
Abstract
Abstract
Background:
Primary care physicians recognize the importance of advance care planning (ACP) conversations and report lack of training and time in the office to start them. Previous efforts have shown that ACP is a low-risk high-value intervention for older patients and those with life-limiting illness.
Objective:
To measure the impact of physician coaching and staff training with registered nurse (RN) support and electronic medical record (EMR) enhancements on the initiation of 2000 ACP conversations in primary care.
Methods:
Employing VitalTalk® physician coaching, Respecting Choices® “Last Steps” ACP facilitator training, support provided by an ACP nurse liaison and EMR customization, the intervention was introduced into 36 primary care practices with an additional EMR tool adopted by 12 of the 36.
Results:
There was an increase from zero at baseline in the number of ACP conversations and a leveling out of new ACP initiated each month. A total of 7200 ACP conversations were initiated for 31 months in 36 primary care practices, and 29% of conversations had advance directives scanned into the EMR during a 10-month review period. Most ACP conversations were initiated by RN care managers. In 2017, there were 7589 more ACP conversations initiated.
Discussion/Conclusion:
By combining two complementary, evidenced-based curricula, providing support of a nurse liaison and designing a summary and alert in the EMR, this program exceeded its goal to initiate 2000 ACP conversations in primary care. Other health systems might consider a similar multicomponent intervention to increase ACP.
Introduction
A
There are few documented models of successful initiation of ACP in primary care although primary care physicians (PCPs) recognize the importance of ACP conversations and their role in having them. 4 PCPs report barriers to having these conversations, including inadequate training, not knowing what to say, inadequate time, and patient–family member conflict. 5 For ACP to succeed in outpatient settings, better clinician communication skills are necessary. 6
Our initiative, Conversations of a Lifetime® (COL), combines multiple modalities, including staff training, physician coaching, and electronic medical record (EMR) enhancements to initiate ACP in primary care. To our knowledge, it is the first system-wide community outpatient model of initiating ACP in primary care. We hypothesized that COL would increase the number of ACP conversations initiated and increase the number of completed advance directives (ADs) scanned into the EMR.
Methods Design
COL was implemented in 36 primary care practices, in an integrated health care system in a large metropolitan Midwestern city. All 36 of the practices in the health system have the Patient-Centered Medical Home (PCMH) designation, a team-based health care delivery model to ensure patients receive the necessary care when and where they needed it. 7 Nineteen of the 36 were also involved in the Comprehensive Primary Care Initiative (CPCi), a Centers for Medicare and Medicaid Services demonstration project. 8 One important resource in CPCi is a full-time RN care manager who initiated ACP conversations. COL was offered between May 2014 and December 2016. This report describes the period from January 2015 to December 2016. The project was supported through a three-year community grant.
Phase 1 (January 2015–December 2016): The intervention included four components: communication coaching for physicians and mid-level providers, training nonphysician ACP facilitators, ACP nurse liaison for support, and EMR enhancements. A four-hour custom coaching curriculum was designed in collaboration with VitalTalk®, 9 a nationally recognized provider of advanced communication skills training for physicians. The Respecting Choices® Last Steps program 10 was used to teach ACP facilitation to key staff to support the PCPs' efforts. Of 169 TriHealth primary care providers in 36 practices, 123 attended the required VitalTalk coaching (73%), and 81 staff members were trained as ACP Facilitators. An ACP nurse liaison provided individualized assistance in the practices through office visits, “lunch and learn” sessions, phone, and e-mail consultation to identify how ACP could be incorporated into practice workflows and maximize EMR documentation. EMR enhancements were designed and implemented at the patient level for both ambulatory and inpatient modules to organize key documents and notes in an ACP summary report; and a simple checkbox was added to provide a data source to track the number of conversations initiated and documented system-wide (Fig. 1). In Phase 1, the 19 CPCi practices served as the intervention group, whereas the other 17 PCMH practices served as the comparison group.

Screenshot from customized feature in EMR of ACP summary report, which follows the patient in ambulatory and inpatient locations within the health system. Features include patient document section with a process for scanning advance directives into the ACP summary rather than the media tab for easier retrieval. “End-of-life discussion” check box is a discrete data field to track the number of ACP conversations initiated. ACP notes can be filtered for ease in locating ACP note from any encounter. ACP, advance care planning; BPA, best practice alert; DNR, do not resuscitate; EMR, electronic medical record.
