
Abstract
Abstract
Background:
The term “palliative approach” has emerged to connote healthcare activities provided consistent with the philosophy of palliative care, but not limited to specialized care providers or settings. A rigorous understanding of the palliative approach requires a conceptual model, which links the philosophy of palliative care to specific actions of practitioners, and is applicable to patients with any life-threatening illness, at any point on the disease trajectory, and provided by any care provider in any setting. This article proposes a conceptual model asserting that a palliative approach exists when care simultaneously addresses whole-person needs, enhances quality of life, and acknowledges mortality.
Objective:
To test the content validity of the proposed model against definitions of palliative care in existing literature.
Design:
Electronic and manual literature searches identified definitions of palliative care and palliative approach. Two authors independently conducted thematic analysis to assess congruence with the domains of the proposed conceptual model.
Results:
Nineteen definitions were identified. The three domains were represented in the majority: whole-person care (17/19), quality-of-life focus (17/19), and mortality acknowledgement (15/19). Published definitions also included other concepts, but only one of these (family within the unit of care) appeared in more than a few definitions.
Conclusions:
The content validity of the proposed conceptual model is supported by the consistent presence of the three domains in published definitions. This conceptual model bridges philosophical definitions and clinician behavior and has potential to inform broad implementation of a palliative approach, at both clinic and system levels.
Background
T
Despite considerable literature describing palliative care, the term palliative approach is not well defined. One recent review of the term's utilization 2 describes how a palliative approach is implemented (upstream, adapted, integrated) but does not help nonspecialists understand what it is. A clear definition requires a conceptual model linking the philosophy of palliative care to the specific actions of practitioners. Such a model is necessary to enable us to describe activities consistent with a palliative approach, and recognize the contribution of these activities and providers to the system of care for people with palliative needs.
This article proposes a conceptual model with three core domains (Fig. 1): whole-person care, focus on quality of life, and mortality acknowledgement. A palliative approach exists when care encompasses all domains concurrently. This model, developed by the authors from their general reading of the palliative care literature, is applicable to patients with any life-threatening illness, at any point on the disease trajectory (from diagnosis until death), and can be provided by any healthcare professional (not only palliative care specialists) in any setting. Based on ideas long-held among palliative care practitioners, this model does not introduce new concepts, but links existing ones in a way not previously described.
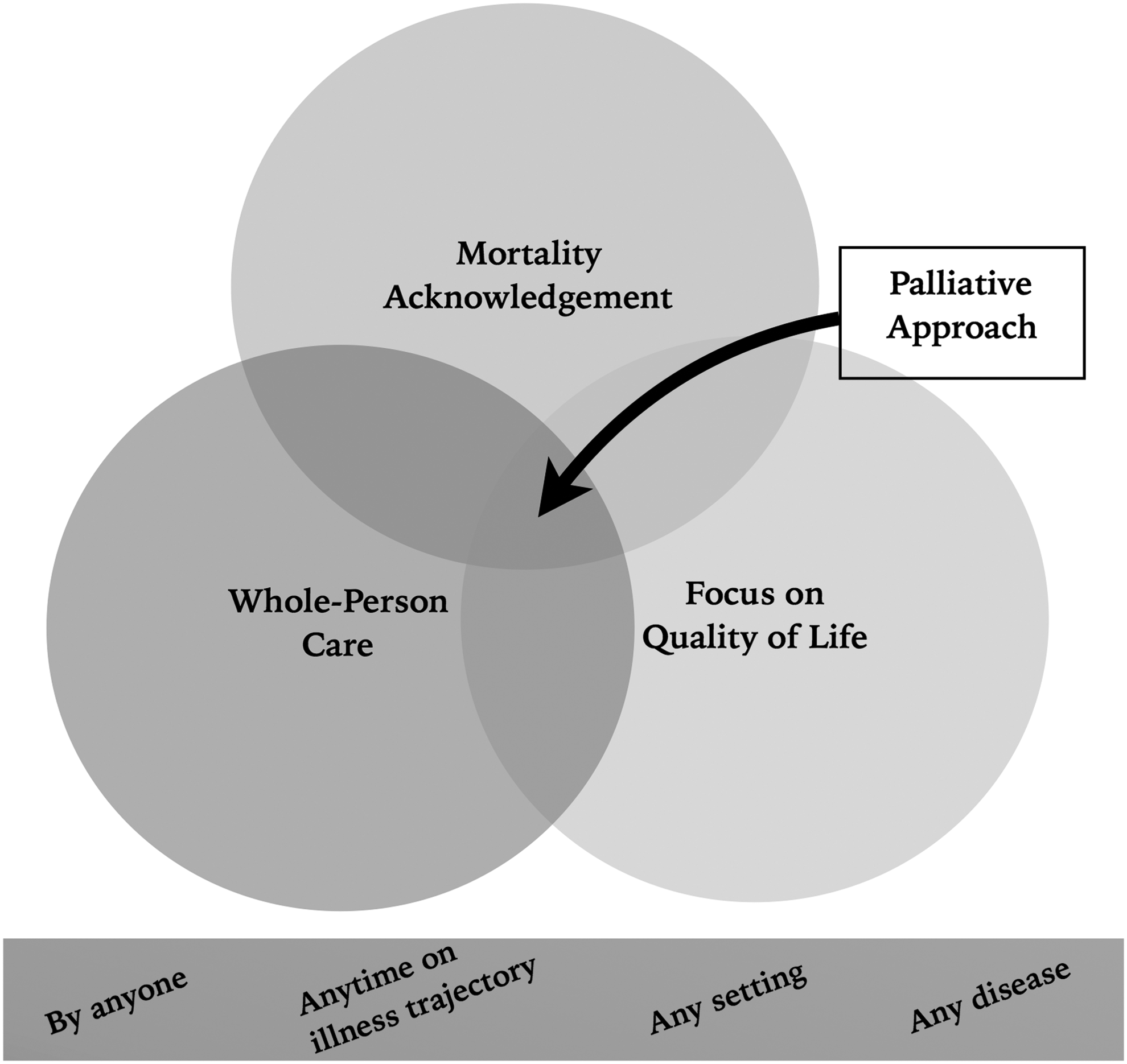
Proposed conceptual model of a palliative approach.
Whole-person care refers to care extending beyond the physical domain, addressing the psychosocial, spiritual, and emotional domains of health.3–5 It involves understanding and supporting patient's values and beliefs, 6 and treating the patient and addressing suffering “holistically.”7–9
