
Abstract
Abstract
Aim:
To study to what extent tumor-specific treatment (chemo- or radiotherapy) was given during the last 30 days in life and to examine how many of the patients were referred to a specialized palliative care unit (PCU), at a low-resource governmental hospital in India.
Patients and Methods:
Medical records of adult cancer patients deceased between April 1 and May 31 in 2016, and pediatric cancer patients deceased between April 1 and September 30 in 2016 were collected. Data regarding gender, age at admission, cancer diagnosis, tumor-specific treatment received, referral to the PCU, and date of death, were sampled.
Results:
A total of 96 patients (52 adults and 44 pediatric patients) were included in the study. In the last 30 days of life, tumor-specific treatment was given to 39 adult patients and 38 pediatric patients. During the last week in life, 26 adult and 25 pediatric patients, respectively, received tumor-specific treatment. Twenty-six adult and 25 pediatric patients, respectively, were referred to the PCU. End-of-life (EoL) tumor therapy was given to a lesser extent among referred patients.
Conclusions:
Eighty percent of the patients were given tumor-specific treatment near EoL. Half of the patients had been referred for specialized palliative care (SPC).
Introduction
Palliative care and quality of life
T
Given with a palliative intent, both chemotherapy (CT) and radiotherapy (RT) can lead to relief of tumor-associated symptoms. The important goal of tumor-specific treatment, given with a palliative intent, is to not compromise the QoL. 3 Continuation or initiation of tumor-specific treatment, mainly CT, close to end of life (EoL) is correlated with impaired QoL near death. 4 Despite this, it is not unusual with tumor-specific treatment in the last 30 days of life5–8 and according to Earle et al., EoL cancer therapy has become more aggressive during the past decade. 9
The differences worldwide in access to PC for cancer patients are large. According to WHO, many cancer patients in low/middle-income countries (LMIC) receive their diagnosis at an advanced stage and will need PC. 10 In India, nearly 1 million new patients are diagnosed with cancer annually and ∼80% of the cancer patients will present at a late stage of their disease. 11 The public healthcare expenditure is low in India, and PC cannot be provided to all patients in need of symptom relief.12,13 Although the Federal Republic of India has proclaimed that opioids should be provided in the management of cancer pain, many states in India lag behind, and there is in general a restricted access to legal opioids and also lack of education in pain management among healthcare personnel. Other barriers that prevent patients living in rural areas from receiving PC are insufficient infrastructure, illiteracy, and poverty. 14 PC is often misinterpreted as treatment opposed to tumor-specific therapy and both patients and doctors can be hesitant to initiate the discussion of PC. 15
One way of measuring the availability of PC in different countries is the legal consumption of morphine for pain relief. In India, an LMIC, the morphine equivalent opioid used, is less than 1 mg per capita per year, compared with most high-income countries (HIC), where the consumption is more than 100 mg per capita per year. 16
Aim
The aim of this retrospective study was to examine to what extent tumor-specific treatment (CT or RT) was given during the last 30 days of life to in-house patients at a low-resource governmental tertiary referral cancer center in India, and to examine how many of these patients had been referred to a specialized palliative care unit (PCU), at the same hospital.
Patients and Methods
Hospital setting
This state-financed hospital is the only cancer hospital providing treatment free of charge to patients below the poverty line in a catchment area of 85 million inhabitants. Medical and surgical cancer treatments, as well as RT are present. A specialized pediatric oncology department and a PCU are available. The hospital has around 350 beds for in-house patients and a shelter for out-patients during treatment.
Data collection
Medical records of deceased cancer patients were collected through the death register at the hospital. Both adult and pediatric patients (children = younger than 19 years) were included. The sampling dates were: adult patients deceased in the period April 1–May 31 of 2016, and April 1–September 30, 2016 for the pediatric patients. The longer sampling period in pediatric patients was chosen to retrieve a more equal sample size and thus comparable groups of patients.
Data regarding gender, age at date of admission, cancer diagnosis, information on tumor-specific treatment during the last 30 days of life and date of death were collected. Date of referral to the PCU and the reason for referral was also sought. Patients deceased during the study periods without an established cancer diagnosis were excluded from the study. Approval was granted for this study by the Institutional Ethics Committee.
