
Abstract
Abstract
Background:
Geographic disparities in access to palliative care cause unnecessary suffering near the end-of-life in low-access U.S. states. The psychological mechanisms accounting for state-level variation are poorly understood.
Objective:
To examine whether statewide differences in personality account for variation in palliative care access.
Design:
We combined 5 state-level datasets that included the 50 states and national capital. Palliative care access was measured by the Center to Advance Palliative Care 2015 state-by-state report card. State-level personality differences in openness, conscientiousness, agreeableness, neuroticism, and extraversion were identified in a report on 619,387 adults. The Census and Gallup provided covariate data. Regression analyses examined whether state-level personality predicted state-level palliative care access, controlling for population size, age, gender, race/ethnicity, socioeconomic status, and political views. Sensitivity analyses controlled for rurality, nonprofit status, and hospital size.
Results:
Palliative care access was higher in states that were older, less racially diverse, higher in socioeconomic status, more liberal, and, as hypothesized, higher in openness. In regression analyses accounting for all predictors and covariates, higher openness continued to account for better state-level access to palliative care (β = 0.428, p = 0.008). Agreeableness also emerged as predicting better access. In sensitivity analyses, personality findings persisted, and less rural states and those with more nonprofits had better access.
Conclusions:
Palliative care access is worse in states lower in openness, meaning where residents are more skeptical, traditional, and concrete. Personality theory offers recommendations for palliative care advocates communicating with administrators, legislators, philanthropists, and patients to expand access in low-openness states.
Introduction
To mitigate geographic disparities in access to palliative care, there is a need to understand psychological mechanisms that impede the development of palliative care programs in low-access regions. Geographic disparities in access to palliative care have been well documented, both cross-nationally1–5 and within individual countries.6–9 Within the United States, for example, nearly 90% of hospitals in the northeastern states have palliative care programs, but fewer than half of hospitals in the Deep South have palliative care programs.9–11 Given that palliative care programs have been shown to improve quality-of-life for patients and family caregivers,12–14 reduce costs,15–17 and prolong patients' survival in certain contexts,18,19 the lack of access in some states is a source of needless suffering for patients dealing with serious illnesses.
We hypothesized that geographic disparities in access to palliative care could be accounted for by geographic variation in personality, with implications for improving access in current low-access states. Psychologists use the term personality to refer specifically to an individual's relatively enduring patterns of thought, feeling, and behavior.20,21 The well-established Five Factor Model 20 of personality indicates that most variation in personality is accounted for by five core personality dimensions: openness, conscientiousness, agreeableness, neuroticism, and extraversion. Personality differs across geographic regions, and state-level variation in personality has been shown to predict important societal outcomes as personality affects the overarching cultural norms, attitudes, mores, opportunities, and available institutions within regions.22–24 Given the common framing of medicine as a battle waged against disease, noncurative efforts to palliate symptoms could be considered unconventional in some states, and therefore vary based on state-level cultural factors such as the personality of the region.
We predicted that states with residents higher in openness and conscientiousness would have better access to palliative care. Individuals high in openness are curious, flexible, imaginative, novelty-seeking, and willing to try new things,20,21 and they are more accepting of novel medical care. 25 Also, states comprised individuals higher in openness are more likely to have enacted physician aid in dying legislation, 26 suggesting a willingness to experiment with offering different models of serious illness care, even controversial ones. Accordingly, we anticipated that the cultural mindset of states higher in openness might facilitate greater acceptance of providing and utilizing palliative care. Moreover, individuals high in conscientiousness are more industrious, efficient, dutiful, and planful.20,21 They invest in behaviors that foster long-term positive outcomes, 27 especially engagement in proactive health behaviors. 28 Findings at the state level have been inconsistent, although some research suggests states with more conscientious residents may see increased income, social capital, and longevity. 29 Conscientious states may espouse cultural values that emphasize following rules and guidelines, perhaps including medical guidelines for quality care, and reinforce the allocation of resources toward program development, including in palliative care. Personality theory offers many recommendations for how to relate to people with particular personality characteristics,30–32 including individuals or groups who are less open or conscientious. Accordingly, findings could help advocates of palliative care to frame services more effectively when communicating with hospital administrators, legislators, philanthropists, and patients who are reticent to develop new programs in low-access geographic states.
In the present investigation, we used several public datasets that provided data on personality, palliative care access, and key covariates for each of the 50 U.S. states and the national capital. We hypothesized that palliative care access would be greater in states where residents were higher in the personality dimensions of openness and conscientiousness.
