
Abstract
Abstract
Surgical-site infection, spinal cord abscess, and catheter tip granuloma are known but rare complications of intrathecal drug delivery systems (IDDS). To date, there are no published cases of brain abscess in a patient with an IDDS. In this study, we report a case of a cancer patient with an IDDS for management of cancer pain who developed a brain abscess with profound mental status changes and clinical management challenges.
Case Report
A 75-
Three months following a standard, sterilely performed pump refill (17 months after implantation), he presented to the emergency department (ED) with acute aphasia, confusion, and fever of 100.8°F. Other vital signs on initial presentation included heart rate 104, blood pressure 172/92, respiratory rate 22/minute, oxygen saturation 97% on room air. There was no neck stiffness or signs of meningismus. Laboratory tests were performed, including a complete blood count (leukocyte count 9.7 k/μL without left shift) and a metabolic panel, which were all within the normal reference range. Gram stains and cultures of blood and urine showed no microbial growth. The IDDS was telemetrically interrogated, and no malfunction, programming error, or dosing error was identified. Inspection showed no signs of infection at the pump site or at the intrathecal catheter implantation site in the lumbar region. A lumbar puncture was performed with unremarkable cerebrospinal fluid (CSF) values, except a CSF protein level of 95 mg/dL (normal reference range <15 mg/dL). Initially, acute alcohol withdrawal was suspected by the ED staff, but magnetic resonance imaging (MRI) of the brain demonstrated a 22-millimeter ovoid mass in the left frontal lobe with rim enhancement and surrounding vasogenic edema, suggestive of pyogenic brain abscess (Fig. 1). Broad-spectrum antimicrobial therapy (vancomycin, cefepime, and metronidazole) was initiated. Additional imaging of the cervical, thoracic, and lumbosacral spine showed no evidence of spinal abscess, discitis, or osteomyelitis. CSF Gram stain was negative and CSF cultures were negative for growth. The source of the brain abscess remained unclear, but the Infectious Disease consultant team recommended explantation of the entire IDDS as they opined that in the absence of a definitive nidus of infection, the IDDS was likely contaminated and seeded the intracranial infection.
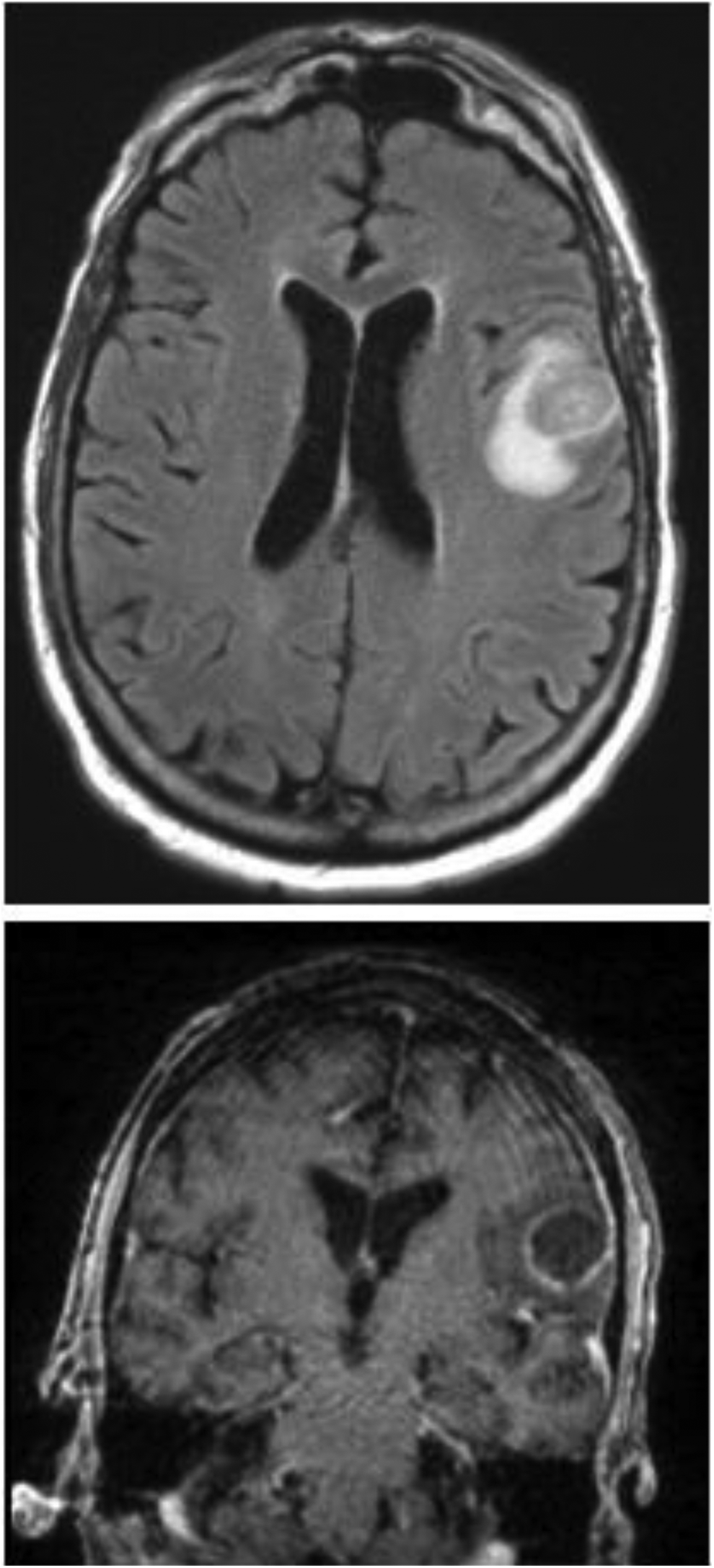
Radiologic imaging–MRI Brain. MRI of the brain demonstrating large spheroid lesion consistent with a pyogenic abscess. MRI, magnetic resonance imaging.
As the patient's mental status remained unimproved with antibiotic therapy, a left frontal craniotomy and abscess drainage was performed on day three of admission. Blood and CSF cultures remained negative for bacterial growth, but wound cultures from the abscess confirmed the presence of Streptococcus anginosus, a bacterial species commonly found in oral cavity and gastrointestinal and genitourinary tracts. The patient's mental status returned to baseline on day 6 of admission and he was discharged home on day 10. He was treated with a six-week course of intravenous ceftriaxone and oral metronidazole and demonstrated a full recovery soon thereafter. He continued to use his IDDS with unchanged programming parameters to satisfactorily manage his chronic rectal and perineal pain as before the hospitalization.
