
Abstract
Abstract
Background:
Code status discussions (CSDs) can be challenging for many clinicians. Barriers associated with them include lack of education, comfort level, and experience.
Objective:
To conduct an educational intervention to improve knowledge and communication approaches related to CSDs.
Design:
A cross-sectional multidisciplinary educational intervention was conducted over one year consisting of an interactive presentation, live role-play, and pre- and post-intervention tests to measure impact of the formal training. Evaluations and comments were also collected.
Setting/Subjects:
Attending physicians, nurses, residents, fellows, and physician assistants (PAs) at an urban community teaching hospital of 500 beds serving an ethnically diverse population.
Measurements:
Data from pre- and post-intervention tests evaluating knowledge and communication approach regarding CSDs were collected. Participants completed a qualitative evaluation of the program.
Results:
There were 165 participants: 29 attending physicians, 26 residents, 17 fellows, 18 PAs, and 75 nurses. All (100%) completed the pre-intervention test and 154 (93.3%) completed the post-intervention test. There was an overall improvement in scores, 43.8% pre-intervention to 75.6% post-intervention (p-values <0.005). Attending physicians and fellows had the highest pre-intervention scores, while nurses and PAs had the lowest. Most participants (97%) reported they learned new information and 91% stated they would change patient management.
Conclusions:
Our study found that a brief educational intervention with multipronged teaching tools improved knowledge concerning CSDs. Participants felt it provided new insights and would change their practice. This study contributes to the literature by examining CSD training across different disciplines, allowing for cross-group comparisons. Future studies should try to correlate educational interventions and clinician knowledge with clinical practice outcomes.
Introduction
Code status discussions (CSD
Televised cardiopulmonary resuscitation (CPR) outcomes are unrealistically successful (∼67%). 5 Actual success rates are between 15% and 20%6–9 and CPR may prolong the dying process in terminally ill patients.10,11 When describing CPR outcomes, physicians use vague language and seldom utilize validated tools that provide statistical information12–14 such as the good outcome following attempted resuscitation (GO-FAR) calculator. 15
Providing medical recommendations can be challenging. Physicians often dominate conversation time, missing key opportunities to allow patients or families to express thoughts.14,16 Residents feel underprepared to conduct CSDs due to lack of training.4,17–21 They may have CSDs without providing information on risks and benefits and not engage in shared decision making. 22
Sulmasy found that nurses were more likely than physicians to believe they should initiate do-not-resuscitate (DNR) discussions, more confident in their ability to discuss DNR than residents, but more likely to feel that it is not their role to recommend. 23 Surveys in conjunction with brief intensive exercises to address the need for formal CSD training have been used with medical students,24,25 residents,1,17,20,26,27 and physicians.18,28
Our study examined providing brief intensive education to clinicians of multiple disciplines and training levels to expand on previous findings. The objective of the intervention was to improve knowledge and communication approaches related to CSDs for various disciplines.
Methods
A cross-sectional educational intervention was conducted over a one-year period (September 2012 to September 2013) at New York-Presbyterian Queens (NYPQ), a 500-bed community teaching hospital serving a diverse patient population. The study consisted of an interactive presentation, with pre- and post-intervention tests to evaluate the impact of formal training across disciplines.
Subjects (Table 1) included internal medicine residents, nurses from various medical units, medicine physician assistants (PAs), attending physicians, and fellows from medicine subspecialties (cardiology, gastroenterology, pulmonary/critical care, nephrology, and infectious disease). Physicians practiced in outpatient and inpatient settings. Nurses and PAs were hospital based. Participation was voluntary.
Baseline Demographics of Participants
For attending physicians and nurses, we conducted a 30-minute educational intervention. Residents and PAs participated in a 45-minute session. Session duration varied due to provider availability, but education content remained standardized for all groups.
Session format was as follows: attendees took a five-question multiple-choice pretest, followed by the educational intervention, and followed by the same five questions administered as a post-intervention test (Table 2).
Questions Asked During the Pre-Intervention and Post-Intervention Tests
CPR, cardiopulmonary resuscitation; DNI, do-not-intubate; DNR, do-not-resuscitate.
Questions assessed knowledge about survival after CPR, risk factors associated with poor outcomes for survival to discharge after inhospital resuscitation (sepsis, renal failure, metastatic cancer, dementia, and functional status), and communication approaches. The questions were developed locally based on existing literature and pilot tested with a small group of multidisciplinary clinicians.