Methods
Procedure
We began by linking 5 public datasets that provided state-level data for the 50 states and the national capital that pertained to access to palliative care, personality, or key demographic covariates. Data sources included the Center to Advance Palliative Care (CAPC) 2015 State-by-State Report Card, 9 a published report on personality norms, 24 the U.S. Census Bureau 2015 American Community Survey, 33 and the 2015 Gallup Daily Tracking Survey. 34 We conducted a sensitivity analysis that incorporated additional data from CAPC 9 as well as U.S. Census of 2010 35 that offers additional variables beyond the annual 2015 survey. None of the datasets included identifying information, so our analyses were not subject to ethical review by an Institutional Review Board.
Measures
Palliative care access
The 2015 CAPC Report Card 9 provides palliative care “access grades” for each state and the national capital, which simply indicate the percentage of hospitals within each state that have palliative care programs. CAPC is a leading palliative care advocacy organization in the United States and regularly compiles relevant data for public education campaigns. For the Report Card, CAPC compiled data from the American Hospital Association Annual Survey Database and the National Palliative Care Registry. The CAPC estimates are based on an overall sample of 2393 hospitals that have ≥50 beds.
Personality
We extracted state-level data on the Big Five personality dimensions from national norms reported by Rentfrow et al. 24 In that investigation, a sample of 619,387 U.S. adults completed the well-validated 44-item Big Five Inventory 36 via the internet between 1999 and 2005. The study was open-access and one of the first large-scale studies to provide participants with scientifically valid customized personality feedback based on their survey responses, a noteworthy incentive that made it one of the largest studies of personality all-time. In the published report, the authors provided the average score as a continuous variable for each personality dimension for each state and the national capital. Each state was well represented with at least 1500 participants.
Covariates
Drawing upon the previous literature,11,37–40 we controlled for key demographic covariates that could be associated with personality, palliative care access, or both. State-level data on population size, age, gender, race/ethnicity (% white and non-Latino/a vs. all others), education (% with at least a Bachelor's degree), poverty status (% above the poverty line), and median income were downloaded from the U.S. Census Bureau's public database for the 2015 American Community Survey, 33 which sampled >2.3 million U.S adults. To avoid reducing statistical power by including too many covariates in our model, we combined three of these variables (education, poverty status, and income) into a single indicator of socioeconomic status that was simply the standardized average of the three, such that higher scores indicated higher socioeconomic status in the state. Because the U.S. Census does not track political views, we used published results from the 2015 Gallup Daily Tracking survey, 34 a telephone-based poll of >175,000 U.S. adults to measure each state's political orientation. This was quantified as the proportion of residents of a state identifying as liberal minus the proportion identifying as conservative, such that more extreme positive numbers reflected more liberal states and more extreme negative numbers reflected more conservative states. Previous studies have used comparable methods of measuring socioeconomic status (SES) 11 and political orientation. 26 In a post hoc sensitivity analysis, we used the CAPC data 9 to control for the proportion of hospitals within each state that were nonprofit and the proportion with at least 300 beds, and we used U.S. Census data 35 to control for state-level differences in rurality.
Statistical analyses
All data were analyzed using SPSS Statistics 22.0. First, we linked the datasets from different sources to yield a master dataset. Then, we examined the distribution of each variable using descriptive statistics and examined the unadjusted associations among variables using correlations. Multiple regression was used to evaluate the study hypotheses. The dependent variable was the CAPC palliative care access grade. The five personality dimensions were included in the model simultaneously as independent variables, and covariates included each state's population, median age, the proportion of female residents, the proportion of white non-Latino/a residents, the composite indicator of socioeconomic status, and average political orientation. In a sensitivity analysis, we additionally controlled for the proportion of hospitals in each state that were nonprofit, the proportion of hospitals with at least 300 beds, and the proportion of residents living in a rural setting. As these were exploratory analyses of secondary data, we used two-tailed alpha levels of 0.05 for all inferential statistical tests rather than a more conservative approach that would increase the risk of type II errors. In response to reasonable requests, we will make the study data available for independent replication or further collaborative efforts.
Results
Descriptive analyses
Table 1 summarizes descriptive state-level data for all variables included in our analyses. As indicated by the CAPC grades, states varied in terms of access to palliative care with a range of 25%–100% of hospitals in each state having a palliative care program. The geographic landscape of this variation in access is depicted in Figure 1A. Each of the state-level personality scores demonstrated a reasonable range of variability (Table 1).

