
Abstract
Abstract
Background:
Despite the increase in the identification of patients at the end of life after the introduction of rapid response team (RRT), there is doubt as to whether there has been an improvement in the quality of care offered to these patients. Proper end-of-life care is the next expected step after identifying patients who are dying.
Objective:
To evaluate the end-of-life care after limitations of medical treatment (LOMTs) as defined by an RRT.
Design:
This is a single-center retrospective cohort study at a tertiary teaching hospital in Porto Alegre, Brazil, from July 2014 to July 2016.
Setting/Subjects:
We included 242 patients with an LOMT as defined by the RRT.
Measurements:
Outcomes of interest included symptoms and palliative measures after RRT review.
Results:
During the study period, there were 5396 calls to 2937 patients, representing 126 calls per 1000 hospital discharges. Of these calls, 4.9% (n = 242) resulted in an LOMT. The primary care team agreed with the LOMT decision proposed by the RRT in 91.7% of cases. Regarding end-of-life symptoms, 7.4% and 5.8% of patients presented with intense or moderate pain, respectively, and 62.4% of patients presented dyspnea in the last 48 hours of hospitalization. Less than 15% of patients received attention for their spiritual needs and/or received psychological support.
Conclusions:
Our data reinforce the important role of RRTs in the identification of end-of-life patients with clinical deterioration. Despite the increase in the identification of these patients, the quality of end-of-life care needs to be improved.
Introduction
R
Despite the increasing involvement of RRTs in end-of-life care, controversy exists regarding the benefits of this practice.8–10 In addition, we must address whether RRTs are the best tool for the identification and definition of limitations of medical treatment (LOMTs) of patients who are dying.11,12 After this definition, we have to offer adequate comfort care, with relief of symptoms. Therefore, the objective of our study is to evaluate the end-of-life care after LOMTs as defined by the RRT.
Methods
The study was approved by the institutional ethics committee under protocol number 1644421. The need for informed consent was waived.
This is a retrospective cohort study that evaluated patients treated by the RRT of the Hospital de Clínicas de Porto Alegre (HCPA) from July 2014 to July 2016. The HCPA is a public tertiary hospital with 842 beds and ∼30,000 hospitalizations annually.
The RRT of this institution was implemented in July 2014 and includes intensivists and internists with experience in emergency medicine; the RRT operates 24 hours a day, seven days a week. Care is provided by the RRT physician in conjunction with the ward staff. The system can be activated by any member of the hospital according to predefined criteria. Triggers for activating the RRT are based on acute changes in heart rate (<40 or >140 beats per minute), systolic blood pressure (<80 mmHg or between 80 and 90 mmHg with symptoms), respiratory rate (<8 or >35 breaths per minute), level of consciousness (reduction in the Glasgow Coma Scale ≥2 points), oxygen saturation (<90%), risk of airway maintenance (need for intubation, tracheal aspiration, or tracheostomy care), prolonged seizures (greater than five minutes), or laboratory triggers (pH <7.3, bicarbonate <12 mEq/L, and lactate >3.0 mmol/L).
The study included all patients with an LOMT as defined by the RRT. LOMT was defined as withholding or withdrawing any form of life-sustaining treatment such as cardiopulmonary resuscitation (CPR), invasive and noninvasive mechanical ventilation, renal replacement therapy, and vasoactive and antimicrobial drugs. The collected data included demographic variables, comorbidities, functional capacity before admission, reasons for calls, goals of care, pain, dyspnea, and palliative measures. Pain level was assessed through the visual analog scale, with mild pain from 1 to 3, moderate pain from 4 to 6, and severe pain greater than or equal to 7. The patients were followed until the hospital outcome.
The data are presented as absolute numbers and percentages or as the means and standard deviations. A Kaplan–Meier survival curve was used in the analysis of the association of the intensity of analgesia with the risk of death in the 90 days of follow-up. Patients alive at the end of follow-up were censored (type 1 censoring). A log-rank test was used to compare survival rates according to the intensity of analgesia in the final 24 hours, and a p value <0.05 was considered statistically significant. The statistical analysis was performed with SPSS 20.0 software (SPSS, Chicago, IL).
Results
During the study period, there were 5396 calls to 2937 patients, representing 126 calls per 1000 hospital discharges. Of these calls, 4.9% (n = 242) resulted in an LOMT. Table 1 shows the demographic and clinical variables of the patients. Approximately one-third of the patients were already confined to the bed and more than half had a diagnosis of cancer. The number of deaths in the hospital during this period was 3468, which represented a mortality rate of 4.92%.
Demographic and Clinical Variables of Patients with a Limitation of Medical Treatment as Defined by the Rapid Response Team
EOL, end-of-life; ICU, intensive care unit; RRT, rapid response team.