Results
Study sample
Out of 101 eligible patients, 96 were included in the study (Fig. 1). Three adult patients and two pediatric patients were excluded because of uncertain cancer diagnoses. Of the 96 included patients, 52 (54%) were adults, of which 24 were females. The median age at death was 45 years (19–80 years). Of the 96 studied cases, 44 (46%) were pediatric patients. Among these, 17 were females and the median age at death was 6 years (range 3 months–18 years). The dominating diagnoses were hematological malignancies, leukemia, and lymphoma, in 29/44 pediatric patients and in 21/52 adult patients. The remaining group of patients (15 children and 31 adults) had varying types of solid tumors (Fig. 2).

Flow chart of included and excluded patients.

Cancer diagnoses in the study population.
Tumor-specific treatment
Tumor-specific treatment (CT or RT) was given to 77/96 patients (80%) in the last 30 days of life, whereof 39/52 were adult patients and 38/44 were pediatric patients. In the last seven days of life, 26 adults and 25 pediatric patients received tumor-specific treatment, and 11 adults and 13 pediatric patients received tumor-specific treatment on the day of death or one day before (Fig. 3). The median number of days between last tumor-specific treatment and the time of death was 4 days (0–27 days) for the adults and 3 days (0–30 days) for the pediatric patients.
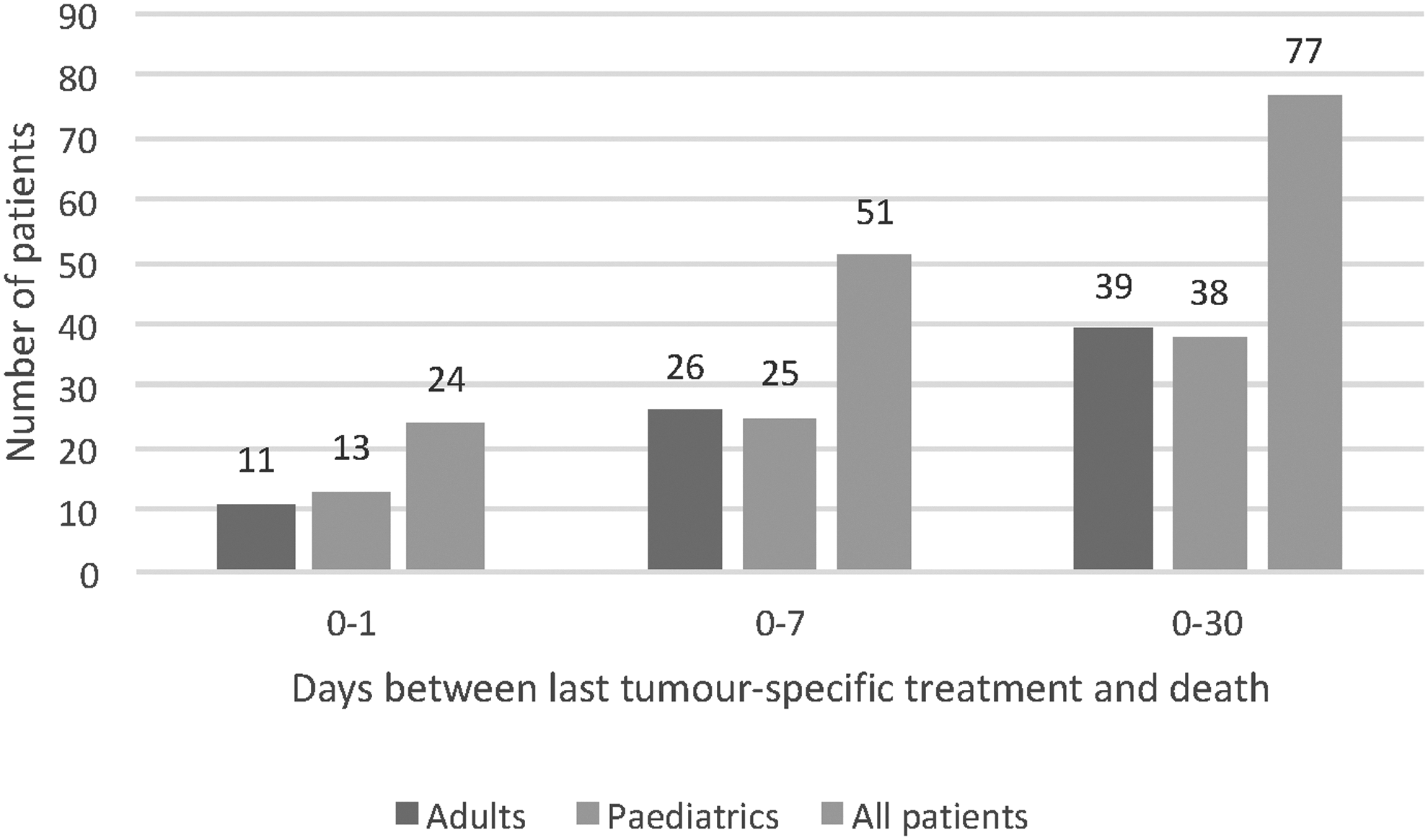
Number of patients treated with tumor-specific treatment on the day of their death or 1 day before (0–1), within the last 7 days of life (0–7), and in the last 30 days of life (0–30).