Access to PC and state-level personality across the United States.
State-Level Descriptive Statistics
Analyses include the 50 states and the national capital of Washington, D.C.
The CAPC assigned a grade to each state indicating the percentage of its hospitals that had palliative care programs.
Values have been standardized to the T-score distribution (i.e., M = 50, SD = 10) to ease interpretation. For example, a score of 80 means 3 SD above the mean, and a score of 45 would mean 0.5 SDs below the mean.
Proportion of residents identifying as a liberal minus the proportion identifying as a conservative. For example, higher positive values indicate more liberal states, and more extreme negative values indicate more conservative states.
CAPC, Center to Advance Palliative Care; SD, standard deviation.
In correlational analyses, as hypothesized, states with higher levels of openness (Fig. 1B) were found to have greater access to palliative care (r = 0.389, p = 0.002; Fig. 2). Contrary to hypotheses, conscientiousness was not associated with greater access to palliative care (r = −0.144, p = 0.313). Neither were the other personality variables. However, access to palliative care was higher in states where residents were older (r = 0.330, p = 0.009), white and non-Latino/a (r = 0.234, p = 0.049), higher in socioeconomic status (r = 0.574, p < 0.001), and more politically liberal (r = 0.575, p < 0.001), thus supporting the rationale of controlling for these variables in regression analyses.
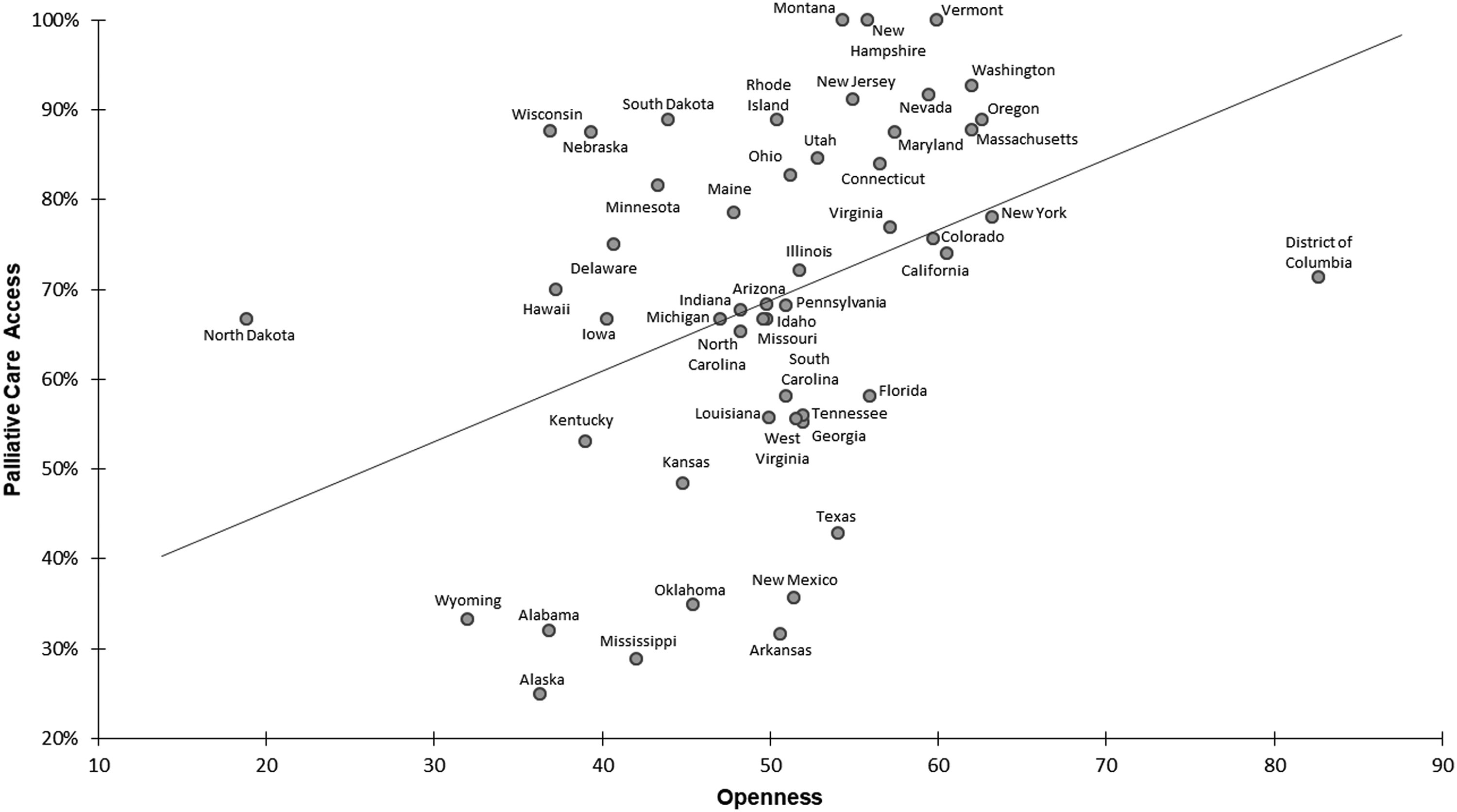
Correlation between openness and palliative care access. As shown in the scatterplot, states with higher levels of openness experienced greater access to palliative care (r = 0.389, p = 0.002). Moreover, this finding persisted in covariate-adjusted analyses (β = 0.428, p = 0.008) that controlled for state-level differences in age, gender, race/ethnicity, socioeconomic status, political views, and population size.
