
Abstract
Abstract
Background:
Opioids are the foundation of treatment for cancer pain but can cause side-effects, one of the most common being nausea and vomiting, which can impair quality of life.
Objective:
To evaluate the evidence for the management of opioid-induced nausea and vomiting. This systematic review was undertaken as part of an update of the European Association for Palliative Care's opioid guidelines.
Design:
Searches of MEDLINE (1966–2017) and EMBASE (1980–2017) were done. Key eligibility criteria were: randomized controlled trials conducted in patients with cancer. The Grading of Recommendations Assessment Development and Evaluations system was applied to formulate recommendations.
Results:
Fifteen studies were eligible (1524 patients). The studies were grouped as follows: opioid switching (n = 8); the use of antiemetics to treat opioid-induced nausea and vomiting (n = 4); and change of route of administration of the opioid (n = 3). Three recommendations were formulated: A weak recommendation for switching from morphine to oxycodone in cancer patients with nausea (quality D); a weak recommendation for switching from tramadol to either codeine or hydrocodone for pain in cancer patients with nausea (quality D); and a weak recommendation for switching from morphine/oxycodone to methadone using the three-day switch method in patients with increasing pain considered untreatable with further opioid titration and/or with opioid-related side effects (quality C).
Conclusions:
This systematic review can make only weak recommendations for the management of opioid-induced nausea and vomiting. There remains a need for high-quality studies before strong recommendations on the management of opioid-induced nausea and vomiting can be made.
Introduction
O
The incidence of nausea and vomiting in patients treated with opioids for chronic pain in general is ∼40% and 15–25%, respectively. 3 In patients with chronic cancer pain, point prevalence of 25% (nausea) and 17% (vomiting) have been reported; 4 however, determining causality of nausea and vomiting is very challenging in patients with cancer.
Nausea and vomiting are distressing symptoms and may strongly impact on the quality of life. 5 In general, there are three approaches to the management of opioid-induced nausea and vomiting: opioid switching (replacing one opioid with another opioid to reduce opioid side effects); the use of antiemetics; and changing the route of administration of the opioid(s). 2 However, there is limited knowledge supporting these practices.
In 2009, the European Association for Palliative Care (EAPC) led a systematic review on management of opioid-induced nausea and vomiting. 6 This review informed their opioid guidelines, however, it demonstrated overall limited evidence in the field.6,7 Now, almost a decade later, these opioid guidelines are being revised and as such evidence on the management of opioid-induced nausea and vomiting is being updated to inform these guidelines. Therefore, the aim of this systematic review was to evaluate the current evidence for the management of opioid-induced nausea and vomiting, and to formulate treatment recommendations when appropriate.
Materials and Methods
Ethics approval was not required for this systematic review. The electronic bibliographic databases MEDLINE (1966 to November week 50, 2017) and EMBASE (1980 to November week 50, 2017) were searched in line with the EAPC guideline search strategy.
Search strategy
Due to the terminology used, that is, the ambiguity of nausea and vomiting-associated words, an extensive search strategy was used. Two separate searches were carried out for nausea and vomiting, respectively. In summary, free text and MeSH/EMTREE search terms were used, searches were limited to studies published in the English language and only randomized controlled trials (RCTs) were included. The search strategy is shown in Appendix 1 (Appendix 1 is available online at www.liebertpub.com/jpm). Hand searching of reference lists of included studies and review articles was also undertaken.
Eligible studies met the following criteria: patients with cancer; ≥18 years of age; on opioids (weak or strong opioid) as defined by WHO's Analgesic Ladder for cancer pain relief 1 ; nausea and/or vomiting assessed as a primary or secondary outcome; RCTs. Studies were excluded if the nausea and vomiting was related to chemotherapy, radiotherapy, malignant bowel obstruction, or postoperative settings. Only primary studies were included.
Appraisal
Following the database search, the titles of all studies were reviewed and studies deemed not relevant were excluded. Following this, all abstracts of the remaining articles were reviewed and again nonrelevant studies were excluded. Subsequently, full-text studies were retrieved and evaluated.
