
Abstract
Abstract
Aim:
The primary objective of this study was to describe demographics and end-of-life treatments of children with cancer at a government tertiary cancer center in India.
Methods:
A retrospective review was undertaken of medical charts of all children younger than 18 years, who died as inpatients while undergoing treatment at the pediatric oncology department between April and September 2016. Data were collected on demographics, diagnosis, treatments, survival, palliative care involvement, and symptoms at end of life.
Results:
There were 44 pediatric oncology patients who died in the hospital during the study period. The most frequent diagnoses were hematological malignancies (n = 29).
Tumor-specific treatment was given to 38/44 (86%) patients in the last 30 days of life, and 13 patients in the last day of life or 1 day before. Of all deaths, 23/44 (52%) occurred within 30 days of admission to the pediatric ward and 34/44 (77%) within 90 days.
Of the 44 patients, 25 (57%) were referred to palliative care. The median number of days between referral and death was 14 (0–78) days. Frequent symptoms documented were bleeding (11/44), dyspnea (10/44), pain (7/44), seizures (7/44), and delirium (5/44), with each patient having one or more of these symptoms. Only patients with a palliative care referral received opioid analgesics or benzodiazepines at the end of life.
Conclusions:
This study highlights the demographics of suffering, death, and end-of-life care in children with cancer at a government tertiary cancer center in India.
Introduction
A
India is categorized as a low- and middle-income country (LMIC). In India, as in many other LMIC, a two-tier system of healthcare exists. 6 There are public (government) facilities, which are underresourced and overcrowded, providing free treatment to below poverty line households who cannot afford better resourced healthcare. There are also the private and corporate hospitals, which are well resourced and accessible to the minority of the Indian population that can afford the costs. Public health expenditure is considered a surrogate marker of access to cancer care and survival, and in India it stands at around 1% of gross domestic product. 7 This puts India in the bottom 15 of 188 countries ranked on public health expenditure as per data for the year 2014 from the World Health Organization (WHO). A large proportion of health expenditure is paid out of pocket by households, with only around 15% of the population being covered by health insurance. This results in increasing inequality in access to cancer care, financial catastrophe, and the vicious cycle of poverty and illness.
The public healthcare system is structured stepwise, with basic medical care being provided in primary health centers in the rural community settings, and specialist oncology care being usually found only in the regional tertiary referral cancer centers. 6 There are 25 regional cancer centers in the country. Families often have to travel many hundreds of kilometers to access public cancer care. Adding to this, there is little awareness about cancer in the general population, few screening programs, and much stigma in the community related to cancer. All these factors lead to delay in seeking treatment and advanced presentation.
The government-run cancer centers are mostly located in urban areas, are significantly overcrowded, with multiple patients sharing a bed, and there are often delays in being seen by an oncologist and starting treatment. Supportive services such as nutrition, physical therapy, and social workers are usually lacking. Pain and palliative care services, with access to opioid medications, are also lacking, and pain is usually managed with nonsteroidal medications. Medical records are paper based and documentation can be erratic, illegible, and incomplete.
In India, there are estimated to be more than a million cancer patients in severe pain who require opioids for pain relief. Only about 0.4% of that population has access to the opioid analgesic morphine. 8 Morphine consumption is used as a surrogate marker for access to palliative care globally. The National Cancer Control Programme of India in 1987 designated palliative care as a priority, and still most of the large cancer hospitals in India, including 18 of the 29 government-designated lead cancer centers, do not have a dedicated palliative care service. 9 Among the palliative programs that do exist, very few have pediatric expertise and thus deprive children and their families of the benefits of palliative care.