Approximately two-thirds of patients (n = 160, 66.1%) had no information regarding the goals of care. In 19.0% of patients (n = 46), a full support goal was registered. For another 36 (14.9%) patients, there was a plan to discuss LOMTs, but without the definition of the goals of care. The patients who passed through the intensive care unit (ICU) or had a prior RRT review were analyzed, and we identified some differences. There was no information regarding the goals of care in 33 (53.2%) patients with prior ICU admission and in 127 (70.6%) patients without prior ICU admission (p = 0.05). This lack of information was observed in 66 (62.8%) patients with prior RRT review and in 95 (69.3%) patients without prior RRT review (p = 0.22). The primary care team agreed with the LOMT decision by the RRT in 91.7% of cases.
Hospital mortality rate was 84.3% (n = 204). The deaths occurred within the first 24 hours after RRT review in 27.9% (n = 57) of cases. Nearly half of the deaths occurred within the first three days after the LOMT definition (n = 101, 49.5%). Among the 38 patients who survived to discharge, 11 (28.9%) were still alive after six months.
Regarding end-of-life care, only 6.6% (n = 16) of patients were admitted to the palliative care unit. Palliative measures and treatment limitations are described in Table 2. Spiritual and psychological support for patients and their relatives was described in 1.2% and 13.2% of cases, respectively. In the evaluation of patients relative to pain management, 75.2% (n = 182) were without pain or unconscious, 7.4% (n = 18) reported severe pain, and 5.8% (n = 14) exhibited moderate pain. In 11.6% (n = 28) of the medical records, there was no description of pain control efficacy. The analgesic prescribed showed a dose–response curve relative to the outcomes of patients. The use of intermittent morphine resulted in a hazard ratio = 4.35 (95% CI: 2.88–4.66, p < 0.001), and morphine through continuous infusion resulted in a hazard ratio of 7.8 (95% CI: 5.76–8.13, p < 0.001) (Fig. 1). Regarding dyspnea, 151 (62.4%) patients presented this symptom, and 71 (29.3%) patients did not present it; in 20 (8.3%) patients, there was no description of the presence or absence of dyspnea.
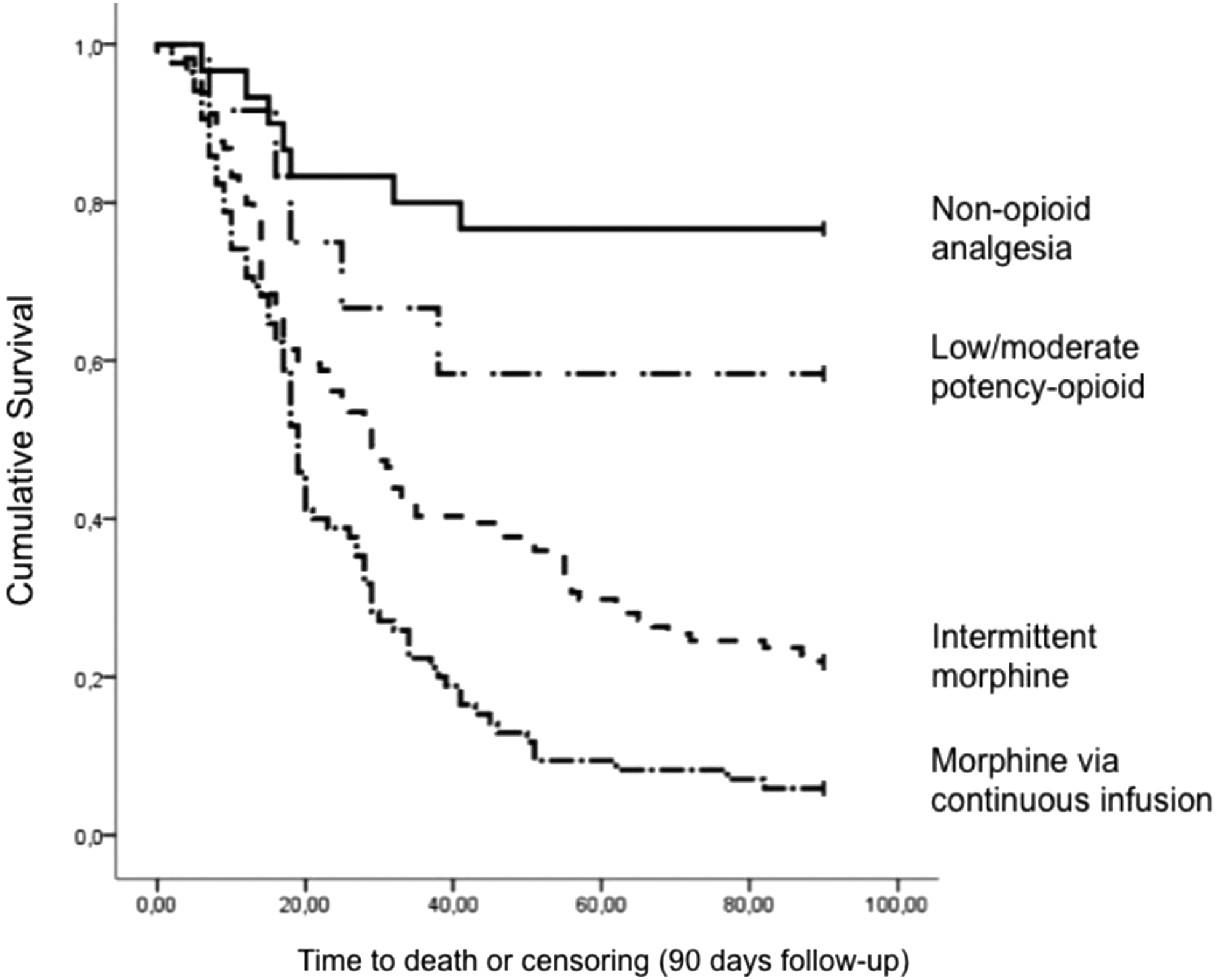
Kaplan–Meier plot of 90-day survival in the strata of the intensity of analgesia.