Hypothesis-testing in regression analyses
As hypothesized, states higher in openness had increased access to palliative care (β = 0.428, p = 0.008), while controlling for state-level differences in age, gender, race/ethnicity, socioeconomic status, political views, and total population levels. Although not hypothesized, higher levels of agreeableness were also associated with increased access to palliative care (β = 0.350, p = 0.029). None of the covariates was significantly associated with palliative care access when accounting for personality and the other covariates in the model.
In the post hoc sensitivity analysis, we continued to find that palliative care access was greater in states higher in openness (β = 0.395, p = 0.003) and agreeableness (β = 0.362, p = 0.005). Palliative care access was higher in states with more nonprofit hospitals (β = 0.532, p < 0.001) and lower rural populations (β = −0.310, p = 0.018), but did not differ according to the other personality variables or covariates.
Discussion
The present study provides evidence that state-level differences in personality are associated with variation in access to palliative care. Specifically, as hypothesized, based on personality theory,25,30–32 access to palliative care was better in states where residents were higher in openness—people who are curious, flexible, and creative, and like hearing new ideas and trying new things. As previous studies have often emphasized institutional rather than cultural factors implicated in access to palliative care, it may seem surprising that statewide differences in personality account for variation in palliative care access, especially given the magnitude of the effect we observed, and this highlights the need for more research on personality in the field of palliative care. Findings also have implications for palliative care clinicians and health policy advocates seeking to increase access to palliative care in low-openness states.
Personality theory can help advocates of palliative care to understand the cultural mindset of residents of low-access geographic states. Of the states with the lowest palliative care access, most were occupied by residents who were low (Wyoming, Alabama, Alaska, Mississippi, and Oklahoma) or moderate (Arkansas, New Mexico, and Texas) in openness (Fig. 2). While palliative care can more easily flourish in high-openness states (e.g., Washington, Oregon, and Massachusetts) where residents have a greater interest in trying new ideas and programs, a different approach is needed to reach residents of states where the culture is less open. According to personality theory,30–32 less-open or “closed” individuals and groups tend to be more skeptical, traditional, and concrete.
Therefore, in marketing palliative care toward hospital administrators, legislators, philanthropists, and patients in low-access geographic states, it may be important for advocates of palliative care to communicate in ways that can effectively persuade people making decisions in cultural contexts that tend to be skeptical, prefer tradition, and desire concrete details—hallmarks of low-openness regions. Palliative care advocates can target skepticism by emphasizing the evidence for palliative care, such as meta-analyses, systematic reviews, cost-effectiveness studies, and national guidelines.13–17,40,41 Also, it would be helpful to frame palliative care by explaining how it is similar to more traditional or familiar services, such as pain and symptom management as well as coordination of care, and how these services often intend to preserve daily routines and traditions as long as possible. While the naming of palliative care programs has been hotly debated,42–46 calling programs by more traditional names, such as a “supportive care,” could curry favor in low-openness states. Finally, several reports47–49 have provided concrete details on the activities emphasized by palliative care clinicians. For example, one study 47 describing an outpatient program found that palliative care clinicians addressed symptom management in 75% of visits and coping in 64% of visits. Framing palliative care as a service that focuses on concrete and pragmatic activities such as managing symptoms and supporting coping could improve opportunities for development in low-openness and low-access states. These tips may be useful whether interacting directly with people who are low in openness themselves or even clinicians and administrators who—even if highly open themselves—may be cautious about developing palliative care programs in light of cultural norms and mores favoring skepticism, tradition, and the concrete in low-openness states. 24 Given that some states low in openness have managed to increase access to palliative care (e.g., South Dakota, Nebraska, Wisconsin, and Minnesota), these barriers are surmountable (for a statewide demonstration, see Ceronsky et al. 50 ).