The content and quality of these studies were assessed by two authors independently (T.S. and B.L.), using the Grading of Recommendations Assessment Development and Evaluations criteria. 8 The factors included study design; possible study limitations (allocations concealment, large losses to follow-up, no ITT analysis carried out, early stopping for benefit, and failure to report outcomes); participants; setting; and results. 8
Eligible studies were grouped into three categories according to the strategy described to prevent nausea and vomiting. These were as follows: studies on switching from one opioid to another; studies on antiemetics; and studies on change of administration route for the opioid(s).
Recommendations were developed based on the studies showing statistically significant change in symptoms. Each recommendation was graded according to the quality of evidence and classified as strong or weak. 8
Results
Figure 1 shows the selection of relevant articles. The search retrieved a total of 466 studies. Hand searching of reference lists of included studies, relevant chapters, and review articles revealed another 16 studies. Removal of 228 duplicates left 254 studies for further evaluation. The most common causes for exclusion were that the study examined nausea and vomiting induced by chemotherapy, radiotherapy, malignant bowel obstruction, or postoperatively; the study failed to report whether the patients were treated with opioids; and/or the study was not an RCT.
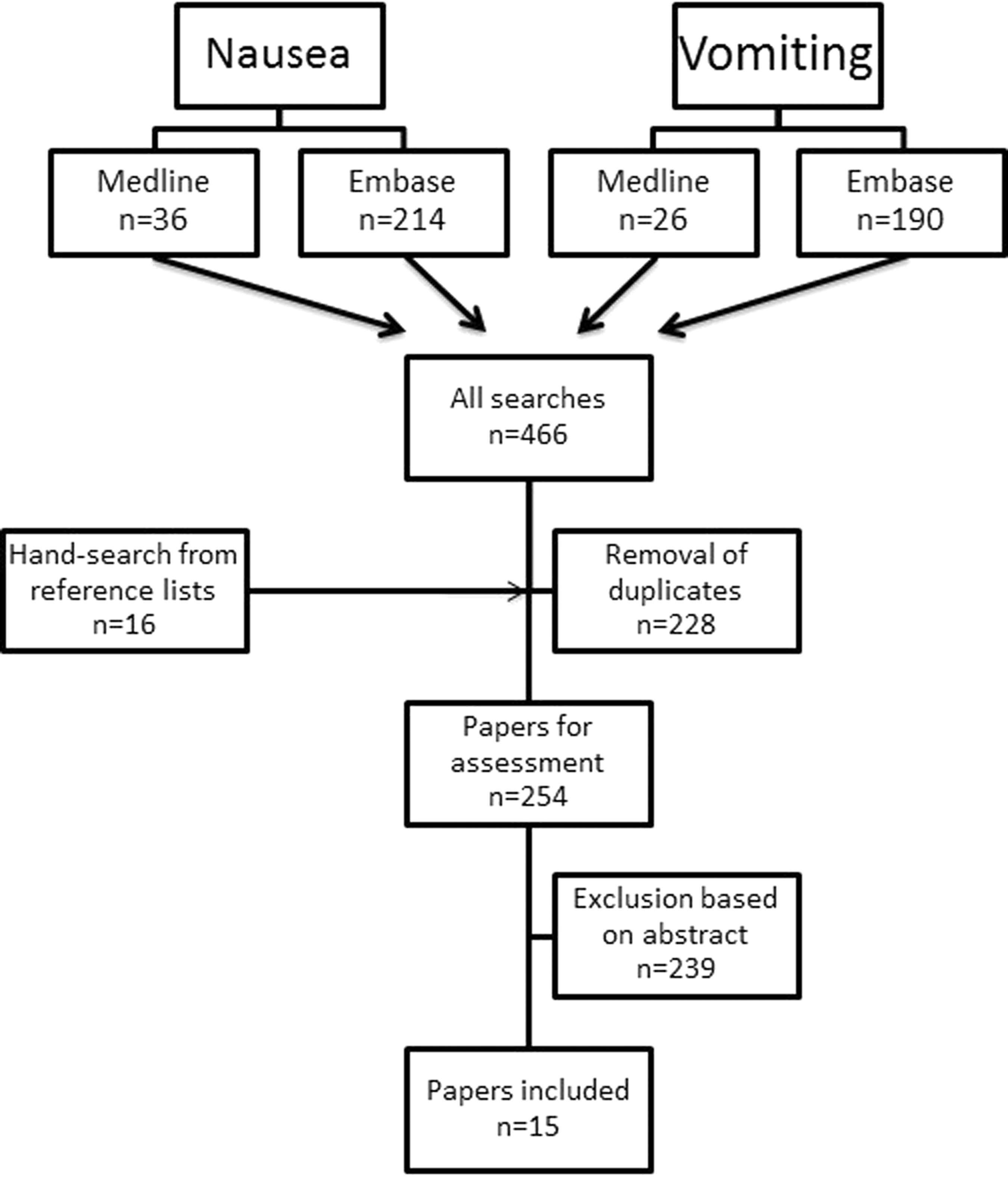
Selection of relevant articles.