Focus on quality of life
A primary goal of palliative care is to optimize patients' quality of life.10–13 Quality-of-life and quantity-of-life goals may coexist, but a palliative approach will always include a focus on the quality of life.
Mortality acknowledgement describes care informed by proximity to death. Mortality acknowledgement does not imply an exclusive or primary focus on death and dying, but recognition of the fact of mortality and exploration of its impact on priority setting and decision making in a patient's care. Mortality acknowledgement can respect patients' varying desire to discuss mortality-related issues, but it still recognizes their relevance.
While a conceptual model of a palliative approach has not been previously articulated, there are numerous definitions of palliative care. The purpose of this article is to assess the content validity of the proposed model by evaluating the consistency between published definitions of palliative care and the three domains proposed.
Methods
The proposed conceptual model was developed by the authors from their general reading of the palliative care literature. To test the content validity of the model, we searched academic literature for definitions of palliative care and conducted a thematic analysis to assess the concordance of the three domains of the model with the content of these definitions.
Literature search
Literature search methods and results are summarized in Figure 2. Web of Science and CINAHL were searched using terms “palliative care OR palliative approach OR palliative medicine” and “defin* OR conceptualiz*”. Articles were selected from initial title and abstract reviews, and included if written in English and focused on defining palliative care and/or a palliative approach. They were excluded if focused solely on patient or provider understandings, specific populations, or did not provide a definition. Additional definitions were obtained through hand-searching references of identified articles, and from a previously published review. 14

Flowchart of literature search for definitions of palliative care.
Definitions of palliative care were extracted from each article and synthesized into a list of distinct definitions organized according to organization or author of origin. Two definitions were excluded at this juncture as they defined solely “specialist palliative care” 15 and palliative care in oncology practices. 16
Thematic analysis
The identified definitions were analyzed to ascertain whether the domains of the proposed model are consistent with them. Each definition was reviewed and broken down into distinct concepts, which were then sorted into four categories: whole-person care, focus on quality of life, mortality acknowledgement, or other. A sample of this method is shown in Figure 3. Whole-person care was defined as care addressing psychosocial, spiritual, emotional, social and/or existential domains. Focus on quality of life was defined as care intended to optimize well-being, comfort, and functional status. Mortality acknowledgement was defined as inclusion of elements related to death, dying, or limited prognosis. “Other” captured concepts that did not clearly fit elsewhere. Two authors independently divided and sorted the concepts. Discrepancies were resolved by consensus.