Phase 2 (March–December 2016): It included all components from Phase 1 and a best practice alert (BPA) in the EMR. The BPA was designed to help providers identify patients most appropriate for initiating ACP. Clinical criteria were adapted from a demonstration project at Gundersen Lutheran and included cognitively intact patients aged 65 years and older (Table 1; Fig. 2). A subset of 12 of the 36 practices agreed to use the BPA.

EMR screenshot of the best practice alert message that providers see when a patient meets criteria for having an ACP conversation. BPA is turned off when the phrase “end-of-life care planning discussion initiated” is marked either yes or no.
ACP, advance care planning; BPA, best practice alert; CMS, Centers for Medicare and Medicaid Services; ED, emergency department.
Phase 3 (January–December 2017): After the intervention period, ACP conversations continued to be initiated and tracked.
Measurement
The main outcomes were the number of patients who had provider-initiated outpatient ACP conversations documented, and a percentage of that population who had AD documents scanned into the EMR. These outcomes were measured as given hereunder:
Phase 1 (36 practices): the number of ACP conversations initiated and documented by the checkbox “yes” in the ACP summary in intervention and comparison practices for 31 months. Phase 2 (12/36 practices using the BPA): measures from Phase 1 and the percentage of records with one or more ADs scanned. Documents included living will, health care proxy, and/or an Ohio DNR form. Phase 3 (38 practices): number of ACP conversations documented by checkbox “yes.”
Results
In Phase 1, 7200 unique patients had ACP conversations initiated and documented in the EMR, including 5392 conversations in the intervention practices and 1808 conversations in the comparison practices. Figure 3 shows trends in the intervention and comparison practices with a leveling off of new ACP as the pool of eligible patients decreased.
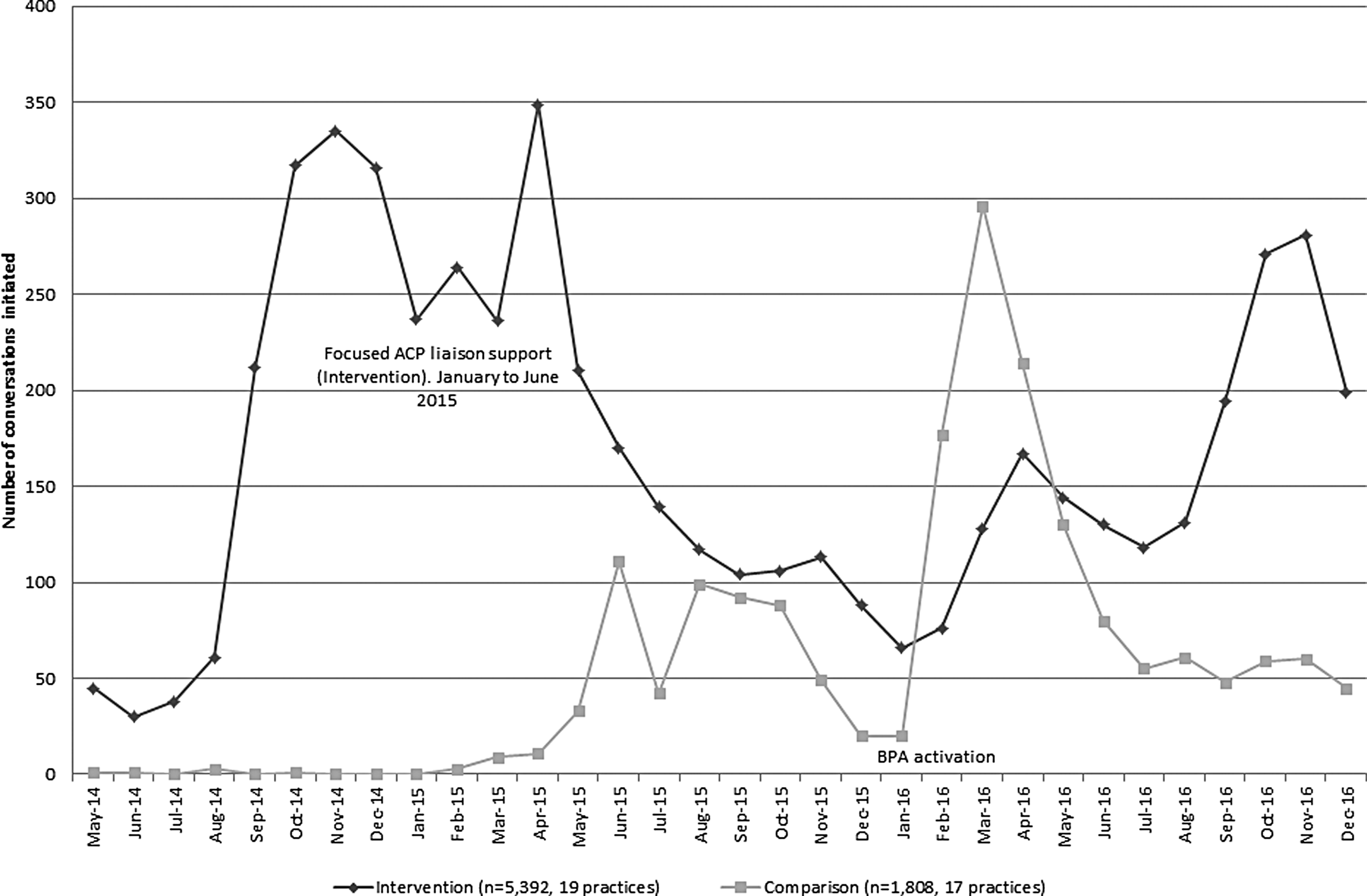
Number of end-of-life (advance care) planning conversations initiated and documented in the EMR in 36 primary care practices for 31 months.
In Phase 2, five intervention practices and seven comparison practices voluntarily implemented the BPA. When ACP was initiated, an average of 29% of conversations led to an AD in the chart. Rates of AD completion were similar in the intervention and comparison practices. There was a wide variation in the number of conversations that led to an AD, from a low of 6% to a high of 70% for a 10-month period. The number of providers per practice and patient populations varied widely.