Palliative Measures and Limitations of Medical Treatment
Discussion
In this retrospective cohort study, we found that in 4.9% of RRT patients there was a new definition of LOMT, representing a new definition approximately every three days. Despite this change in the goals of care, 13% and 62.4% of patients still presented with moderate or severe pain and dyspnea, respectively, in their last days of life. In addition, most patients did not receive psychological and/or spiritual support.
Recent studies have shown the prominence of RRTs in end-of-life care beyond acute interventions for unstable patients.13–15 RRT triggers may represent unrecognized signs of gradual deterioration of a chronic disease in the later stages of the natural death process. 16 In this case, RRTs have the opportunity to recognize and treat patients who would benefit from end-of-life care. 15 Several studies have shown an increase in orders of nonresuscitation after the introduction of RRTs in hospitals.17–20 In a recent systematic review, LOMTs were established in 2% to 31% of RRT calls. 21 These findings highlight the role that RRTs have played in the care of patients at the end of life as a frequent tool for the identification of these patients.3,22 In our study, the primary care team agreed with the LOMT proposed by the RRT in 91.7% of cases. A similar rate was found in another study. 23 LOMTs are relatively heterogeneous among medical specialties, suggesting that there are benefits in including several physicians in the discussion of end-of-life care.24,25 Intensivists already play this role in the ICU and have an opportunity to apply this experience in other hospitalized patients through RRTs. 26 Despite this, in our study, more than half of the patients who passed through the ICU or had prior RRT review had no definition of the goals of care. Even intensivists are missing out on some opportunities, and there is room for improvement.
A discussion of end-of-life care initiated by the RRT, however, presents some possible disadvantages: the patient is generally not able to participate in the decision because he or she is experiencing severe instability, the RRT does not usually know the patient and the family sufficiently, and decisions are made at the time of crisis. 27 Ideally, patients should have the opportunity to discuss the goals of care before clinical deterioration, with their preferences clearly documented. 28
Despite the increase in the identification of patients at the end of life since the introduction of RRTs, there have been no consistent improvements in the quality of care provided to these patients. 10 End-of-life care requires more than withholding CPR. An order of nonresuscitation is an appropriate first step but should be followed by a discussion of treatment limits, preferential place of death, symptom control, attention to spiritual needs, and family support, among others.27,29 RRTs cannot be content to identify patients at the end of life without worrying about the care offered to these patients after this identification. Moderate or severe pain and dyspnea were observed in 13% and 62.4% of patients with a definition of LOMT in our study, respectively. Downar et al. found that 8% of patients died without receiving any palliative medication. 29 Regarding analgesia, we identified a dose–response association curve between intensity and mortality rate. Patients who received more potent medications were more likely to die, suggesting that analgesia may have been guided by variables other than the patient's level of pain. In addition, concern for spiritual and psychological support for patients and their relatives was even less evident. Less than 15% of patients and families received this support.
Limitations
This study was performed in a single center, so the results may be difficult to generalize. The retrospective design may have introduced a bias in obtaining the data. Some interventions, such as psychological and spiritual support for both a patient and his or her family, may not have been recorded in the medical record and may have consequently been underestimated in our study. However, we reviewed the records of all professionals involved in patient care, including those of psychologists. Any psychologist contact with a patient and/or family member and any mention of spiritual support or religious leader visitation were considered psychological and spiritual support, respectively.
Conclusion
Our data reinforce the important role of RRTs in the identification of end-of-life patients with clinical deterioration. Despite the increase in the identification of these patients, the quality of end-of-life care needs to be improved. Many patients are still dying with pain and dyspnea and without psychological and/or spiritual support. Further studies are needed to establish the role that an RRT should play in this scenario and to determine strategies to improve the quality of end-of-life care.
Footnotes
Author Disclosure Statement
No competing financial interests exist.