
Abstract
Abstract
Background:
While the importance of pediatric palliative care (PPC) for children with life-threatening illness is increasingly recognized, little is known about physicians' attitudes toward palliative care for children with heart disease.
Objective:
To compare the perspectives of PPC physicians and pediatric cardiologists regarding palliative care in pediatric heart disease.
Design:
Cross-sectional web-based surveys.
Results:
Responses from 183 pediatric cardiologists were compared to those of 49 PPC physicians (response rates 31% [183/589] and 28% [49/175], respectively). Forty-eight percent of PPC physicians and 63% of pediatric cardiologists agreed that availability of PPC is adequate (p = 0.028). The majority of both groups indicated that PPC consultation occurs “too late.” Compared with pediatric cardiologists, PPC physicians reported greater competence in all areas of advance care planning, communication, and symptom management. PPC physicians more often described obstacles to PPC consultation as “many” or “numerous” (42% vs. 7%, p < 0.001). PPC physicians overestimated how much pediatric cardiologists worry about PPC introducing inconsistency in approach (60% vs. 11%, p < 0.001), perceive lack of added value from PPC (30% vs. 7%, p < 0.001), believe that PPC involvement will undermine parental hope (65% vs. 44%, p = 0.003), and perceive that PPC is poorly accepted by parents (53% vs. 27%, p < 0.001).
Conclusions:
There are significant differences between pediatric cardiologists and PPC physicians in perception of palliative care involvement and perceived barriers to PPC consultation. An intervention that targets communication and exchange of expertise between PPC and pediatric cardiology could improve care for children with heart disease.
Introduction
C
Studies have begun to assess the end-of-life experience of children with heart disease, 9 their families, 10 and their providers. 11 A recent single-center retrospective study of PPC team involvement in children with cardiac disease over a five-year period demonstrated that PPC addresses a range of issues, from psychosocial support to advance care planning, and is incorporated not only around end of life but also much earlier in the illness course. 12 In addition, for those children who died, end-of-life care patterns were found to be consistent with family goals of care. Initial investigations have taken place into pediatric cardiologists' attitudes toward palliative care, including barriers to palliative care involvement and perceived competency in symptom management, prognostic awareness, and advance care planning. 13 However, little is known about PPC physicians' attitudes toward palliative care for this unique patient population, or how PPC physicians' attitudes are compared with those of pediatric cardiologists.
Methods
Study design
This is a cross-sectional survey study of PPC physicians and pediatric cardiologists in the United States in 2016. The PPC physician survey was circulated via email to members of the pediatric special interest group of the American Academy of Hospice and Palliative Medicine (AAHPM). A letter introducing the study and survey was included. Two reminder emails were sent at monthly time intervals.
Study design for the original cohort of pediatric cardiologists has been previously reported. 13 In brief, the study authors contacted a single pediatric cardiologists at 19 medical centers across the United States and requested that the survey be circulated by email to faculty within the Department of Cardiology. All 19 centers agreed to participate. Two monthly reminder emails were sent. The surveys of pediatric cardiologists and palliative care physicians were circulated within the same three-month period. The Boston Children's Hospital Institutional Review Board approved the study protocol and survey instrument.
Survey development
The Provider Survey about Palliative Care for Children with Heart Disease (PSPHD) 13 was adapted from a recent survey of members of the American College of Cardiology related to adult patients with end-stage cardiovascular diseases. 14 The surveys were then modified for PPC physician and pediatric cardiology participants. Shared domains between the two surveys included perceived barriers to palliative care consultation, timing and extent of palliative care involvement, and physician competency in symptom management and palliative care skills. Physician demographic and practice characteristics were also queried.
Participants
This study included two groups of participants: (1) PPC physicians and (2) pediatric cardiologists (described previously 13 ). The first two questions of the modified PSPHD instrument for PPC physicians were mandatory and served as inclusion criteria for the study to ensure that respondents identified as physicians who practice subspecialty PPC.
Data management and statistics
Qualtrics, an online survey tool (Qualtrics, Provo, UT), was used to distribute the surveys and securely store responses. Descriptive statistics were performed for continuous and categorical variables. Fisher exact and Chi-squared tests were used to assess association between categorical characteristics and categorical response. The Mantel–Haenszel test was also performed for ordinal categorical variables, but inferences were similar (results not shown). For binary responses formed from collapsed response categories, logistic regression models were used to describe the relationship between the response and the predictor of interest. The differences in the responses of PPC physicians and pediatric cardiologists to corresponding questions were compared using Chi-square tests. A p-value of <0.05 was considered statistically significant.