CT was given to 36 of the 39 adult patients and to 36 of the 38 pediatric patients who received tumor-specific treatment in the last 30 days of life. RT was given to 11 adults and 4 pediatric patients (Fig. 4). Among these patients, eight adults and two pediatric patients received both CT and RT. The tumor-specific treatment given to the 11 adult patients and 13 pediatric patients on the day of death or one day before death, was CT for 9 adults and 12 pediatric patients. The other two adults and one child received RT.
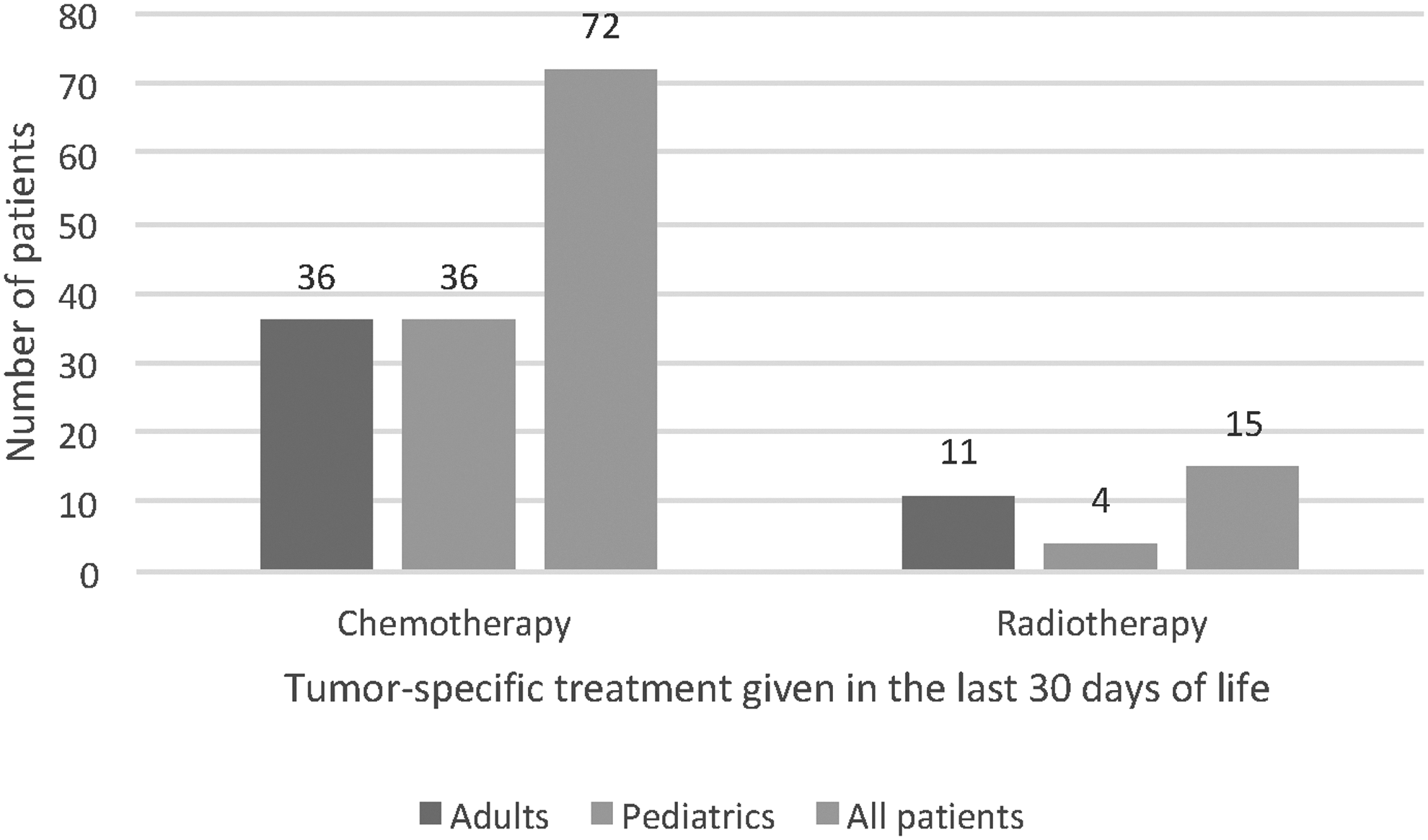
Number of patients receiving CT and RT in the last 30 days of life. Among these patients, eight adults and two pediatric patients received both CT and RT in the last 30 days of life. CT, chemotherapy; RT, radiotherapy.
