNR orders are perceived and dynamics of decision making. 20 This study, while capturing a large population, is also regional and in a nonprofit hospice setting. A potential next step is to see if the relationship between full code orders and live discharge is similar in different regions and for-profit hospices.
This study demonstrates that full code orders in hospice are both relatively common and are independent risk factors for hospice live discharge, particularly for nonwhite patients. Understanding more about these patients and how to improve their care will be an important mechanism to address hospice live discharges and support the decision making of all patients at the end of life.
Footnotes
Acknowledgments
Dr. Ankuda is funded by the Robert Wood Johnson Foundation Clinical Scholars Program and a Blue Cross Blue Shield of Michigan Physician Investigator Award.
Author Disclosure Statement
No competing financial interests exist.