Discussion
The presence of an IDDS in a patient with profound mental status changes and brain abscess can be a source of debate and disagreement among the team of medical providers regarding immediate explantation of the IDDS device. At no time in this case was there clinical evidence of an IDDS wound infection, wound dehiscence or meningismus, and no evidence for a remote infection. Fortunately, a hasty plan to explant the device was thrwarted by interdisciplinary education and close evaluation of the clinical, laboratory, and imaging evidence at hand, tempered with a discussion of the epidemiology of brain abscesses. Indeed, IDDS explantation and abrupt cessation of intrathecal opioids in this case would increase risks to the patient for opioid withdrawal, increased pain, and potential oversedation with parenteral or oral opioid equivalents, all of which would have complicated the recovery from brain abscess and craniotomy and introduced profound and unnecessary costs.
The overall rate of infectious complications from IDDS is low. A retrospective review of 626 IDDS in a pooled analysis of published cases and postmarket data, identified an overall infection rate of 2–8% in adults, with 57–80% of IDDS-related infections occurring at or near the pump subcutaneous pocket site, and 80–90% of IDDS infections presenting clinically within the first two months following surgical implantation.1,2 Staphylococcus aureus and Staphylococcus epidermidis species comprise 50–70% of surgical site infections after IDDS implantation.2,3 Rates of infection are lower in adult patients with IDDS as compared with children, and fecal or urinary incontinence, spasticity, and percutaneous endoscopic gastrostomy (PEG) tubes appear to be risk factors. 2 Neuraxial infections, namely, meningitis, is profoundly rare. In our review of the medical literature, we found a paucity of meningitis cases related to an IDDS and nearly all were in patients treated with intrathecal baclofen for spasticity, but none was in cancer patients. These included single reports of meningitis caused by Staphylococcus aureus, 4 S. epidermidis, 5 nontuberculous Mycobacterium, 6 and Pseudomonas. 7 A retrospective database review of 120 patients with IDDS showed one case of S. aureus meningitis, 8 and a more comprehensive 2007 systematic review of all publications on IDDS showed only one case of meningitis. 9
Although each percutaneous IDDS refill is indeed an opportunity for skin flora or contaminated drug to be introduced into the IDDS drug reservoir, bacterioretentive filters decrease the likelihood of seeding of the IDDS or the neuraxial space with bacteria. In this case, the IDDS contained filter pores that are 0.22 microns in diameter, preventing the passage of Streptococcus species, which are known to range in size from 0.5 to 2.0 microns. 1 These filters should prevent the passage of bacteria, but the duration of filter efficacy and integrity is unknown, and in theory, an IDDS that is contaminated with bacterial growth could overwhelm these barriers.