The last CT dose given was administered intravenously in 33/36 adult patients and 29/36 pediatric patients, and orally in 4 adults and 10 children (Fig. 5). Of these patients, one adult and three children received both oral and intravenous CT as their last treatment. The median number of days between last CT dose and time of death was 6 days (0–27 days) for the patients who received intravenous CT, and 1 day (0–18 days) for the patients who received oral CT.
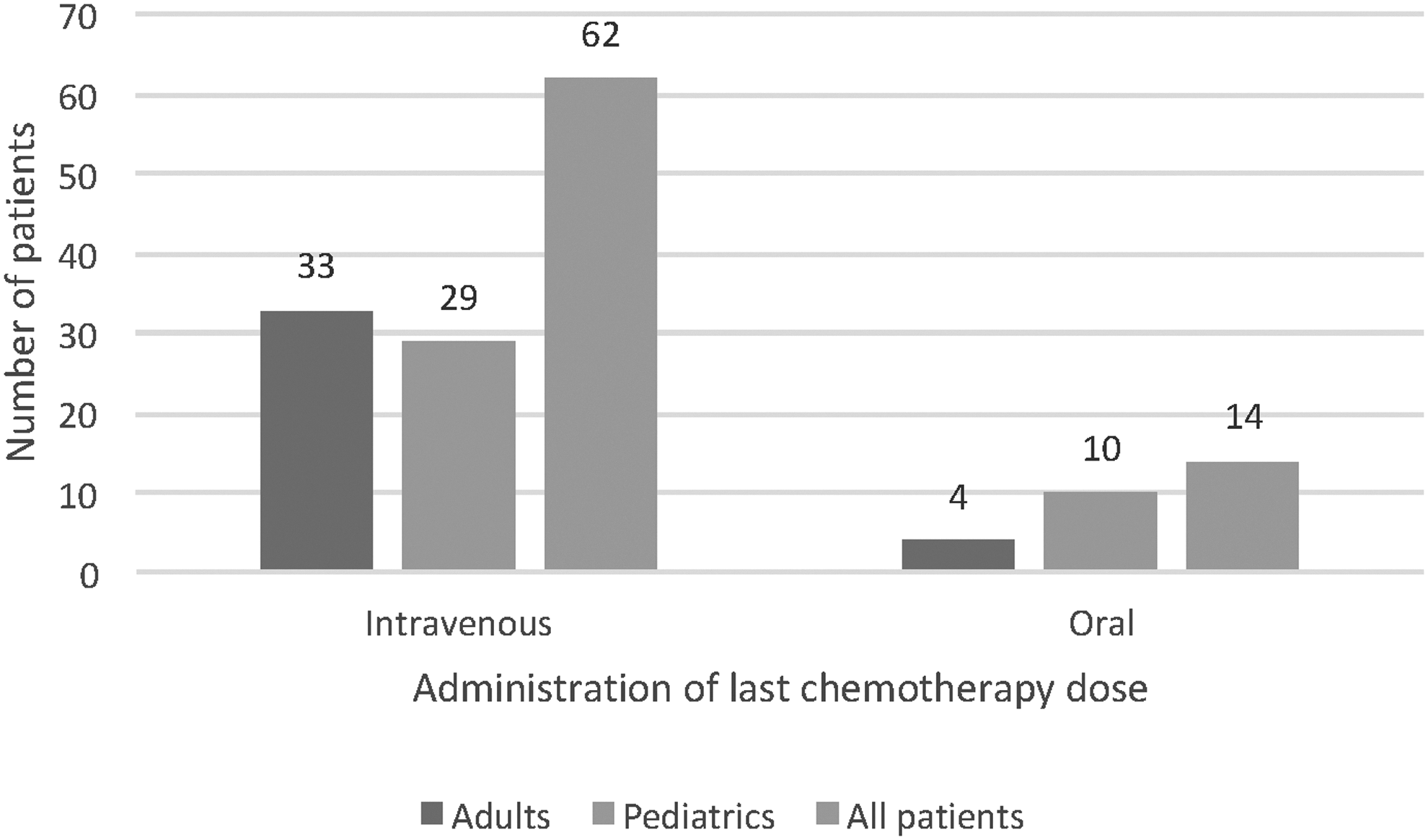
Administration of the last CT dose given in the last 30 days of life. One adult patient and three pediatric patients received both intravenous and oral CT as their last treatment.