The institute where the current study was conducted is one of the designated regional cancer centers of India and the only government-run cancer hospital in the states of Andhra Pradesh and Telangana. The institute has a catchment area of 85 million inhabitants, which is the population of Andhra Pradesh and Telangana combined. The pediatric oncology department provides cancer treatment free of cost for children and consists of two wards with a total of 89 beds available. There are no single rooms. In the pediatric wards, there are at any given time around 120 patients admitted. Every year the hospital cares for around 1000 children with cancer. All curative treatment is inpatient. Children go home at completion of each phase (induction, consolidation, and maintenance) of treatment for few days and then return to continue treatment. Patients and families often travel long distances and then stay in the hospital for weeks, deprived of their extended family and community support when it is needed most. 9
A distinct pediatric palliative care service, integrated into the pediatric oncology service, was created at this institute in 2007, to care for patients under curative treatment and also patients with advanced disease. The service, consisting of a dedicated team of physicians, nurses, and social workers trained in pediatric palliative care, provides free treatment for all children. Screening for pain is carried out on all patients and the commonly used opioid analgesics (oral and parenteral morphine, and parenteral and transdermal fentanyl) are available for the patients who need them. The oncology team refers a patient to palliative care either when they are on curative treatment and they have severe physical symptoms (most commonly pain) or when they have advanced disease. The pediatric palliative care service also offers home-based care for patients living in the city of Hyderabad and phone support for those living further away. There is also inpatient hospice care provided for children with difficult symptoms or those needing end-of-life or respite care.
The five-year survival for childhood cancer in India is about 37–40%, much lower than the expected almost 80% survival in HIC.10–12 Treatment refusal and abandonment, due to complex socioeconomic factors, are postulated to be a major cause for therapy failure in India. 13 In HIC, treatment failure and relapse are the leading causes of pediatric cancer mortality, whereas in LMIC, the limited access to diagnostic facilities and care, abandonment due to the prolonged travel time to care facility, transportation costs, and treatment-related financial burden are significant determinants of cancer cure and prognosis. Early mortality related to disease is high.
Literature from HIC reports significant suffering at end of life in childhood cancer, and describes the need for, and benefit of, pediatric palliative care in this setting.14–16 There are limited data from India on how children with cancer die and there is a need for more studies from LMIC to understand and plan for better pediatric oncology services, including palliative care, in the lesser resourced settings. To describe the suffering at end of life in children with cancer would be the first step to identify the palliative care needs and deliverables for tertiary cancer centers in the country.
The level of intensity of tumor-specific treatment at the end of life is a controversial subject. There is literature from HIC that describes high-intensity end-of-life care (HI-EOLC) in children with cancer, particularly in hematologic malignancies. 17 There is little awareness about this issue in India.
The primary objective of this study was to describe the end-of-life treatments, and demographics, of children with cancer at a government tertiary cancer center in India. A secondary objective of this study was to raise awareness about high-intensity tumor-specific end-of-life treatments in children with cancer.
Methods
A retrospective study was done of medical records of all children up to 18 years of age who died between April 1 and September 30, 2016, while undergoing curative treatment at the pediatric oncology department at this center.
Data regarding age at admission, cancer diagnosis, tumor-specific treatment during the last 30 days of life, palliative care referral, symptoms and symptomatic treatment at end of life, and date of death were collected. Additional data regarding demographics were obtained by conducting telephone interviews with the family caregivers of the children. Approval was granted for this study by the institutional ethics committee.
Descriptive statistics were presented in tables using median (lowest-highest value) for continuous variables and percentages for categorical values. Whenever feasible, it was also presented as pie chart or histogram. To test differences between two groups regarding categorical values, Fisher's exact test was used. For survival, a Kaplan–Meier curve, with date of admission to the pediatric ward as entry date, is presented. Date of admission was chosen as entry date for survival analysis as date of diagnosis was not recorded in all cases.
Results
Of the 46 pediatric oncology patients who died in the hospital during the six-month study period, 44 were included in the study. Two patients were excluded because of uncertain diagnoses.
Among the 44 eligible patients, 17 were females and 27 were males. Mean age of the patients at admission was seven years (range 3 months–18 years). For demographic data, see Table 1.
Diagnosis and end-of-life tumor-specific treatment
The most frequent diagnoses were hematological malignancies (n = 29). The remaining patients had solid tumors (Fig. 1).