Results
Characteristics of participants
A total of 179 individuals in the AAHPM pediatric special interest group received the survey via email. Of the 52 people who opened the survey link and began the survey, 49 met the inclusion criteria giving an overall response rate of 28% (49/175). As previously described, 13 the pediatric cardiology cohort had an overall response rate of 31% (n = 183/589), with a final analytic cohort of 165 physicians who provided complete responses. The sample included general pediatric cardiologists (30%), cardiac intensivists (20%), heart failure specialists (16%), and other cardiac subspecialists (34%). Demographic and practice characteristics of the PPC and pediatric cardiology physicians are shown and compared in Table 1.
Results displayed as mean ± SD or n (%).
The pediatric cardiology and PPC physician groups varied significantly based on race/ethnicity (p = 0.02), with a greater proportion of cardiologists identifying as Asian (15% vs. 2%) but showed no differences in terms of years of experience, religion, practice type, or location. PPC physicians were significantly more likely to practice at institutions that offer heart transplant and ventricular assist device placement (VAD), although overall number of inpatient beds appeared to be similar. Compared with pediatric cardiologists, PPC physicians reported that a significantly greater percentage of the patients they care for die in a given year of practice (84% vs. 8% with death of ≥5% of patient cared for per year). PPC physicians were more likely than pediatric cardiologists to have received didactic training in caring for children with heart disease at end of life (44% vs. 21%, p = 0.001).
Perceptions of palliative care involvement
Significantly more PPC physicians reported the presence of automatic palliative care consultations for certain diagnoses or interventions encountered in pediatric cardiology practice (48% vs. 27%, p = 0.016) and 30% of pediatric cardiologists did not know if automatic consultations were present. Automatic consultations were reported for conditions such as extracorporeal membrane oxygenation (ECMO), heart/lung transplantation, extreme prematurity, trisomy 13 or 18, pulmonary vein stenosis, and single ventricle congenital heart disease.
PPC physicians and pediatric cardiology providers were also asked to report their perceptions regarding degree of palliative care involvement in the care of patients with pediatric heart disease at their institutions. There was no difference between groups in the perceived extent of palliative care involvement for heart transplant (often/always 39–53% of the time), pulmonary hypertension (often/always 22–42%), VAD (often/always 43–53%), and ECMO patients (often/always 30–35%). PPC physicians perceived greater palliative care involvement at their institutions in the care of patients with single ventricle lesions (often/always 40% vs. 19%, p = 0.013) and for cardiac lesions with associated genetic diagnoses (often/always 86% vs. 59%, p < 0.001). In contrast, they perceived less frequent involvement in patients with pulmonary vein stenosis (23% vs. 41%, p = 0.039).
Forty-eight percent of PPC physicians and 63% of pediatric cardiologists agreed that availability of palliative care is adequate at their institution (p = 0.028). Nearly all respondents felt that the palliative care consultations occur “too late” (73% of PPC physicians and 60% of pediatric cardiologists) and none reported that they occur “too early.” The two groups differed with respect to who they think should have primary responsibility for discussing limitations on life-prolonging interventions for pediatric cardiac patients in a variety of settings (p = 0.043). PPC physicians more often selected “case-by-case basis,” while pediatric cardiologists more often selected primary cardiologist or cardiac intensivist. Fewer than 5% of respondents in each group selected “palliative care clinician” or “cardiac surgeon.” Nearly all PPC physicians and pediatric cardiologists disagreed with the statement “palliative care and heart transplant are mutually exclusive.” PPC physicians were more likely to agree with the statement “mechanical devices can be a form of palliative care” (77% vs. 65%, p = 0.021).