Of all 50 patients with hematological malignancies, 41 patients (82%) received tumor-specific treatment in the last 30 days of life. In the group of patients with solid tumors (n = 46), 36 patients (78%) received tumor-specific treatment in the last 30 days of life (Fig. 6).
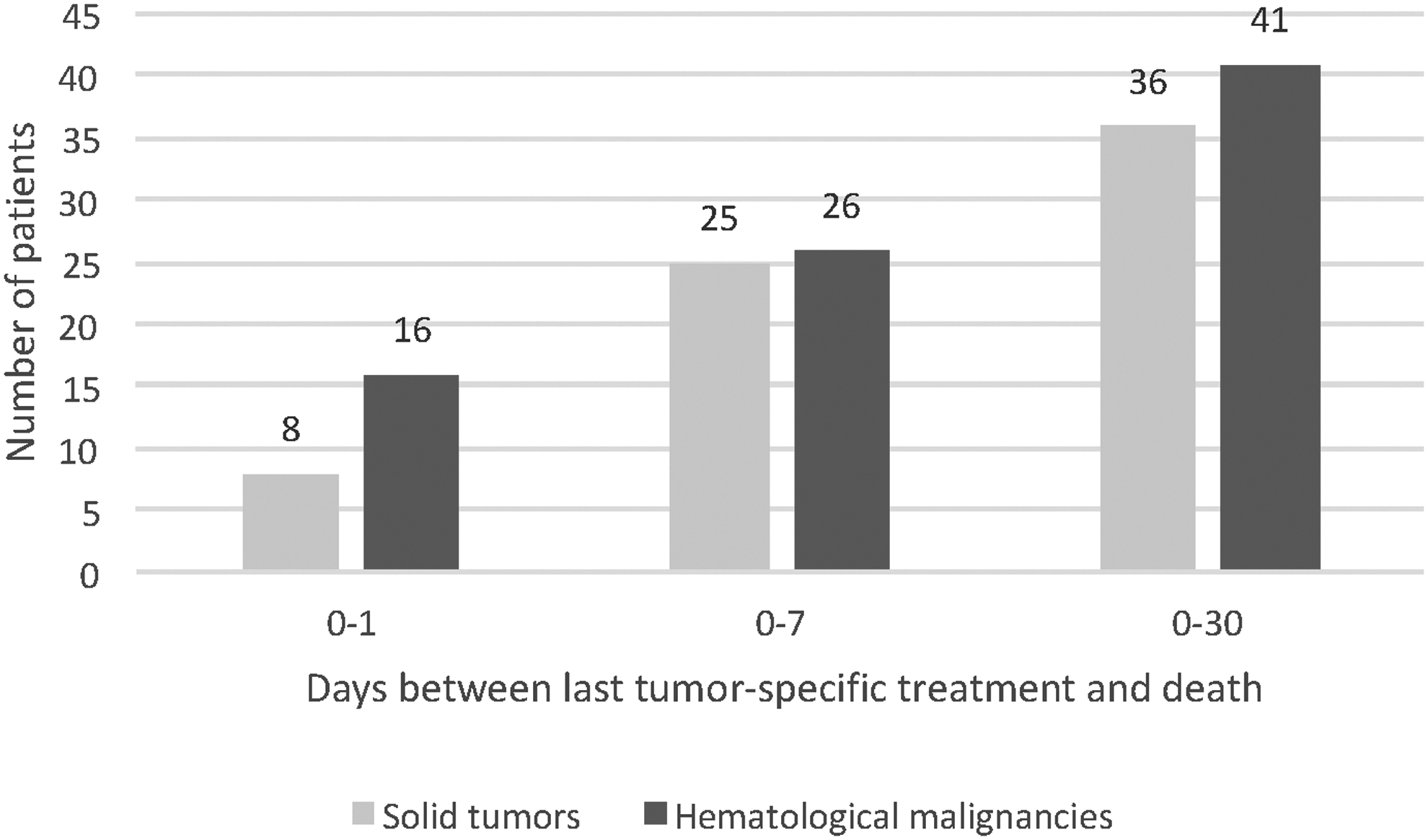
Number of patients treated with tumor-specific treatment on the day of their death or one day before (0–1), within the last 7 days of life (0–7), and in the last 30 days of life (0–30), comparing solid tumors with hematological malignancies.
