
Abstract
Abstract
Background:
Little is known about research priorities in adult palliative care. Identifying research priorities for adult palliative care will help in increasing research quality and translation.
Objective:
The aim was to identify the views of health professionals' research priorities in adult palliative care that lead to development of a palliative care research agenda in Australia.
Design:
A modified three-round Delphi survey.
Setting/Subjects:
Palliative care researchers and clinicians in Australia were invited to participate.
Results:
A total of 25 panelists completed round 1, 14 completed round 2, and 13 completed round 3. Round 1 resulted in 90 research priorities in 13 categories. Round 2 showed consensus agreement on 19/90 research priorities. Round 3 resulted in the top 10 research priorities of the 19 achieving consensus in round 2. Panelists agreed that research is needed on the transition to palliative care; improving communication about prognosis; increasing access to palliative care for indigenous communities, people who wish to remain at home, and people in aged care; addressing family caregivers' needs; promoting patients' and families' decision making; improving cross-cultural aspects of palliative care; determining the effects of assisted dying legislation; and improving bereavement care in rural, remote, and Aboriginal populations.
Conclusions:
The expert panelists identified the top 10 research priorities for adult palliative care. These identified research priorities are the most urgent topics requiring attention to increase the quality of life of patients requiring palliative care and their family members.
Background
T
The identification of research priorities in adult palliative care is desirable to increase research capacity, quality, and evidence; promote translation of knowledge into practice; prevent research duplication; and enhance funding competitiveness. 6 Globally, these identified research priorities could be used to build research capacity, leverage funding, better identify patient needs, maximize patient recruitment and retention, enable international comparative studies, maximize research translation, and overall contribute to more effective service development to meet emerging needs.9–11 However, there is little known about research priorities in adult palliative care.
Research priorities have been determined for pediatric palliative care in Canada 12 and the United States, 13 but these are unlikely to generalize to adult palliative care because of three differences between the two settings—pediatric palliative care addresses a broader spectrum of diseases, whereas cancer dominates adult palliative care services; children tend to receive palliative care earlier in the disease trajectory than do adults; and there are far fewer children requiring palliative care compared with adults. 14 Two other studies determined research priorities for palliative care and combined adult and pediatric services across Africa 10 and in the Australian state of Victoria. 11 Thus, we aimed to gain consensus on the research priorities of palliative care clinicians and researchers with a view to establishing a prioritized research agenda for adult palliative care in Australia.
Methods
The study was approved by the Curtin University Human Research Ethics Committee (HRE2017-0432). A modified three-round Delphi survey, adapted from Delphi studies of research priorities in pediatric palliative care,12,13 was employed to identify palliative care researchers' and clinicians' research priorities to establish a consensus-based research agenda for Australian adult palliative care. The Delphi technique is an appropriate method to identify research priorities and enables efficient access to a broad range of experts with the aim of achieving consensus through a process where successive stages depend on results from the previous round. 16
Panel recruitment
Panelists were identified as current experts in palliative care research and/or practice in Australia. The research team identified potential panelists (N = 146), purposively selected as experts to optimize data validity, 17 from websites of national and state palliative care associations, university profiles, and lists of presenters at recent palliative care conferences. Several palliative care organizations also advertised the study to members. There is no consensus on the optimal sample sizes for Delphi studies, with sample sizes ranging from 10 to 1000+16,18 and response rates varying substantially from 15.8% 19 to 97.1%. 20 To ensure a minimum sample size of 10 in round 3, accounting for 50% retention rates between consecutive rounds, 21 we aimed to contact at least 80 panelists in round 1.
Questionnaire administration
Potential panelists were invited with an individual link to the round 1 questionnaire, and only those panelists who completed each round received invitations for subsequent rounds (Fig. 1). The questionnaires were hosted online on Qualtrics. After providing informed consent, round 1 panelists were asked a series of demographic questions and to provide their top five priority areas for adult palliative care research in Australia. These responses were collated for use in round 2. Round 2 panelists were asked to rate each of the 90 items on a four-point scale: (1) very important/urgent priority; (2) moderately important/intermediate priority; (3) somewhat important/low priority; or (4) not important/not a priority. There were two open-ended questions to allow panelists to provide feedback (regarding the scope of the questions) and identify any missing priorities. In accordance with a similar study, consensus was defined as being achieved if the percentage of items scoring 1 (urgent priority) or 2 (intermediate priority) was >85% with a mean score <2. 13 Round 3 panelists were asked to rank their top 10 research priorities from those achieving consensus in round 2. Round 3 rankings were collated into a total prioritization score for each item. Panelists had three weeks to complete rounds 1 and 2 and two weeks to complete round 3 and received a reminder e-mail one and two weeks after distribution of each round. Each questionnaire could be completed in one or more sittings to allow panelists to deliberate on responses. 16 Panelists who participated in all three rounds were offered the chance to enter a draw to win one of four $25 gift vouchers.