Perceived barriers to palliative care involvement
Compared to pediatric cardiologists, PPC physicians more often described the obstacles to requesting palliative care consultation as “many” or “numerous” (42% vs. 7%, p < 0.001, Fig. 1). Pediatric cardiologists were asked to select specific barriers to palliative care consultation, and PPC physicians were asked to describe how they think pediatric cardiologists perceive these barriers. Pediatric cardiologists most often selected “concern that parents will think I am giving up on their child” (56%) and “referring to palliative care services too early will undermine the parents' hope” (44%). Significant discrepancies were noted between PPC physicians and pediatric cardiologists in all but two areas (Fig. 2). PPC physicians overestimated how much pediatric cardiologists worry about the PPC team introducing inconsistency in approach (60% vs. 11%, p < 0.001), perceive lack of added value for PPC (30% vs. 7%, p < 0.001), believe that PPC involvement will undermine parental hope (65% vs. 44%, p = 0.003), and perceive that PPC is poorly accepted by parents (53% vs. 27%, p < 0.001). PPC physicians underestimated the degree to which pediatric cardiologists perceive insufficient palliative care resources to be a barrier at their institution (5% vs. 22%, p < 0.001).
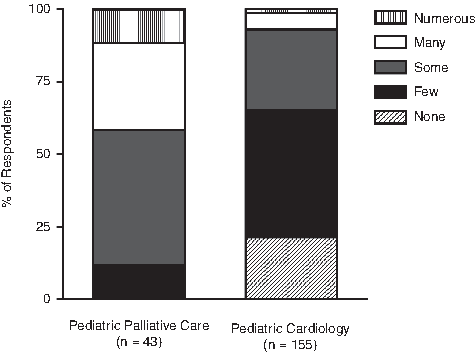
Comparison of physician-reported extent of obstacles to consulting palliative care for children with heart disease at their institution.
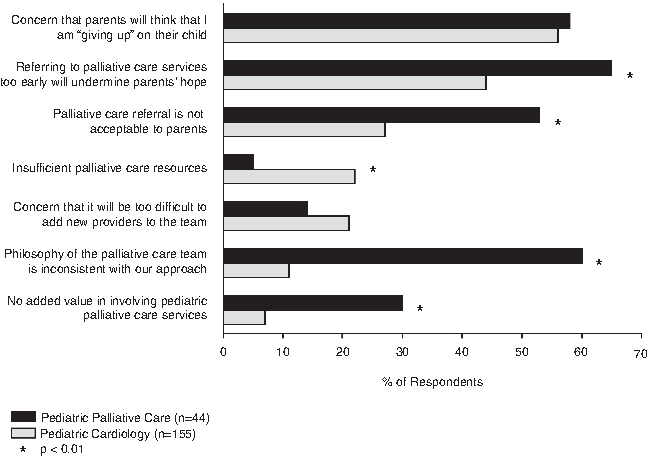
Comparison of physician-reported obstacles to palliative care involvement in pediatric cardiology patients at their institution. Bars represent percentage of physicians who selected each barrier.
Perceived physician competency
Physicians in both groups were asked to report their degree of competency in a variety of areas, including care at end of life, prognostication, communication, and symptom management in the setting of children with heart disease. For each clinical activity, PPC reported a higher level of competence compared with pediatric cardiologists (Figs. 3 and 4). These differences were statistically significant with p < 0.01 in every area other than prognostication of life expectancy, in which both groups reported relatively low levels of perceived competency (51% of PPC physicians and 33% of pediatric cardiologists perceived themselves as “moderately” or “very” competent, p = 0.21). In terms of symptom management, PPC physicians reported the lowest levels of perceived competence in management of thirst and fatigue, while pediatric cardiologists reported the lowest levels of perceived competence in addressing psychological distress (Fig. 4).
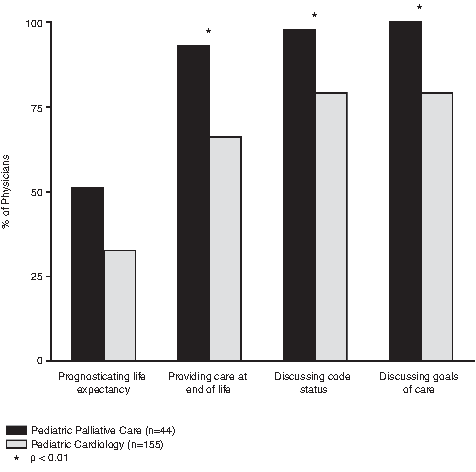
Comparison of perceived physician competency in advance care planning, communication, and palliative care skills. Bars represent percentage of physicians reporting “moderately” or “very” competent.