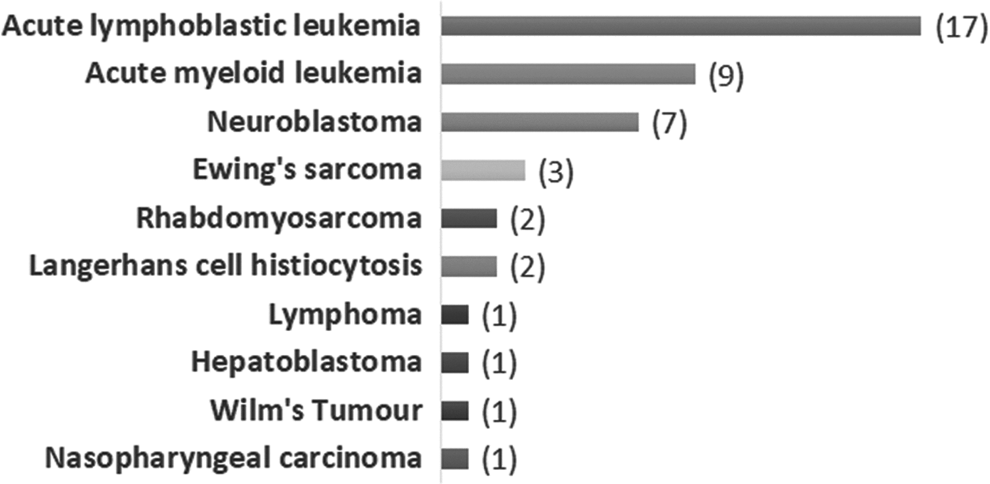
Cancer diagnoses in the study population (number of patients).
Tumor-specific treatment (chemotherapy and/or radiotherapy) was given to 38/44 (86%) patients in the last 30 days of life. There were 25 patients who received tumor-specific treatment in the last week of life and 13 patients who received tumor-specific treatment in the last day of life or one day before (Fig. 2). Median number of days between last tumor-specific treatment and death was 3 (0–30) days. The median survival following last chemotherapy, intravenous or oral, was 3 (0–30) days and 2 (1–30) days, respectively.
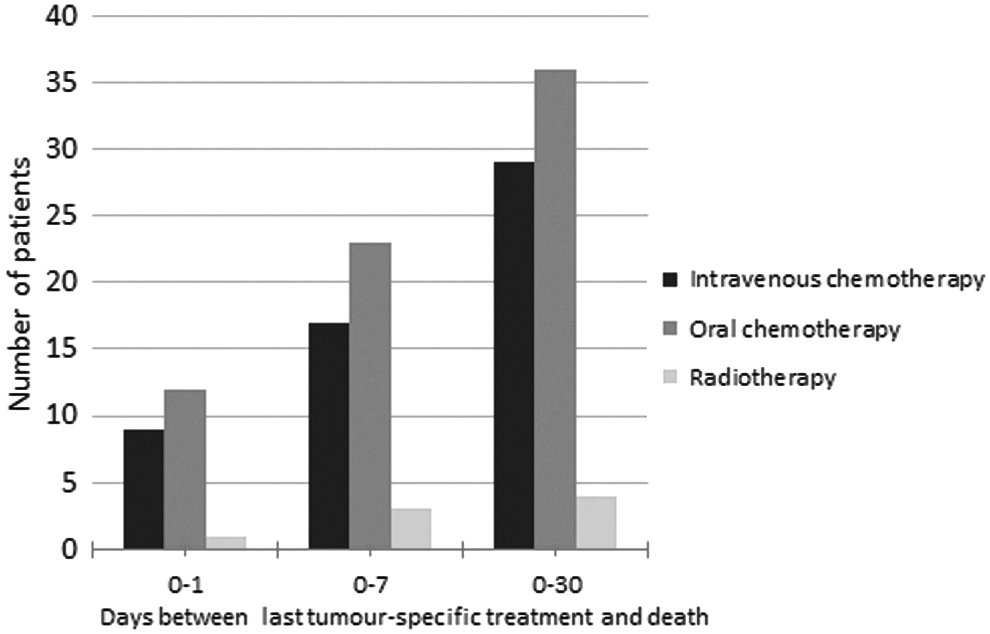
Relationship in time between tumor-specific treatment and death of patients depending on type of treatment.
Of the 29 patients with hematological malignancies, 24 patients (83%) received tumor-specific treatment in the last 30 days of life and 9 (31%) in the last day of life or 1 day before death. Of the 15 patients with solid tumors, 14 (99%) received tumor-specific treatment in the last 30 days of life and 4 (27%) in the last day of life or 1 day before death (Fig. 3).