Method of initial definition analysis, demonstrated using a sample definition. Each definition was divided into distinct concepts, which were then sorted into one of the three categories of the proposed conceptual model or an “other” category.
Results
Literature search
The initial search yielded 52 articles focused on the definition or conceptualization of palliative care. Thirty-three did not meet inclusion criteria. Nine additional articles were sourced from a previous systematic review, 14 and two articles from hand-searching references. Extraction and synthesis resulted in a total of 19 definitions (Table 1).
Thematic analysis
Results of the thematic analysis of concepts within each domain are listed in Table 2. Seventeen of the nineteen definitions of palliative care included at least one concept relating to whole-person care.17–21,23–31,33–35 Seventeen included emphasis on quality of life.17–25,27–32,34,35 Fifteen included concepts related to mortality acknowledgement.17–22,24,25,27,30–35 Some included concepts that did not clearly fall under one of the three proposed domains such as including family in the unit of care,17–21,23,25–27,29,31,33–35 individualized care,23,26 care coordination,18,19,27 or good communication.26,27
Only elements cited by two or more authors are included, with the exception of the “Other” column, which includes all concepts.
Discussion
This conceptual model proposes that a palliative approach exists when care incorporates three domains simultaneously: whole-person care, focus on quality of life, and mortality acknowledgement. The purpose of the literature review and thematic analysis was to determine whether this model is consistent with published definitions of palliative care. The results of the thematic analysis suggest this conceptual model possesses substantial content validity.
While the vast majority of elements included in most definitions of palliative care fall neatly into one of the three domains, several concepts were assigned to the category “other.” Because the content analysis process was, by necessity, interpretive, we chose to be conservative in interpretation, assigning several concepts to the “other” category, which could arguably have been classified differently. For example, “including family within the unit of care” is consistent with both whole-person care and quality-of-life focus, but for the purposes of this review was categorized as “other.” Assignment to the “other” category did not necessarily imply contradiction to the model, but often represented a methodologically conservative decision about how to categorize an element that did not relate only to a single domain.
The domains reflect familiar ideas in palliative care, but the innovation of the proposed model is to make explicit that a palliative approach exists when, and only when, care includes elements addressing all three domains. Every published definition lists features of palliative care17–35 (e.g., “pain and symptom management, information sharing and advance care planning, psychosocial and spiritual support” 18 ). However, each list is different and none specifies the relationship among the features listed. Is the list exhaustive or illustrative? Is every feature mandatory, or only some? Do the features apply to individuals or teams? The conceptual model represents an important step by grouping key features and making explicit the relationship between them.
This model has several potential applications. It can aid education and communication in a topic area where confusion over terminology is common. For healthcare providers and organizations, it could guide efforts to implement a palliative approach by linking the central elements of the philosophy of palliative care to specific and measurable operational practices. (for example, behaviors indicating the presence of whole-person care might include documentation of systematic evaluation of psychosocial care needs. Actions aligning with quality-of-life focus might include documentation of regular symptom assessments. Indicators of mortality acknowledgement might include documentation of goals of care discussions. Finally, the model provides one gauge by which to assess the sufficiency of proposed quality indicator sets as well as existing checklists 50 , 51 : do they address all core domains? Indicator sets that address all core domains, for diverse patient populations, care settings, and provider groups will be keys to supporting equitable access to a palliative approach at a system level.
This article's primary limitation is that the literature search, while thorough, was not exhaustive and was unlikely to capture every extant definition. Future research will further validate the model through direct feedback from palliative care practitioners, and explore use of the model for educational, program planning, and performance measurement purposes in different patient populations, provider groups and healthcare settings.
Conclusion
This article proposes a conceptual model which asserts that a palliative approach exists when care simultaneously addresses whole-person needs, enhances quality of life, and acknowledges mortality. This model is applicable to care provided in any setting, by any provider, to any patient with a life-threatening illness, at any point in their illness trajectory. The domains of the proposed model are consistent with published definitions of palliative care.
Footnotes
Acknowledgment
Andrea McLellan, Head of Collections and Technical Services at McMaster University Health Sciences Library, for her assistance in developing our literature search strategy.
Author Disclosure Statement
No competing financial interests exist.