Treatment intention
In this retrospective study, the aim of the tumor-directed treatment was stated in only a few cases. In three of the four children receiving RT in the last month of life, the aim was recorded as palliative and the corresponding figure for adults was in five of the 11 RT treatments. CT was given with a palliative intent in 7 of the 36 adult patients receiving treatment in the last month of life. In the pediatric patients the intent of CT was not stated in the medical records. The prognosis of the patients was discussed in 33 of the 52 adults and in 34 of the pediatric patients.
Causes of death
Causes of death were not noted in the medical records. No resuscitations, nor invasive life- saving treatment were performed. No intensive care transfers were undertaken. Intensive EoL care is not performed at the hospital. The symptoms during the last day in life were recorded, in adults, mainly as shortness of breath and varying levels of unconsciousness and in the children as fever, seizures, and bleeding. Data are not shown.
Referral to the specialized PCU
Twenty-six of the 52 adult patients (50%) and 25 of the 44 pediatric patients (57%) had been referred to the PCU for specialized symptom management, before or during the last month in life. The median number of days between referral and death was 11 days (0–42 days) for the adults (with two outliers excluded) and 14 days (0–78 days) for the pediatric patients (with four outliers excluded). In four cases, the specific date for referral to the PCU was not found. Pain was the most common reason for referral for both adults and for the children (n = 20 and n = 19, respectively).
Among the 77 patients who received tumor-specific treatment in the last 30 days of life, 42 patients (19/39 adults and 23/38 pediatric patients) had been referred to the PCU. Of the 24 patients who received tumor-specific treatment on the day of death or one day before, 7 patients had been referred to the PCU and 17 had not been referred (Fig. 7).
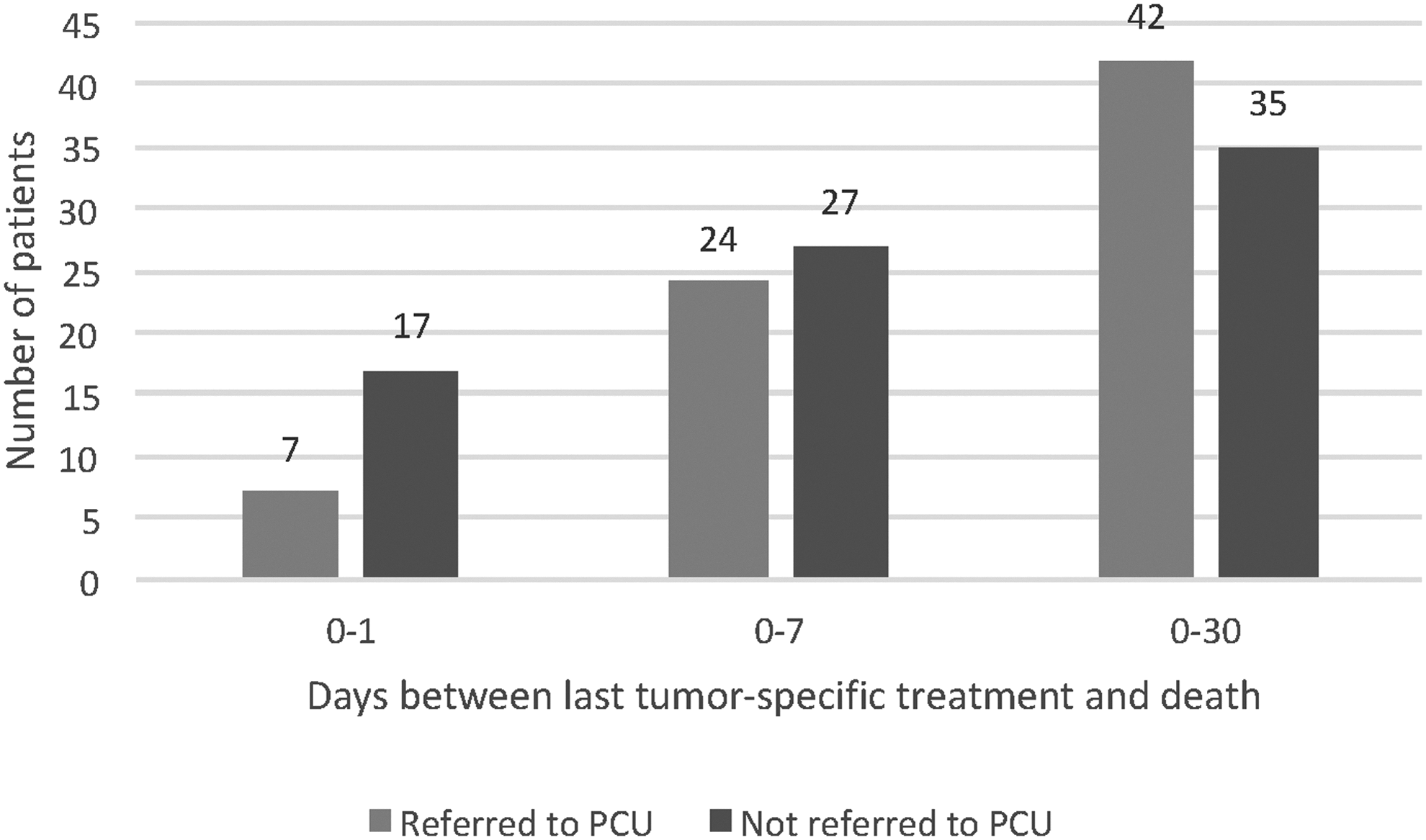
Number of patients and days between last tumor-specific treatment given, 0–1, 0–7, and 0–30, respectively, and relationship to whether a referral to the PCU was done. PCU, palliative care unit.
Discussion
Tumor-specific treatment