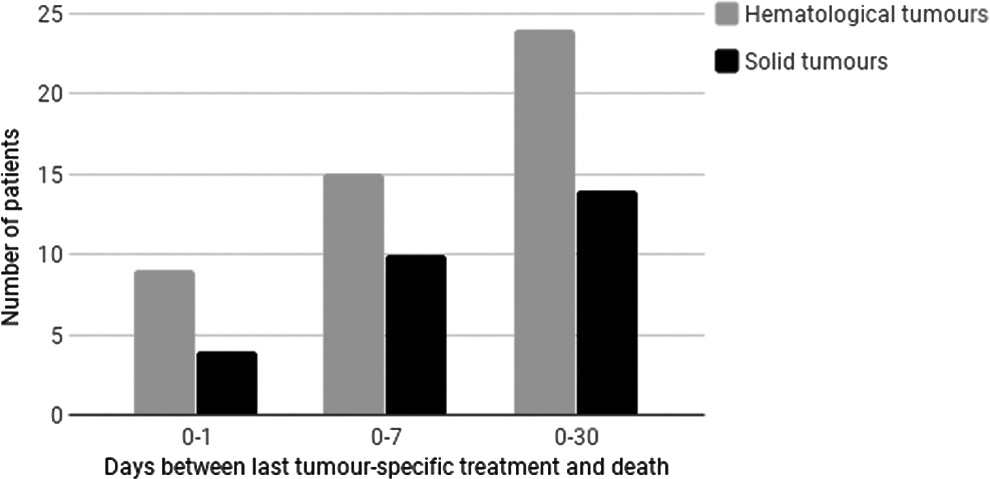
Relationship in time between tumor-specific treatment and death of patient depending on type of malignancy.
Referral to palliative care
Of the 44 patients, 25 (57%) were referred to palliative care. The median number of days between referral and death was 14 (0–78) days with four outliers excluded. In four cases, the date for referral to palliative care was not found. The main reason for referral was pain.
Among the 38 patients who received tumor-specific treatment in the last month of life, 23 (61%) were referred to palliative care. Of the 13 patients who received tumor-specific treatment in the last day of life or one day before, only 4 (31%) had received a palliative care referral (Fig. 4).

Relationship in time between tumor-specific treatment and death of patient depending on referral to palliative care.
Of the 29 patients with hematological malignancies, 13 (45%) received a palliative care referral. Of the 15 patients with solid tumors, 12 (80%) received a palliative care referral (p = 0.052, Fisher's exact test), suggesting a difference in attitudes toward referral to palliative care between the two groups of patients, although not statistically significant in this small study group.
Symptoms and symptomatic treatment at end of life
Symptoms experienced by the patient on last day of life were documented in 30/44 medical charts. Frequent symptoms documented were bleeding (11/44), dyspnea (10/44), pain (7/44), seizures (7/44), and delirium (5/44), with each patient having one or more of these symptoms.
Of the 11 patients with documented dyspnea in the last day of life, 7 were referred to palliative care. Of these patients, four died on the day of referral, before palliative care could be initiated, while the remaining three received benzodiazepines. Of the seven patients with documented pain, six were referred to palliative care. Among those six patients, four received analgesics (the other two died on the day of referral before palliative care could be initiated) and three of four received oral morphine. Only patients with a palliative care referral received strong opioid analgesics or benzodiazepines at the end of life.
Of all deaths, 23/44 (52%) occurred within 30 days of admission to the pediatric ward and 34/44 (77%) within 90 days. One-year survival was below 10% in the study group and just above 20% of the children survived six months following the first admission to the pediatric oncology ward (Fig. 5).

Kaplan–Meier curve depicting survival following admission (in months) to the pediatric ward for the deceased children during this study period.
Discussion
The present study describes the demographics and end-of-life symptoms and treatments in pediatric cancer patients at a government tertiary cancer center in India.
As per a report from the Centers for Disease Control and Prevention, CNS tumors are the leading cause of death from childhood cancer in the United States. 11 Strikingly, they are not even represented in this dataset and are comparatively rarer nation wide. 4 It is believed that the reason for this is delayed diagnosis with only a few patients surviving to presentation at a tertiary cancer center in India.