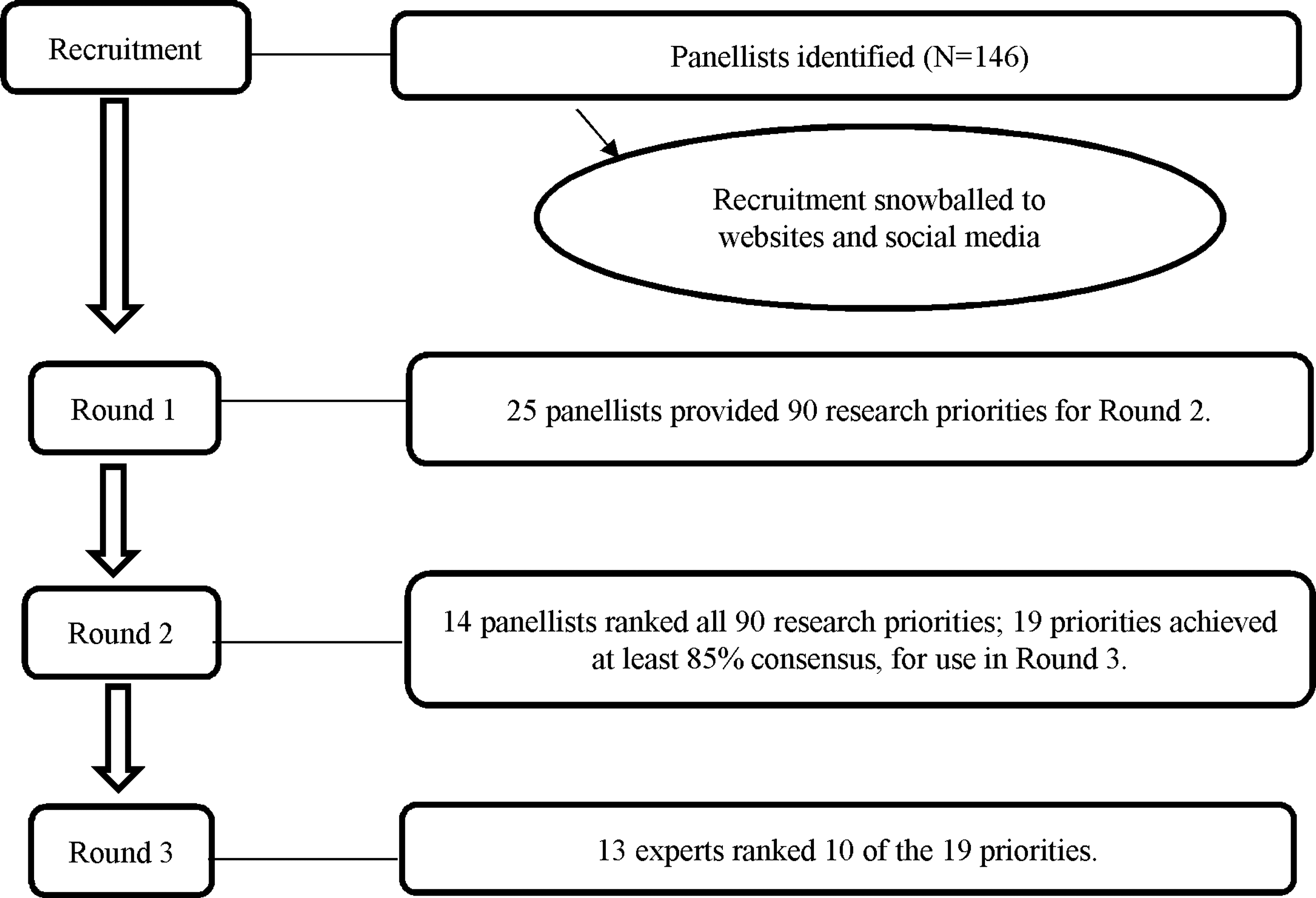
Flowchart of the modified three-round Delphi survey.