At the governmental cancer hospital where the present study was performed, 77 of 96 patients (80%) received tumor-specific treatment during the last 30 days of life. In other studies, corresponding numbers vary between 20% and 56%.5–8 However, only one study from India assessing tumor-specific treatment close to death was found. This study from New Delhi reported that 71% of 259 patients died within 90 days after receiving CT, RT, surgery, or stem cell transplant. 17 In two studies of older patients (above 65 years and a median patient age of 61 years, respectively) low numbers, such as 4% and 9% of the patients, were reported being treated with tumor-specific treatment close to death. The authors of these studies concluded that they saw a trend to lesser use of CT with increasing age and that younger patients thus might be treated more aggressively.18,19 Patients with hematological malignancies is another patient group with a higher risk of receiving aggressive EoL care.9,18 However, in the present study, with a small number of patients included, this differences in EoL care could not be reproduced.
The time elapsing between cessation of tumor-specific treatment and death might differ if the treatment is given intravenously or orally. Greer et al. found a difference with 49 days between last intravenous administration and death, but 24 days between treatment and death for orally administered drugs. 20 In the present study we saw a similar trend with a difference of 6 days between last intravenous administration of CT and death, and 1 day between last oral administration and death. Oral tumor-specific treatment might be perceived as less aggressive compared with intravenous treatment, explaining why oral administration of tumor-specific treatment more often is given to patients close to death.
Treatment-related side effects can increase overall morbidity and contribute to an earlier death in treated patients compared with when no tumor-specific treatment is given. According to two studies from the United Kingdom and Japan, 7.5% and 2.3%, respectively, of all the deaths were considered to be related to CT or RT given, either palliatively or curatively intended.21,22 In the present study, this could not be analyzed, although we found in an earlier nonpublished bachelor thesis (Lund University, Faculty of Medicine, Sweden 2015) that in children with acute myeloid leukemia (AML), death during the induction phase of CT was seen in 19 of the 45 children, thus a treatment-related morbidity can be suspected. In a study by Wolfe et al., 23 it was reported that children with advanced cancer experience high suffering according to their own reports, and cancer-directed therapy contributes substantially to this suffering. This is important for physicians to consider when starting a tumor-specific treatment, especially when a chance of cure is not at hand, and where the effect of increased morbidity by treatment side effects may be life threatening.
