
Abstract
Abstract
Introduction:
With medical cannabis (MC) remaining illegal at the federal level, hospice programs are unsure how to handle requests for MC, particularly since hospice is largely funded with federal dollars. The purpose of this survey was to determine respondents' comfort level with MC use in hospice, what processes and logistics hospice programs are employing when dealing with MC, and to determine what, if any, education hospice programs are providing to their staff.
Methods:
An anonymous online survey assessed a variety of factors surrounding hospice staff practice, experience, and opinions regarding MC. The survey was disseminated to employees of clients of a large hospice benefit manager as well as through a national hospice and palliative medicine professional organization.
Results:
Three hundred ten hospice professionals responded to the survey. More than half of the respondents were nurses followed by administrators and physicians. Regardless of legal status, hospice staff members were overwhelmingly in agreement that MC is appropriate for hospice patients to have access to and use. Several barriers to use were identified including discordant legal status between state and federal governments, concerns about clinical efficacy and safety, and a myriad of other societal factors. Wide variations in MC documentation and education practices between hospices were noted.
Discussion:
The data suggest overwhelming support for MC use in the hospice setting. Our findings highlight important opportunities to support hospice providers and their patients through education and the development of policies around MC.
Introduction
Evidence on the effectiveness of medical cannabis (MC) for symptoms experienced at the end of life such as pain, muscle spasms, anorexia, nausea/vomiting, and cachexia dates back thousands of years.1,2 At the time that this survey was conducted, plant-based cannabis was legal for medical use in 33 of 50 U.S. states and DC. 3 Despite widespread interest in the use of plant-based cannabis in hospice, it presents a number of problems, particularly since it is illegal at the federal level and hospice is largely funded with federal dollars. 4 This survey sampled hospice staff from programs across the United States to assess their comfort level with MC use in hospice, and to describe the processes and logistics they are employing when dealing with MC. In addition, respondents were asked to describe education provided and the existing protocols for cannabis use in their organization.
Methods
We developed a 37-item online survey in consultation with a team of experts in palliative care pharmacy and education. Survey questions encompassed four domains: (1) respondent characteristics; (2) practice, experiences, and opinions regarding MC; (3) concerns related to MC use; and (4) hospice processes and education. The research team tested the survey for errors and made revisions through a collaborative process. The instrument consisted of a series of multiple-choice questions with opportunities for free text commentary. The survey was created and disseminated using an online survey tool (Formsite; Vroman Systems, Inc., Downers Grove, IL).
Enclara Pharmacia, a national full-service pharmacy benefit manager and mail order supplier of medications and clinical services for the hospice industry, sent an e-mail invitation to participate in the survey to >500 hospice clients. A link to the survey was also included in two National Hospice and Palliative Care Organization (NHPCO) NewsBriefs newsletters and posted in the “Research Opportunities” section on NHPCO.org. Participants who responded to the survey were granted access to a free “Medical Cannabis in Hospice and Palliative Care” online course. The survey was open for two and a half weeks. Notice of informed consent was provided at survey introduction and all responses were anonymous. The Institutional Review Board of the University of Maryland, Baltimore, approved the survey.
Data Analysis
Responses were downloaded into an electronic spreadsheet for central record keeping and descriptive analysis. The terms “cannabis” and “marijuana” are often used interchangeably and as such were both used within survey questions for familiarity purposes. However, for consistency we designated the term “cannabis” for use in the Results and Discussions sections.
Results
The sample included a national representation of 310 hospice professionals (primarily nurses) from 40 states. Organizational characteristics such as size by average daily census (ADC) and profit status were compared with national statistics reported by NHPCO. The organizational size based upon ADC of respondents was similar to national trends; however, our sample had a higher representation of not-for-profit hospices. Table 1 and Appendix Table A1 list the characteristics of the respondents, their hospices, and the legal status of cannabis in their practice state. The majority of respondents (62%) reported that they practiced in states where MC is legal for medical or recreational use, whereas 33% came from states where it was not legal, and a small percentage (5%) were unsure of the legal status of cannabis in their state.
Respondent Characteristics
According to respondents, there is overwhelming support (91%) for MC use for hospice patients. However, respondents reported that is rare for hospice physicians to recommend or certify patients for MC. Half of the physician respondents (n = 18) indicated that they do not write orders to certify patients for MC, whereas seven report doing so less than once a month, and one certifies patients more than six times per month. In addition, most respondents indicated that hospice physicians discuss MC with patients only if specifically asked. They overwhelmingly agreed (84%) that health care professionals would benefit from standardized protocols to better manage MC in their organizations.