Statistical analyses
Statistical analyses were conducted using IBM SPSS, Version 22.0. Less than 1% of the data was missing; a Little's missing completely at random (MCAR) test showed that data were missing at random (df = 0.293, p = 0.864) and therefore were replaced using expectation maximization. Means and standard deviations were calculated for each item. Due to the small sample size and unevenly distributed sample, Mann-Whitney U tests were used to explore differences in panelists' round 2 ratings according to gender; role (researcher or clinician); location (metropolitan or rural); or discipline (medical and nursing or allied health); and median split for experience (>/<) 17 years working in palliative care and >/< 19.5 years since graduation. Effect sizes were interpreted according to Cohen's 22 conventions. Due to the exploratory nature of the study and small sample size, Bonferroni corrections for multiple comparisons were not made.
Results
Item generation, rating, and ranking
Panelist characteristics are summarized in Table 1. The round 1 survey was completed by 25 panelists who generated 125 priorities. These were analyzed by two authors (R.S. and L.J.B.) using conventional content analysis 23 to systematically code, count, and categorize responses; remove ambiguous or duplicate statements; and achieve consensus by discussing discrepancies in opinion. This process resulted in 90 research priority statement items grouped into 13 categories. The means and standard deviations for each category and item are shown in Table 2.
Summary of Panelist Characteristics
SD, standard deviation.
Means and Standard Deviations for Each Category and Item (Round 2)
Items achieving consensus as very important/urgent priority.
Italicized text indicates the means and standard deviations for each category.
A total of 14 of the 25 round 1 panelists completed round 2 (response rate = 56%). Of the 90 items generated in round 1, 19 reached consensus in round 2. A total of 13 of the 14 round 2 panelists completed round 3 (response rate = 93%) and 19 of the 90 items (21.11%) achieved consensus as high priorities. The category with the lowest mean rating (i.e., the highest rating of importance/urgency) was communication between health care professionals and patients/families, followed by community education and capacity building for end-of-life care, and then bereavement care. Two categories had a mean overall priority rating of 2 with all items rated 2 or more—staff training and development, and symptom management—and were therefore considered to be of the least importance/urgency. The 19 items were presented to panelists in round 3 to rank their top 10 (Table 3).
Prioritized Research Agenda for Palliative Care in Australia
Rating comparisons according to panelist characteristics
Mann-Whitney U tests indicated no significant differences in responses according to gender, role, and organization location or discipline, years working in palliative care, and years since graduation. Items in the category of integration of palliative care were rated significantly lower (higher priority) by panelists working in multidisciplinary teams (mean rank 5.44, n = 9) than those not in a multidisciplinary team (mean rank 11.2, n = 5) (U = 4.00, p = 0.013, two-tailed), with a large (r = 0.67) effect size. Items in the category of communication between health care professionals and patients/families were rated significantly higher (lower priority) by panelists working on sites with inpatients (mean rank 10.9, n = 5) than those working on other sites (mean rank 5.61, n = 9) (U = 5.50, p = 0.021, two-tailed), with a large (r = 0.62) effect size. Items in the category of family and caregiver well-being were rated significantly higher (lower priority) by panelists working on sites with inpatients (mean rank 10.7, n = 5) than those working on other sites (mean rank 5.72, n = 9) (U = 6.5, p = 0.032, two-tailed), with a large (r = 0.57) effect size.
Open-ended responses
Five panelists responded to the open-ended questions in round 2. Two panelists commented that the questionnaire represented an exhaustive list of all relevant research priorities. Three provided additional priorities. One suggestion centered on pediatric palliative care, which was not in the scope of our study, and the remaining two suggestions concerned integrative care packages for people with dementia and research on barriers to care for people with neurological conditions.