Both CT and RT come with a risk of side effects that may severely compromise the QoL in a group of patients already in poor performance status. For this reason, all CT or RT given in the last 30 days of life was considered futile in this study. One could argue that a palliative RT given during the last month of life, could, in very selected cases, be of value if given in one or a few fractions, but this was not the fractionation pattern in this material. Many studies have shown the negative effects of CT and RT given close to death. Prigerson et al. 24 showed that although the meaning of palliative CT should be to improve QoL for patients with end-stage cancer, it did not improve quality of death (QoD) for patients with moderate or poor performance status and worsened the QoD for patients with a good performance status before therapy. Therefore, the conclusion was that QoD in patients with end-stage cancer is not improved, and can be harmed by CT use near death, even in patients with good performance status. Wright et al., as well as Wu et al., found that patients who receive palliative CT are more likely to receive intensive care, have an increased risk of undergoing cardiopulmonary resuscitation, mechanical ventilation, endotracheal intubation, and of dying in an intensive care unit, compared with patients not receiving tumor-specific treatment near EoL. Fewer of these patients also receive hospice care as compared with patients where less EoL CT is given.25,26
Both patients and physicians overestimate the antitumoral effect of palliative CT. Weeks et al. showed that 69% of patients with generalized lung cancer believed that there was a curative possibility with the treatment, as did 81% of patients with generalized colorectal cancer. 27 In a study from the United Kingdom, 161 patients (8.1%) died within 30 days of CT, whereof 12 with a potentially curative intent. 21 This was also the case among 27% of patients with solid tumors and 66% of patients with hematological malignancies in the study from New Delhi. 17 Physicians often overestimate the chance for tumor response and underestimate the risk of treatment-associated morbidity in their patients, 28 and do not recognize the patient being close to death. 29 Even when a poor prognosis is obvious, the discussion about changing the focus of the treatment from cure to symptom relief can be difficult for the physician. To recommend yet another line of tumor-specific therapy can be less challenging than to end active therapy and explain the benefits of best supportive care. Also the discussion of the poor prognosis and short life expectancy can again be postponed if continuing therapy. 9 The mere availability of many tumor-specific treatment options may by itself increase treatment aggressiveness, 28 which can be initiated both by the medical professionals or the patient and the family, all with unrealistic high expectations of the treatment effects. If there is no access to a PCU, physicians tend to continue to treat with CT longer than if there is a PCU to refer to. 9 The risk of receiving CT close to death reduces significantly if a decision, taken together with the patient and family, is made in advance when in the trajectory of the disease the tumor-specific treatment should be discontinued. 29
About half of the deceased patients in the present study had been referred for symptom management to the specialized PCU at the hospital, in line with a study from Japan, where 61% out of 72 patients had been referred to a palliative department. 30 Barriers to initiate SPC are many. Reasons, aside the uncomfortable discussion, can be cultural, when the poor prognosis is not to be talked about, or when lack of financial resources for the patient and family limits the access to care, two of the major causes for a delayed or nonexistent PC. 16 Studies have reported the median duration of survival after referral to PC being 18–20 days.31,32 In the present study, these figures were 11 days (0–42 days) for adults and 14 days (0–78 days) for children. When asked for the appropriate time of referral to SPC, physicians in PC would recommend referral around three months before death, 33 although with optimized care, a good death can be achieved even within a short period of time. 32
Early referral to PC is associated with less aggressive EoL care in the last 30 days of life, with significantly lower rates of emergency ward visits, hospital admissions, and hospital deaths. 19 Contact with PC has also been shown to reduce the risk of receiving CT in the EoL.20,30,34,35 This is in concordance with the present study, where patients who had been referred to the PCU were less likely to have received tumor-specific treatment in the last few days of life (Fig. 7).
Only a few studies on PC in LMIC are published. A comparison of figures between the results in the present study, from a low-resource setting in an LMIC, and earlier published studies from HIC, is hardly meaningful. The healthcare resources and the availability of PC for the majority of patients in LMIC as well as the very contents of PC are very different from HIC. Literacy, awareness, and cultural beliefs are some of the factors that will affect how PC is received in a society and among the patients.
Conclusion
The majority (80%) of the patients in this study had received tumor-specific treatment in the last 30 days of life at this low-resource cancer hospital in an LMIC. Around half of all patients had been referred for contact with a specialized PCU, during the last weeks in life. QoL near death could not be determined in this retrospective study. To encourage the discussion and awareness of when to discontinue futile treatment and provide best supportive care is in the interest of the patient, the family, and the healthcare system. This applies for all countries and particularly in low-resource areas, such as in the present study, where optimized distribution and use of the limited healthcare resources is even more important.
Footnotes
Acknowledgments
The authors would like to acknowledge the MNJ Institute of Oncology and Regional Cancer Center (MNJIORCC) Hyderabad, India, and Lund University, Sweden, for making this study possible. They would like to acknowledge and thank Ms Vineela Rapalli, Mr Fazil, Ms Sunitha, Ms Pavitra, Ms Navatha, and the staff at the Department of Pain and Palliative care at MNJIORCC.
Author Disclosure Statement
No competing financial interests exist.