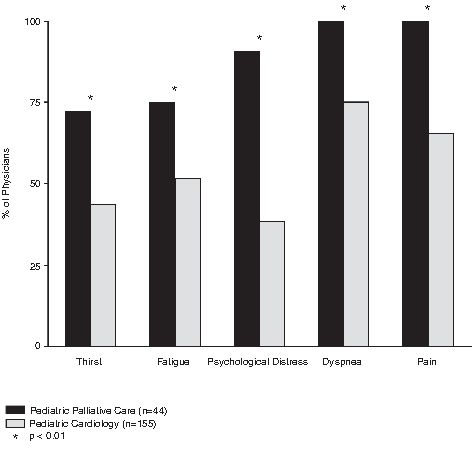
Comparison of perceived physician competency in symptom management. Bars represent percentage of physicians reporting “moderately” or “very” competent.
Discussion
This study provides the first assessment of how pediatric cardiologist and PPC physician perspectives compare regarding palliative care for children with heart disease. We demonstrate that there are gaps in perception of palliative care involvement in a variety of cardiac conditions, that the majority of all physicians feel that palliative care consultations occur too late, and that there are significant discrepancies in perceived barriers to palliative care. PPC physicians report greater perceived competency in areas related to palliative care and symptom management.
The two groups of physicians were similar in most demographic and practice characteristics. The most notable difference was that the PPC physicians reported significantly less exposure to heart transplant and VAD. This finding suggests that the cohort of PPC physicians in our study may be seeing a population of children with less severe heart disease, compared to the pediatric cardiology physicians who almost all worked in institutions with advanced cardiac technologies. PPC physicians reported greater presence of automatic palliative care consultations at their institutions for conditions such as heart transplant and ECMO, and a third of pediatric cardiologists did not know if automatic consultations were present. These findings highlight a discrepancy in awareness about the availability of PPC consultation and suggest opportunities for education about the role of PPC.
Both PPC physicians and pediatric cardiologists report greatest palliative care team involvement in patients with underlying genetic syndromes, single ventricle lesions, and in those who have received a heart transplant or VAD. Only one third of both PPC physicians and pediatric cardiologists report consistent PPC involvement in patients requiring ECMO, which is somewhat surprising given that 60% of children requiring ECMO for cardiac indications do not survive to hospital discharge. 15 This finding suggests that further PPC involvement may be indicated in patients requiring advanced cardiac technologies and prompts consideration for the use of automatic PPC consultations as a means to expand this involvement. 16
PPC physicians are more likely than pediatric cardiologists to report that the subspecialty palliative care service is “often” or “always” involved with single ventricle diagnoses and congenital heart disease in children with genetic syndromes. This may reflect that the overall number of children with these conditions seen by PPC physicians is significantly smaller than that seen by pediatric cardiologists, and therefore, they perceive a higher percentage of their teams' involvement. In addition, the children they do see with these conditions are likely the more severe cases, while cardiologists see the entire spectrum of clinical severity for each condition. In contrast, compared to the pediatric cardiologists, PPC physicians perceived less frequent palliative care involvement in cases of pulmonary vein stenosis. This likely reflects the rarity of the condition and the assumption by PPC physicians therefore that palliative care is infrequently involved in these cases. Moreover, the nearly uniform high mortality associated with this condition may be more familiar to pediatric cardiologists. Perhaps PPC clinicians would benefit from education from pediatric cardiologists about overall survival outcomes in children with heart disease to better inform their understanding of the spectrum of disease severity across a variety of clinical conditions. Overall, the heterogeneity of responses to questions related to frequency of PPC involvement is itself a notable finding, suggesting that PPC involvement depends on a variety of case and institution-specific factors.
Although both pediatric cardiologists and PPC physicians report availability of subspecialty PPC services, still more than one third of each group do not perceive that availability is adequate. Moreover, the majority of physicians in both groups report that palliative care consultation occurs “too late” in the course of a patient's illness. This is consistent with a recent study of palliative care involvement in children with heart disease, which found that among children who died, initial consultation occurred a median of only one month before death. 12
Compared to pediatric cardiologists, PPC physicians were significantly more likely to describe the obstacles to requesting PPC consultation as “many” or “numerous” (7% vs. 42%) and over 20% of pediatric cardiologists reported no obstacles (Fig. 1). The most frequently selected barriers to PPC consultation identified by pediatric cardiologists were “concern that parents will think I am giving up on their child” (56%) and “referring to palliative care services too early will undermine the parents' hope” (44%). Not surprisingly, PPC physicians also identified these as barriers. Given that respondents reported low competency in prognostication of life expectancy, these concerns may delay PPC referral until prognostication is more certain, at which point it may be “too late.”