The educational intervention (Supplements A and B; Supplementary Data are available online at www.liebertpub.com/jpm) included a PowerPoint presentation covering CPR statistics, indicators for poor outcomes after inhospital CPR, a stepwise guideline for CSDs, and one live 5–7-minute role-play. It was highlighted that a DNR order is not equivalent to comfort care or “do not treat” the patient. 29
Following the session, participants evaluated the teaching program for usefulness and clinical applicability (Supplement C). The evaluation consisted of four questions: (1) were the educational objectives met; (2) was new information provided; (3) would this change how they would manage their patients; and (4) describe new insights gained?
Data from the test scores and program evaluations were entered into a database. Demographic information (age-range, gender, ethnicity), years of practice, and discipline were obtained before the intervention. The tests were scored from 0 to 100 points and an average score was calculated for each discipline. Individual comparisons over time could not be performed as the test scores and evaluations were anonymous.
The primary outcome for this study, both at pre- and post-intervention, was the overall percent correct across the five questions. Secondary analyses looked at the changes across time in individual questions. Analysis of variance was used to determine if there was statistically significant improvement in mean percent correct from pretraining to posttraining (factor “Time”). The analysis of variance model also included a term for “Group” and the interaction of Group by Time. By including a term for each group's average pre-intervention score and average post-intervention score, we could directly estimate the average improvement for each group, as well as compare improvement across groups. In this way, differential improvement in one group of responders compared with another could be tested. In the presence of a significant interaction, linear contrasts were estimated for prespecified pair-wise comparisons.
Pearson correlation was used to measure linear associations among the questions, to help determine degree of overlap in information queried by each question.
Parameter estimates are summarized by the mean and standard deviation or by the frequency and percent, and where appropriate, by 95% confidence intervals around the estimate. A p-value <0.05 was deemed statistically significant; no adjustment was made to the p-value due to multiple testing. SAS v9.4 (Cary, NC) was used in all analyses.
NYPQ's Institutional Review Board approved this study.
Results
There were 165 total participants: 29 attending physicians, 26 residents, 17 fellows, 18 PAs, and 75 nurses. All 165 (100%) completed the pre-intervention test and 154 (93.3%) completed the post-intervention test. Table 1 shows baseline demographics of participants. There were statistically significant differences in age-range, gender, ethnicity, and years of experience across disciplines. Nurses and attending physicians had the most years of experience, followed by PAs, and then fellows and residents. Subjects were ethnically diverse.
We compared disciplines and examined the change between pre- and post-intervention scores (Fig. 1). The overall pre-intervention score was 43.8%, and the overall post-intervention score was 75.6%. Attendings and fellows had the highest pre-intervention scores and nurses and PAs the lowest. There were no significant changes in the pre- and post-intervention scores when comparing attending and fellow groups. However, there were statistically significant differences between the attending group and other groups (p < 0.01).
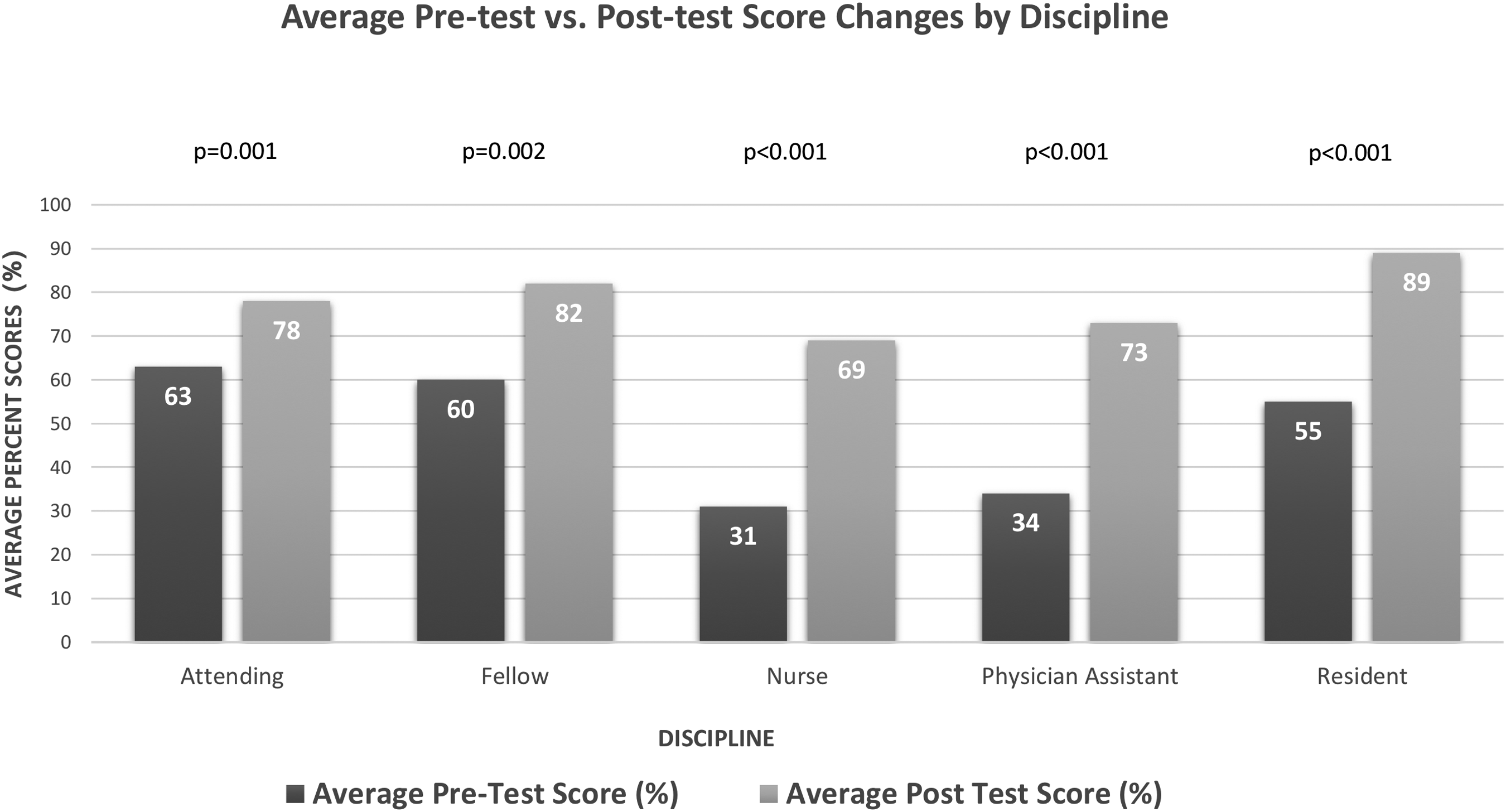
Comparison of pre-intervention and post-intervention test scores by discipline.