Conclusions
This study provides evidence to inform a prioritized research agenda for palliative care in Australia. Panelists identified urgent research priorities concerning integration of palliative care, communication, specific populations, family and caregiver well-being, models of care, and bereavement care, all of which feature in the literature.24–31 Panelists identified two research priorities concerning communication between health care professionals and patients/families. Communication surrounding prognosis can be problematic, and there are recommendations to increase research on the development of tools to understand family decision-making typologies; develop methods for consensus building among multidisciplinary teams, patients, and family members when views differ; and determine optimal approaches to supporting and guiding family members when making decisions. 15 Determining optimal timing and processes for communicating the transitions into palliative care was also identified in our study and was a research priority for Victorian palliative care. 11 As the conditions and needs of palliative care patients change over time, research in systems and communication regarding progression into palliative care may help to make the transition as seamless as possible for patients/caregivers. 15
Panelists identified one research priority centered on family and caregiver well-being as well as three other priorities that involved caregivers/other family members. Family caregivers are pivotal for successful patient outcomes and improving quality of life, but often face unmet needs and a lack of support despite the philosophy of family-centered palliative care. 32 These unmet needs stem from numerous factors such as financial disadvantage, social isolation, inadequate symptom management, lack of information regarding their role, discomfort with confronting death and dying, and exclusion from information and care planning. Considering that rates of depression and anxiety are as high as 44% for family caregivers, and that nearly 50% of caregivers are below population norms on physical health, 32 there is a significant need for research to find ways to identify caregivers who would most benefit from palliative care and/or other services and to match the most useful components of palliative care to those with specific needs. 33
Panelists identified two research priorities concerning models of care with an emphasis on palliative care in the home and in aged care settings. Most patients wishing to remain at home and requiring palliative care services are not likely to have their needs and preferences met without significant family caregiver input 32 and therefore research could help to identify ways to support family members/caregivers. Our study suggests that Australian services, caregivers, and families may benefit from research that promotes preparedness for the transition to palliative care.
Panelists identified three research priorities concerning indigenous and culturally diverse populations. Disparities in quality of life for Aboriginal and Torres Strait Islander and culturally and linguistically diverse (CALD) people diagnosed with chronic illness, groups in comparison with Anglo-Australian populations, are well recognized. Cancer is the second leading cause of death in Aboriginal and Torres Strait Islander people and is more likely to be diagnosed as terminal in indigenous populations than Anglo-Australian populations, 34 and clinical levels of depression in cancer survivors are significantly higher for ethnic minority groups in Australia (11% Arabic, 9% Chinese, and 9% Greek) compared with Anglo-Australians (2%). 35 Aboriginal and Torres Strait Islanders remain under-represented in the palliative care population due to a lack of understanding of palliative care, poor availability of services, and the burden of chronic disease outranking palliative care as a priority. 36 Barriers and challenges to access include language barriers, unfamiliarity with health care systems, socioeconomic status and lack of financial resources, discrimination and cultural incompetence of health professionals, structural barriers within the health system, and lack of access to CALD or Aboriginal and Torres Strait Islander health care providers.35,36 A study in Canada identified key challenges for palliative care specific to rural indigenous populations to increase the relevance, access, and comprehensiveness of palliative services specific to their needs. 37
Panelists identified two research priorities concerning bereavement. Bereavement care is an increasing area of interest and sophistication in palliative care. 38 However, the provision of tailored support is hampered by questions concerning who to support, for how long, and to what end, given funding and staffing constraints. 39 Research addressing these issues would be complemented by research to strengthen the community's capacity to support the dying and the bereaved. 40
Study limitations
The panelists were very experienced palliative care clinicians and researchers (averaging over 20 years working in palliative care) and there was a high retention rate from round 2 to 3. 20 However, the sample was small and nonrandom, and participation rates were lower than similar studies using the same methods of identifying and inviting panelists. 41 There was a small representation by panelists from medicine/nursing disciplines (and rural locations), which means that the identified priorities might not reflect the goals of the two main disciplines in palliative care. The identified research priorities may not be definitive or in fact constitute current research gaps as they may have been investigated, but not successfully disseminated. Further Delphi or other studies would be useful to provide a more comprehensive picture of expert opinion both in Australia and in other countries. Although we sought to develop a holistic picture of health professionals' perspectives for urgent research in adult palliative care, the perspectives of patients and their family caregivers were not represented. Investigating these stakeholders' perceptions in palliative care research will help identify goals for progress so that interventions can target and be tailored to specific needs of the patient and family members.15,42
Clinical implications
This study is the first to systematically generate research priorities for adult palliative care in Australia based on researchers' and clinicians' perspectives of urgency, gaps in knowledge, and potential for impact on the quality of life of palliative care patients and their families. The study offers guidance for adult palliative care research (nationally and internationally) that could be conducted to address the priorities identified for adult palliative care in Australia, particularly in the areas of communication, integration of palliative care services, caregiver and family needs, new models and packages of palliative care, indigenous and cross-cultural populations, and bereavement care. These priorities provide an evidence base to guide palliative care research that is oriented toward the needs of researchers and clinicians so that research is strategic, clinically relevant, and addresses neglected areas.
Footnotes
Acknowledgment
This study received no funding. The authors thank the palliative care experts for their interest in this research.
Author Disclosure Statement
No competing financial interests exist.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.