Furthermore, significant discrepancies were observed between the two groups regarding perceived barriers to PPC consultation. Most notably, PPC physicians vastly overestimated the degree to which pediatric cardiologists worry that the philosophy of the palliative care team is inconsistent with their therapeutic approach (60% vs. 11%). This finding is consistent with the fact that a large proportion of pediatric cardiologists do not identify obstacles to involving PPC and do not view PPC as inconsistent with life-prolonging therapies. Similarly, PPC physicians overestimated the degree to which pediatric cardiologists worry that PPC referral is not acceptable to parents and that there is no added value in involving PPC. In contrast, PPC physicians underestimated the degree to which pediatric cardiologists identify insufficient PPC resources as a barrier to consultation. This is consistent with our finding that about one third of pediatric cardiologists view PPC resources as inadequate.
Not surprisingly, PPC physicians reported greater competency across all areas surveyed, including care at end of life, communication, and symptom management (Figs. 2 and 3). These differences may reflect that PPC physicians have undergone subspecialty training in these areas. However, it is striking that over half of PPC physicians had not received training specific to children with cardiac disease. Moreover, over a quarter of PPC physicians do not feel “moderately” or “very” competent managing thirst and fatigue, two common symptoms of heart failure. 17 The discrepancy in reported competency levels between PPC physicians and pediatric cardiologists highlights not only the role for greater subspecialty PPC involvement in the care of children with heart disease but also a need for training both PPC physicians and pediatric cardiologists in symptom management.
A recent study found that the most common indications for PPC consultation in children with heart disease are delineation of goals of care and provision of psychosocial support for families. 12 This is, in part, consistent with our findings, in which PPC physicians are significantly more comfortable than pediatric cardiologists in managing psychological distress of patients and families. However, given that nearly 80% of pediatric cardiologists report feeling competent in discussing goals of care, 13 it is surprising that PPC is so frequently consulted for this indication. Perhaps this reflects that the stated indication for PPC consultation may not adequately capture the complexity of the factors involved. It may also reflect the lack of time that pediatric cardiologists have to spend with patients to have these discussions. In addition, it may indicate that further education in communication and family support is indicated.
This survey-based study has several important limitations. Although consistent with those of other web-based physician surveys, 18 the response rate for both PPC physicians and pediatric cardiologists may limit the study's generalizability. In addition, the pediatric cardiologist cohort was heterogeneous with only a portion of them caring for sicker patients. General cardiologists and other cardiac subspecialties may have more limited knowledge of or exposure to palliative care. While urban, academic, and large hospitals are overrepresented, there was more balanced regional representation. In an effort to preserve anonymity and encourage participation, institution names were not collected, and therefore, the two groups of physicians were not matched by institution type. A follow-up study that matches participants by institution or type of institution would be valuable in the future. Sampling bias may have contributed to an overestimation of both PPC involvement and physician competency measures. In addition, competency measures in this study were physician-reported and therefore do not provide objective measures of knowledge or competency.
Despite these limitations, this study offers valuable new insight into the differences between pediatric cardiologist and PPC physician perspectives on the role of palliative care in children with cardiac disease. We have demonstrated that both pediatric cardiologists and PPC physicians feel that PPC occurs too late. Compared with pediatric cardiologists, PPC physicians feel that obstacles to palliative care consultation are greater and they overestimate the degree to which pediatric cardiologists perceive that palliative care will be inconsistent with their team's approach. PPC physicians, not surprisingly, report greater levels of competence across all areas related to palliative care and symptom management. An intervention that targets communication and exchange of expertise between PPC and pediatric cardiology could improve care for children with heart disease.
Footnotes
Acknowledgments
This study was supported, in part, by the Kobe Perry Fund and the Sophia Dean Fund of the Advanced Cardiac Therapies Education & Research Fund at Boston Children's Heart Center. We thank the physicians who participated in this study for sharing their experiences and perspectives. In addition, we thank Minmin Lu for her assistance with biostatistical analysis.
Author Disclosure Statement
No competing financial interests exist.