Table 1 summarizes the 15 eligible studies (n = 1524). As discussed, these are now presented as per the method of treatment of opioid-induced nausea and vomiting.
Included Studies
ESAS, Edmonton Symptom Assessment System; NRS, numerical rating scales; PCA, patient-controlled analgesia; RCT, randomized controlled trial.
Opioid switch
Eight studies were retrieved discussing issues related to switch of opioids to improve control of opioid-induced nausea and vomiting.9–16 In all these studies nausea and/or vomiting was a secondary or tertiary outcome measure. Four studies were inconclusive or did not show any significant difference in nausea and/or vomiting between treatments.12,14–16
The study by Kalso and Vainio was a double-blinded crossover RCT, including 20 patients with cancer pain. 11 Morphine and oxycodone were administered orally and through a patient-controlled analgesia (PCA) device for 48 hours with each route of administration, before the treatment was swapped over to the other opioid for another 48 hours with each route of administration. There was “no significant” difference in pain intensity between treatments (p-value not reported), however, morphine administered through the oral route caused significantly more nausea compared with administration through a PCA device and compared with both routes of administration of oxycodone (p-value not reported).
The study by Rodriguez et al. was a multicenter, double-blinded RCT, including 177 patients with cancer-related pain. 9 Patients were randomized between three arms, receiving codeine, hydrocodone, or tramadol over the three week study period. No significant difference was found in proportion of patients with pain relief between the groups (p-value not reported). However, vomiting was experienced in a significantly larger proportion of the patients receiving tramadol compared with the two other treatment arms (p = 0.047).
Pace et al. examined 52 patients with cancer pain in an open-labeled RCT comparing treatment with transdermal buprenorphine in addition to tramadol, with treatment of sustained-release morphine in addition to tramadol. 13 Patients were observed for eight weeks and there was significantly lower pain intensity (p < 0.01) and fewer patients experiencing nausea (p = 0.042) in the buprenorphine arm, compared with the morphine arm. However, the numbers were small, with nausea experienced in three patients in the buprenorphine arm compared with nine patients in the morphine arm.
The study by Moksnes et al. compared a switch from morphine/oxycodone to methadone using the stop-and-go method with a three-day switch. 10 This was a multicenter, randomized phase II study examining 42 cancer patients with increasing pain considered untreatable with further opioid titration and/or with opioid-related side effects. No statistically significant differences were found between the methods of switching with respect to pain intensity (mean difference 0.5; 95% CI: 1.2–2.2), or nausea (mean difference 0.6; 95% CI: 1.1–2.1).
Nosek et al. conducted an RCT comparing oral controlled-release morphine and oxycodone with transdermal formulations of buprenorphine and fentanyl in the treatment of severe pain in 62 patients with cancer. 16 They assessed nausea using the Edmonton Symptom Assessment Score. The authors concluded that there was no difference in nausea severity between the opioids studied (no p-value reported); however, there was a tendency for a greater severity of nausea in patients treated with morphine.
The following recommendations can be made based on the studies that were eligible:
A weak recommendation is given for switching from morphine to oxycodone in cancer patients with nausea (quality D). A weak recommendation is given for switching from tramadol to either codeine or hydrocodone for pain in cancer patients with nausea (quality D). A weak recommendation is given for switching from morphine/oxycodone to methadone using the three-day switch method in patients with increasing pain considered untreatable with further opioid titration and/or with opioid-related side effects (quality C).
Use of antiemetics
Four of the studies discussed the use of antiemetics to improve control of opioid-induced nausea and/or vomiting.17–20 In these studies nausea and/or vomiting was examined as the primary outcome measure.