Table 3 illustrates score differences for each question by discipline. Questions 1 and 2 focused on factual data and scored higher. Questions 3 to 5 focused on communication and approach and scored lower. Interestingly, question 3, regarding the most appropriate phrasing, appeared to be the most challenging for all groups, with the lowest pre-intervention percent correct.
Pre-Intervention → Post-Intervention Test Score Change for Each Question by Discipline
All groups had a statistically significant increase in their post-intervention scores (all p-values <0.005). Residents had the highest post-intervention scores. Attending physicians had the highest pre-intervention scores and the least improvement compared with the other four groups (p < 0.02). By using a linear model with time, group, and the group/time interaction (allowing for different improvements within each group), we were able to estimate directly the average improvement of each group, as well as compare groups. It revealed that attending scores improved less than residents, nurses, and PAs (p = 0.02, p = 0.001, p = 0.01, respectively), but not less than fellows (p = 0.44). Improvement was not found to differ across other groups.
A total of 154 participants completed at least one question in the postsession evaluation form. Most participants (97%) reported that they learned new information and 91% stated they would change their patient management. Participants completed qualitative comments about how this session would change their patient management approach and their insights on CSDs (Table 4).
Selected Participants' Comments and Insights on Patient Care
Discussion
The combination of presenting evidence-based resources, teaching communication approaches, and role-playing was useful in training on how to have effective CSDs. Knowledge gaps existed for all participants. When given validated tools and communication training, knowledge improved objectively when comparing changes in scores. Subjects reported increased comfort level with CSDs as evidenced by qualitative comments. Study results support that all clinical disciplines can learn skills to conduct CSDs.
Attending physicians had the highest baseline knowledge. Nurses and PAs scored the lowest and had the highest score improvement reflecting receptivity to learn about CSDs. Resident and fellow groups achieved the highest post-intervention scores. This may be related to physician trainees being in the active learning phase and honing their test taking skills.
Score increase was seen in all questions. The greatest improvement was seen in question 3. This suggests that clinicians may feel uncomfortable with making medical recommendations regarding resuscitation. Qualitatively, participants reported new insights that related to “It is acceptable to give recommendations to families.”
Our study had several limitations. It was conducted at one institution and may not be generalizable. Teaching time was limited—reflecting the reality of teaching within clinical constraints in a busy community hospital. Test results could not be analyzed for each participant, so group averages were compared.
Conclusion
This study contributes to the literature by examining multidisciplinary CSD skill-building, allowing for cross-group comparisons, among a diverse clinical staff. This brief educational intervention with multipronged teaching tools improved knowledge and comfort level concerning CSDs. Participants found the education valuable and felt it would change the way they cared for patients. Future studies could explore more focused skill-building on communication and tailoring the intervention to specific disciplines, given differential benefits across groups.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.