It is common for patients or family members to inquire about MC, with 90% responding that they have fielded questions from patients and slightly over half receive inquiries about its use one to two times per month. However, it is unusual for clinicians to initiate discussion of using MC with patients, families, or physicians involved in the case, with only 37% reporting having done so in the past month. Even in states where cannabis is legal, less than a third of nurses provide education on its use.
Table 2 summarizes respondents' attitudes toward MC use and their opinions of how patients, family members, and staff/coworkers view its use in hospice. Although most clinicians are not concerned about patients' MC use, their opinions about others' attitudes toward its use are mixed.
Fear of Medical Cannabis
Most respondents have cared for a patient using MC; only 27% have not. For those who have cared for a patient, MC is viewed as effective in treating a variety of symptoms. When asked what symptoms respondents felt MC managed with the greatest success, nausea/vomiting, pain, and anxiety were reported the most. Many (43%) report observing no serious toxicities or adverse effects, followed by confusion (8%), drowsiness (8%), somnolence (5%), and dry mouth (5%).
MC is usually documented within the medication profile or progress note although documentation practices vary widely (Table 3). Approximately half of hospice staff usually alert the pharmacist/medication reviewer when a patient is using MC; however, 25% do not. The chemical composition is frequently not known by clinicians or patients and routes of administration (e.g., smoked and vaporized) and dosage formulations (e.g., oils and edibles) (Fig. 1) vary considerably.
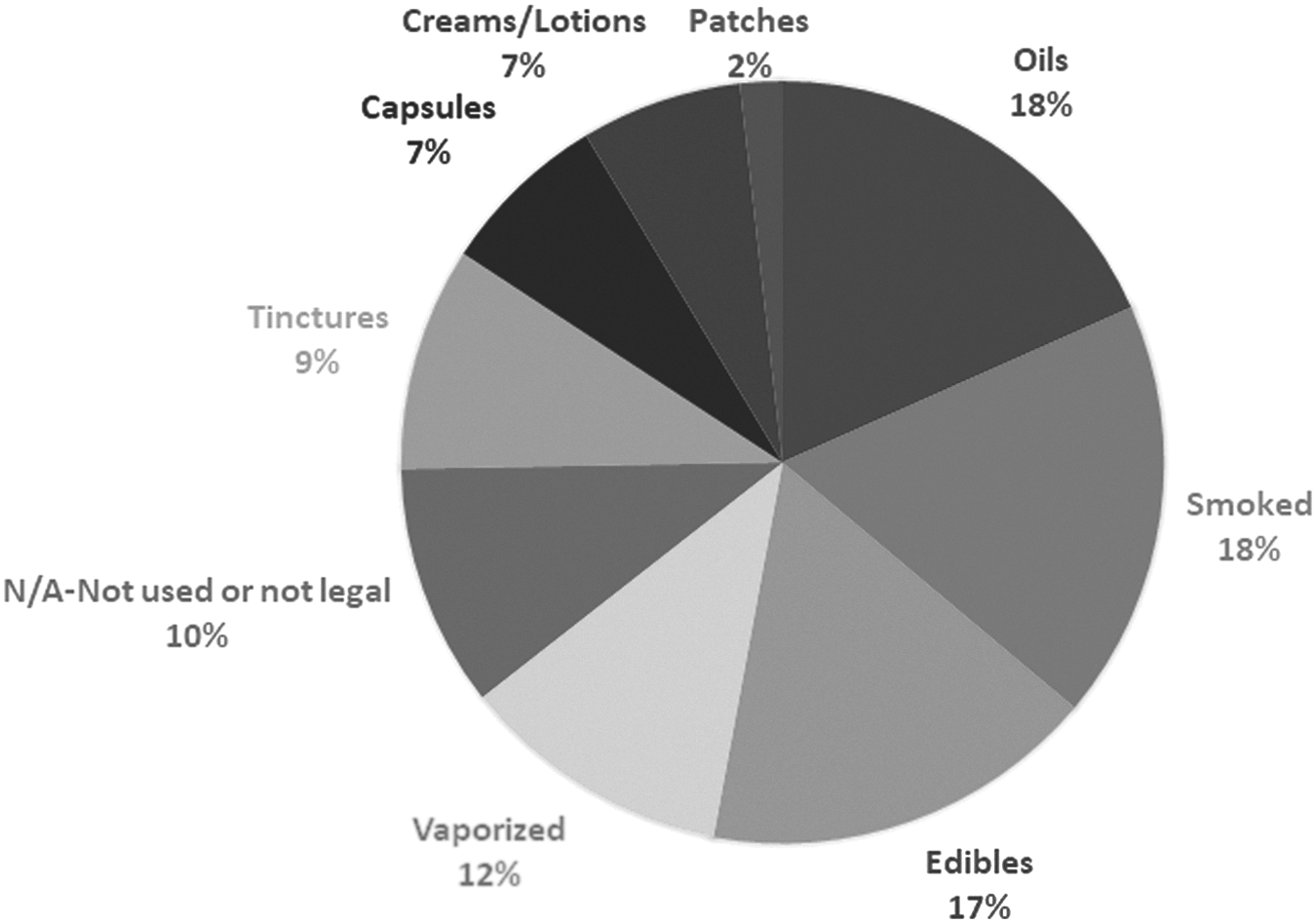
What forms of cannabis are your patients using? (select all that apply) (responses = 894, n = 310).