Several additional findings on personality also warrant attention. First, although we hypothesized that states higher in conscientiousness would have better access to palliative care, that association is unsupported at this point of time. This may change in the future if hospital accreditation bodies increase standards of compliance for ensuring access to palliative care. Second, as anticipated, neuroticism and extraversion were not associated with palliative care access. Neuroticism could increase the need for palliative care but may also undermine motivation to develop programs, and extraversion has often had inconsistent associations with health behaviors. Third, an unanticipated finding was that states higher in agreeableness had better access to palliative care. It is possible that states where residents are less argumentative and more attuned to the suffering of others will support policies and institutions such as palliative care programs aimed at reducing suffering. One study 22 found that residents of more agreeable states engage in more behaviors that are associated with social reciprocity, a cultural value relevant to investing in palliative care and other social programs. However, our agreeableness finding should be interpreted with caution because the association was statistically significant in the covariate-adjusted analyses, but absent in the unadjusted analyses.
Although considered as covariates in our analyses, several of the demographic and institutional differences across states also accounted for variation in access to palliative care. Similar to a previous study, 11 we found that states with higher socioeconomic status had better access to palliative care, and we also found that states with older and more liberal residents had better access. However, these findings were no longer significant when accounting for personality. In our sensitivity analysis, we found that states with more nonprofit hospitals and fewer rural inhabitants had better access to palliative care, even when accounting for personality and demographic covariates. Others 10 have noted that the role of nonprofit hospitals in palliative care access warrants more attention. Moreover, more research is needed to evaluate novel models of palliative care, such as telehealth 51 and e-health 52 interventions, that could increase access for rural patients. It was notable that state-level differences in personality continued to account for variation in access to palliative care when controlling for each of these demographic and institutional characteristics, reiterating the importance of personality theory in this field of research.
Overall, this investigation was balanced by strengths and limitations. Foremost, the sample size of 51 geographic regions was an inherent limitation. Existing personality datasets with large sample sizes and geographic information emphasize higher order geographic units (i.e., states), which limits the number of units for analysis, but future studies could collect data across a higher number of lower order geographic units of analysis (e.g., communities), as this could increase statistical power. Second, while most of the datasets in this study were from 2015, the large national personality dataset only included data as recent as 2005. Although personality is thought by definition to be stable, given this time lag, it is possible that the observed effects may underestimate the real-world associations. Nonetheless, we also cannot rule out the possibility of systematic bias due to migration effects, cohort effects, or shifting political climates. Third, as our analyses focused on state-level differences, we caution against drawing strong inferences at other levels of analysis, such as how an individual's personality might influence attitudes toward palliative care. At the level of the individual, several studies have identified patient characteristics associated with attitudes toward palliative care.53–56 The present findings provide the impetus for future studies examining how the personalities of residents, health care providers, and hospital administrators may be associated with acceptance of palliative care. Such studies would help clarify how the personality culture of a state may contribute to institutional decisions surrounding the establishment and development of palliative care programs. Fourth, our analyses examined the independent contribution of each of the five personality dimensions to explaining state-level variation. Future studies could use novel statistical approaches (e.g., K-means cluster analysis) or groupings of similar states. 57 These limitations notwithstanding, a key strength of the study is the timeliness of the analyses, given national and international priorities focused on increasing access to and utilization of palliative care programs. Moreover, while geographic disparities in access to palliative care have been well documented, 9 an additional key strength of this investigation is that it is the first of its kind to attempt to account for substantive psychological characteristics that account for state-level variation.
In conclusion, access to palliative care is better in states where residents are higher in the personality dimension of openness. Personality theory suggests that to improve access in states where residents are low in openness, advocates of palliative care may wish to emphasize its evidence base, frame palliative care as similar to more traditional services, and describe palliative care in concrete detail, emphasizing its focus on symptom management and coping.
Footnotes
Acknowledgments
This research was supported by the National Institute of General Medical Sciences (U54GM104940) of the National Institutes of Health (U.S.). The authors conducted the research independently from the funder.
Author Disclosure Statement
No competing financial interests exist.