The survival rate for childhood malignancies is close to 80% in HIC, whereas it is less than half that figure in India. In the present study, more than half of the children dying from cancer during the study period died during their first treatment regimen, underlining the fact that death occurs early in the disease trajectory in LMIC. Previous unpublished research conducted at this institute to determine cause of early mortality during induction phase of pediatric leukemia treatment found that the most common reasons were late presentation, abandonment, limited capacity for intensive and supportive care, infections, and malnutrition.
It is well described in literature from HIC that children with cancer at the end of life experience significant suffering.14,18 According to their parents, about 90% of the children suffered from at least one symptom in the last month of life, most commonly pain, dyspnea, or fatigue, and of those treated for pain, only a quarter achieved adequate pain relief. An audit of pediatric palliative care prescribing practices at a tertiary cancer center in India found that about a third of the prescriptions contained morphine. 19 In many cancer institutes in India, oncologists do not prescribe strong opioids. As our study shows, only patients who receive a palliative care referral would receive morphine and benzodiazepines at the end of life.
A recent study from Canada defined HI-EOLC in pediatric oncology patients as intravenous chemotherapy received within 14 days of death, more than one hospitalization within 30 days of death, or any intensive care unit admission within 30 days of death. 17 In their study, 40.6% of the patients received HI-EOLC and patients with hematologic malignancies were at highest risk for high-intensity care. While it may be appropriate in individual cases, the authors stated that this may indicate a tendency to focus on tumor-specific treatment at the cost of palliative care. Tzuh Tang et al. studied end-of-life care for Taiwanese children with cancer and reported that 50–60% received chemotherapy and intensive care in the last month of life. 20 Only 7.2% patients were referred to hospice care, and a quarter of those referrals were in the last three days of life. They also expressed the opinion that HI-EOLC is an issue that is not addressed in LMIC. A retrospective audit of pediatric palliative care referral practices conducted at a tertiary cancer center in India found that most patients were referred with advanced disease and that oncologists in general were unaware of the scope of pediatric palliative care. 21 In the present study, 52% percent of patients received intravenous chemotherapy in the last two weeks of life, the majority being children with hematological malignancies where the disease was considered still curable. They also had lesser palliative care referrals than patients with solid tumors, corroborated with a near-significant finding.
Earle et al. studied the question of whether aggressive end-of-life cancer care was a quality-of-care issue. 22 They reported that patients receiving aggressive chemotherapy received lesser and delayed hospice referrals. They explored the causes of aggressive end-of-life care and found that it was a combination of the treating oncologist's difficulty in transitioning from curative to palliative care and the unrealistic expectations from patients and their families. Also, physicians tend to overestimate the chance of survival. Studies have described the anxiety experienced by pediatric oncologists when discussing death and dying with patients and their families.23,24 All this results in a higher probability of intensive interventions that could jeopardize a patient's chances of a “good death.” There are no recommendations on when to stop cancer treatment in dying children, and future research needs to focus on this issue. The decision to end a tumor-specific treatment is difficult and requires trust from the family, good emotional support, and communication skills from the medical team, as well as initiating early palliative care to ensure a good quality of life for the child and family at end of life.
This study only captures the death of inpatients undergoing curative treatment. During the same study period, there were several children who died at home, and of whom we have no information of symptoms and treatments given at the end of life. In LMIC, there is limited capacity for supplying end-of-life palliative care to homes far away from cancer centers.
Conclusion
We conclude that pediatric patients who died at this tertiary cancer center died early in their disease trajectory, with tumor-specific treatment given close to death. Only half of the patients were referred to the palliative care department for symptom management. End-of-life symptoms were mainly pain, bleeding, and dyspnea, and only patients referred to the palliative care department received strong opioid analgesics or benzodiazepines at the end of life.
While studies from HIC are critical in understanding and advancing the evolving field of pediatric palliative care, studies from LMIC are equally important in defining the global need for pediatric palliative care. As the demographics of suffering and death differ, so then must the provision of pediatric palliative care and the systems that study, design, and implement these solutions differ. This study highlights the importance of considering the global context of pediatric palliative care as the field evolves and when policies are created. Only once the needs are understood can adequate education, program development, and resource allocation follow.
Footnotes
Acknowledgments
The authors thank Dave Lysecki, M.D., and Simon Sutcliffe, M.D., for their insightful comments during article preparation.
Author Disclosure Statement
No competing financial interests exist.