In Phase 3, in 2017, after the study period, 7589 new ACP conversations were initiated and 123 (1.6%) were billed with the new ACP CPT codes.
Discussion/Conclusion
The COL intervention found that ACP conversations occurred with a combination of communication coaching, staff training, ACP nurse liaison, and EMR changes. ACP conversations initiated in the primary care setting led to ADs being scanned into the EMR. Results point to the need for a practice champion (RN care manager) embedded at a practice site who supports ACP for successful implementation and sustainability. Coaching providers and training key staff is a good start. Ongoing practice support is also helpful. We saw an increase from zero ACP conversations initiated in both intervention (CPCi) and comparison (PCMH) practices, although the BPA led to a spike in ACP documentation in both groups. In the intervention practices, the increase was consistent and sustained. We were encouraged by the consistent number of conversations initiated and documented. Using the BPA helped prompt physicians and staff to initiate ACP conversations. In 2017, we saw the efforts sustained with 7589 more ACP conversations in 38 practice sites. The low number of conversations billed using the ACP CPT codes suggest that reimbursement is not a major factor in having outpatient ACP conversations.
There are limitations to our findings. This was not a randomized trial and there was no measurement for ACP in primary care before the COL intervention was designed and implemented. We did not collect demographic or illness data about patient populations, which might have let us know how many patients should have had conversations. We do not know how the CPCi model impacted the intervention. Only 12 of the 36 practices opted to use the BPA to alert them to patients who would benefit from ACP—becoming a self-selected group who were more likely to implement ACP changes. However, the COL project shows the feasibility of a real-world multicomponent intervention that impacts the occurrence of ACP. Future research could focus on how similar multifaceted interventions impact patient outcomes, including the concordance of EOL care with wishes documented in the outpatient setting and cost of care in the last six months of life.
Footnotes
Acknowledgments
We thank Colleen Kuderer, MSN, RN-BC, ACP Nurse Liaison, who tirelessly and with grace and humor provided technical support and content expertise to the primary care practices. Bethesda Inc., the program funder, provided funds and encouragement to create the innovative Conversations of a Lifetime® program.
Author Disclosure Statement
Jillian Gustin, MD, FACP, FAAHPM, and Julie Childers, MD, FAAHPM, are trained as VitalTalk® facilitators and are paid for their time and travel.