To date, brain abscess has never been reported in patients with IDDS. In this case, physical examination, laboratory findings, and imaging did not support the differential diagnosis of a bacterial infection of the CSF seeding deep in the brain. Brain abscess results from a contiguous infection near the brain (otitis media, oral and pharyngeal infections, sinusitis, mastoiditis, and cranial cellulitis), hematogenous dissemination from a distant site of infection, and in cases of open skull fractures, head trauma, or cranial surgery. 10 It is also seen in congenital cyanotic heart disease where right to left shunting can occur. 11 Forty percent of brain abscesses are related to dental infections and 32–60% are polymicrobial. 12 In at least 25% of cases, no etiology of a brain abscess can be found. 10
This infection most commonly presents as a solitary deep frontal lobe lesion and has a predilection for men, diabetics, alcoholics, and the immunocompromised. The mortality rate is 4–20% and patients with cranial neoplasms or chronic illness are known to have a more difficult clinical course. 13 Clinical presentation in adults is most commonly headache, fever, and mental status changes, with negative blood cultures in 24–40% of cases. The infection typically starts as a local area of cerebritis that develops into a pus-filled cavity surrounded by a well vascularized region. In comparison, neoplastic brain lesions are typically less vacularized. 11
S. anginosus species, also called S. millieri, the causative bacteria in this case, is a normal component of the microflora of the oropharyngeal, gastrointestinal, and genitourinary tracts, and has been implicated as a cause of both bacteremia and liver or brain abscesses in patients with colorectal malignancy.14,15 As the CSF was not contaminated and no other potential infectious source was found, the brain abscess was most likely cryptogenic. Direct bacterial seeding of the CSF from a contaminated IDDS could, in theory, cause a brain abscess immediately adjacent to the ventricles, but this could not explain the presence of a deep frontal lobe abscess, where there is no contact with CSF. This patient's immunocompromised state, postoperative and postradiation pelvic and rectal anatomy, and history of straining during defecation could have caused a transient bacteremia and thereby support the hematogenous-spread theory seen in other gastrointestinal malignancies,16,17 but no objective evidence is present to support this theory in this case.
If indicated, the IDDS side port and refill (reservoir) ports can be respectively sampled for Gram stain and bacterial culture to confirm or rule out a contaminated IDDS, but was not necessary in this case. If IDDS contamination is identified and results in CSF contamination, the IDDS is typically surgically explanted in toto, although intrareservoir antibiotic administration has been reportedly successful.
Conclusion
Infectious complications of IDDS are rare, especially when they occur temporally remote to the surgical implantation. When neuraxial infections do occur in a patient with an indwelling IDDS, the device may be reflexively and incorrectly implicated as the cause, a costly mistake. Pain specialists and their colleagues should be aware of the bacteriostatic safeguards of IDDS in current use, and the clinical signs, symptoms, and imaging results seen with intrathecal infection, as well as the epidemiology of brain abscess. Transient bacteremia in an immunocompromised and frail patient with a lower GI malignancy could have caused the brain abscess in this case, but was most likely cryptogenic. In any case, the abscess was completely unrelated to the IDDS. It should be self-evident that critical management decisions in complex patients being managed by multiple provider decisions–such as IDDS explantation–are taken only after clinical examination, evaluation of laboratory and imaging results, and team discussion.
Footnotes
Author Disclosure Statement
No competing financial interests exist.