The study by Bruera et al. was an international, multicenter, double-blinded RCT examining 51 cancer patients with chronic nausea. 18 All the patients received metoclopramide for their nausea, but were randomized between two treatment arms, having either dexamethasone or placebo added to their metoclopramide treatment. The study demonstrated no difference between the dexamethasone and the placebo group in improving nausea (p ≥ 0.16). However, the study concluded that frequent assessment and continuation of metoclopramide for about one week may provide major symptom control in most patients.
The study by Hardy et al. was an international, multicenter, double-blinded RCT, including 92 patients with cancer. 17 Patients were randomized between three treatment arms: receiving ondansetron, metoclopramide or placebo for nausea, and/or vomiting following changes to their opioid treatment. The study found no significant difference between the arms in the proportion achieving complete control of nausea and/or vomiting in the 24-hour study period (p-value not reported). It concluded that neither ondansetron nor metoclopramide was more effective than placebo for opioid-induced nausea and/or vomiting. However, the study was terminated early due to difficulties recruiting patients, and the results must therefore be interpreted carefully.
Two studies by Mystakidou et al. compared treatment regimens of tropisetron to conventional treatment regimens with combinations of metoclopramide, chlorpromazine, and dexamethasone for nausea and vomiting in 280 and 160 patients, respectively.19,20 In both studies the patients were treated for cancer pain with morphine or dihydrocodeine at the point they were included, and nausea and/or vomiting was assessed during a 15-day period. In both studies patients experienced less nausea and vomiting in the arms receiving tropisetron.
None of these studies provided sufficient evidence to formulate any recommendations.
Change of route of administration
Three studies discussed a change of route of administration of a drug to improve control of opioid-induced nausea and vomiting.21–23 All studies compared treatment with morphine given by the oral route versus the rectal route, and nausea and/or vomiting was examined as the secondary or tertiary outcome.
The study by Bruera et al. was a double-blinded crossover RCT, where 30 patients with chronic cancer pain were included. 22 Treatment with morphine given subcutaneously was compared with morphine controlled-release suppositories and all patients received each treatment for a period of four days in random order. Nausea was not demonstrated to be significantly different between the two groups (p > 0.46).
De Conno et al. carried out a double-blinded, crossover RCT examining 34 patients with advanced cancer. 23 The study compared treatment with morphine given by the oral route with morphine given by the rectal route, and all patients received each treatment for a period of two days in random order. Intensity of nausea showed no significant difference between treatments (p-value not reported).
The third study was a double-blinded, crossover RCT by Babul et al. 21 Twenty-seven patients with cancer were included, and received morphine sulfate controlled-release tablets and morphine sulfate controlled-release suppositories for a period of seven days each in random order. Treatment with morphine sulfate controlled-release suppositories were shown to give significantly less nausea compared with the controlled-release tablets (p < 0.0065).
No recommendations could be formulated based on these results.
Although not eligible for inclusion in the present systematic review, a study by Wirz et al. is worthy of mention. 24 In a three-arm trial comparing transdermal fentanyl, transdermal buprenorphine, and oral hydromorphone, they observed that while overall nausea intensity did not differ between groups, patients using transdermal preparations had less nausea.
Discussion
This systematic review demonstrates an overall low quality of the existing literature on management of opioid-induced nausea and vomiting. This review updates a previous systematic review that appraised evidence up to 2009, and despite fifteen RCTs being included in the present review, only three weak recommendations were formulated.
High-quality studies take a long time to plan, set up and run, and one could argue that it is too early to see a response to the earlier recommendations for more high-quality studies in this area. However, there are several challenges that might explain the difficulties carrying out high-quality studies within this field. In general, it is well known that it is challenging to recruit patients in palliative care settings. This is due to the advanced nature of their condition, which may make it difficult for them to participate in clinical studies and the associated assessments. 25 For the same reason, attrition can be problematic. However, the need for symptom control studies in patients with cancer has been advocated. 26
One of the key challenges in this area is that patients with advanced cancer are complex and the etiology behind their nausea and vomiting is often multifactorial. Common causes include drugs such as opioids, delayed gastric emptying, mechanical bowel obstruction, increased intracranial pressure, vestibular dysfunction, metabolic problems, and cortical effects such as anxiety or depression. 27 It follows from this that it can be challenging to conclude from a study whether the management of nausea and vomiting yields opioid-induced nausea and vomiting in particular. This was also evident in the present systematic review.