Hospice Processes
Most hospices lack an MC policy with only 19% of respondents stating that their organization has one. Patients pay for MC out of pocket and hospices do not cover the cost. Except in rare instances, hospice staff members do not assist in the administration, procurement, or disposal of MC.
Figure 2 displays the education provided to staff and volunteers related to MC. Many have not received education, but for those who have, a wide variety of topics are discussed.
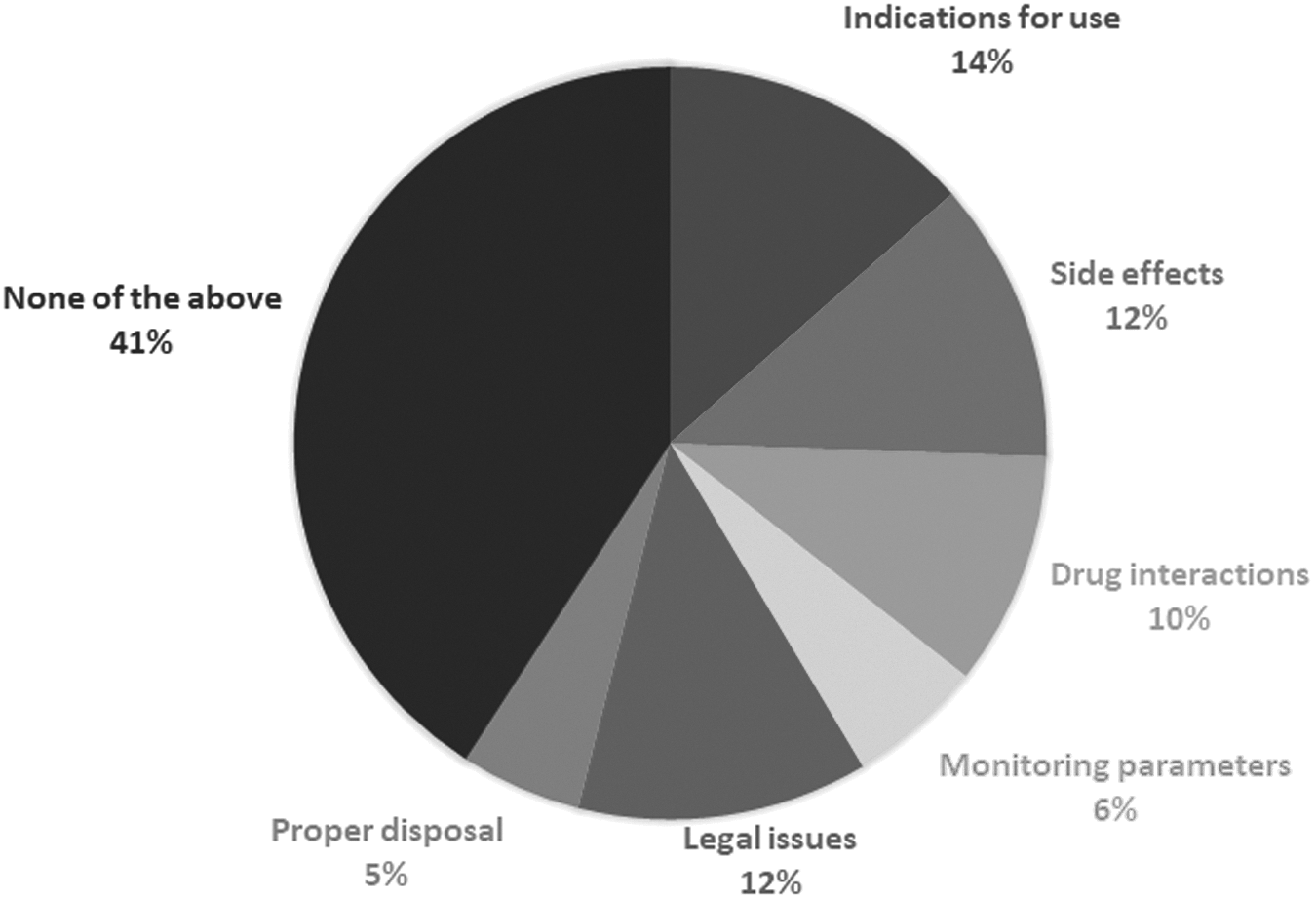
On which of the following does your hospice provide education to staff and volunteers as it relates to medical cannabis? (select all that apply) (responses = 497, n = 310).