Furthermore, to define the right endpoint for nausea and/or vomiting, and to use the right assessment tool to measure it, is challenging. Nausea, vomiting, and retching are separate entities; however, terms to describe them are often used interchangeably, resulting in imprecise assessment. 28 Nausea is a subjective feeling and needs to be reported by the patient. Several characteristics may be of importance: frequency; intensity; duration; quantitative; and qualitative aspects. 29 Many different assessment tools and endpoints are used. Three of the most common one-dimensional scales are visual analog scales, numerical rating scales, and verbal categorical scales. In addition, a number of global symptom assessment tools have been developed. 29 However, the ideal assessment tool has yet to be agreed on.29–31 It is also unclear as to the optimal period of assessment. While some tools assess the last three to six days, others assess the last 24- or 12-hour period. 30 Furthermore, there is no consensus whether nausea is best rated “right now,” “on average,” or “at its worst.” Altogether, the variety of assessment tools and endpoints for nausea and/or vomiting makes studies more difficult to interpret and compare.
Another challenge related to studies on opioid-induced nausea and vomiting is to predict which patients will be affected by this. It has been suggested that the following can be used to predict what patients are of greater risk: increasing age; gender (female); deteriorating physical status; type of opioid (opioids other than transdermal fentanyl); type of cancer (cancer of the female reproductive organs); as well as polymorphisms within the 5-hydroxytryptamine (serotonin) receptor 3B gene (HTR3B), catechol-O-methyltransferase gene, and cholinergic receptor muscarinic 3 gene. 32 Opioid-induced nausea and vomiting is common with the initiation of therapy, but is subsequently unpredictable with improvement in some patients and persistence in others.2,33 It can therefore be a challenge to recruit patients to studies, and the recruitment might need to happen more “ad hoc.”
In opioid-induced nausea and vomiting, the underlying mechanisms are only partly understood, but three main mechanisms are thought to be involved: opioids can directly stimulate opioid receptors in the chemoreceptor trigger zone in the medulla oblongata; they can bind to opioid-sensitive receptors and result in increased vestibular sensitivity; and they can act peripherally and affect receptors in the gastrointestinal tract.2,32,33 These complex underlying mechanisms behind opioid-induced nausea and vomiting make these symptoms also challenging to manage in clinical practice. For an antiemetic to be effective, it needs to antagonize the particular receptors stimulated by the opioid, and thereby relieve the opioid-induced nausea and vomiting. The antiemetic optimal for opioid-induced nausea and vomiting is not known and clinical practice is still partly based on expert opinion.
Future studies, which aim to examine opioid-induced nausea and vomiting, should clearly define the causal factors. First, to determine opioid as the precipitant, second, to examine whether opioid type, route, and/or dose are important factors. Detailed characterization of opioid-induced nausea and vomiting is a fundamental step before possible treatment strategies are examined.
Only three (weak) recommendations can be made regarding opioid switching in the setting of opioid-induced nausea and vomiting. No recommendations can be given regarding the use of antiemetics, or change of the route of administration of the opioid. Based on the existing evidence, it is still not known what the best approach is regarding these methods of management. The best practice for opioid switching, changing route of administration, and the optimal antiemetic, are all issues that need further examination. Whether one of these methods is better than the other is also unclear.
As for all systematic reviews, this has limitations associated with the search strategy. Relevant studies might possibly have been left out due to the exclusion criteria. Only RCTs were included in this study, possibly leaving other relevant studies out (e.g., observational). Language bias and publication bias can be present. The proposed recommendations are based on few publications, which are also associated with methodological limitations.
Conclusion
This systematic review can make only weak recommendations for the management of opioid-induced nausea and vomiting. The existing literature is of low quality and the challenges of researching this area are likely to have contributed to this. There remains a need for high-quality studies to be done before strong recommendations on the management of opioid-induced nausea and vomiting can be made.
Footnotes
Acknowledgment
Harriet Harris assisted with retrieval of articles. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.