Discussion
This is the largest national survey to date to examine the knowledge, experience, and views of hospice professionals regarding the use of MC. 1 Many respondents provided optional responses that gave additional insight about their most relevant concerns that are highlighted hereunder.
First, similar to findings by Uritsky et al., 1 regardless of legal status, hospice staff overwhelmingly support patient access to MC. Those who practice in states where MC is not yet legal wish that it was.
Second, respondents described several barriers to use, including the discordant legal status between state and federal governments, concerns about clinical efficacy and safety, and other societal factors. Despite lack of fear and a high level of acceptance of MC use, areas of misinformation and confusion remain. Many respondents expressed knowledge deficits and regulatory-related concerns, highlighting challenges to overcome before MC is more commonly used in hospice.
Additional barriers include underutilization and lack of access, barriers to procurement, and high out-of-pocket cost. Also, many hospice physicians are not certified to recommend MC for patients and are not discussing its use with patient unless brought up by patients or caregivers. It is important to clarify that physicians only “recommend” or “certify” a patient for cannabis and do not legally “prescribe” it due to its categorization as a DEA Schedule I substance; however, some continue to mislabel the practices “prescribing.” In addition, the relatively new legal status of MC in some states may contribute to a lack of expertise, training, or certification required to recommend it.
Respondents also expressed concern about providing or covering cannabis as a symptom management medication while receiving federal reimbursement. For this reason, hospices do not cover the cost of the therapy, yet express discomfort that they are not paying for a medication that provides symptom relief. They also raised concerns about storing or administering cannabis in an inpatient setting and about the potential for recreational use and diversion or theft by family members.
Third, respondents were uncertain about the specific MC products their patients were using, including the tetrahydrocannabinol (THC)/cannabidiol (CBD) content, dosage form, dosing, and potential for drug interactions. More research in this area is needed, as the hundreds of molecules that compose the whole plant make the matter of interactions more complex than single-entity medications. Clinicians should advise a “start low and go slow” approach coupled with close monitoring for adverse effects, and should familiarize themselves with the information on interactions that is currently available.5,6 In states where cannabis is legal, less than a third of clinicians provide education to patients and family members, which may be due to the lack of MC education.
These findings highlight the need for education, protocols, and standardization, specifically regarding documentation. There was a wide variation in where cannabis was documented in the patient record. These inconsistencies may contribute to a pharmacist or medication reviewer being unaware that a patient is using MC. Finally, hospice staff members are not assisting in the procurement, administration, or disposal of MC. Staff who disposed of cannabis used methods consistent with those used for opioids. There was widespread agreement that hospices would benefit from standardized protocols to better manage MC in their patients, although few report having a formal policy in place. The American Pain Society's Clinical Practice Recommendations for Care of Patients Using Cannabis as Therapy may be useful source when designing future cannabis protocols for hospice. 7
Strengths and Limitations
There are several limitations to this study. Although we solicited responses from all types of hospice providers, we had a lower proportion of physicians compared with nurses, which could be explained by the ratios of physicians to nurses on a typical hospice staff. Given that hospice nurses spend a significant amount of time at the bedside with patients and families where cannabis is used, we feel their responses provide useful insight to answer our research question along with physicians, pharmacists, and other interdisciplinary team members. Many of the respondents expressed differences in use patterns that may result from variation in exposure to or experience with MC, especially because the legal status differs from state to state. However, even in states where it is not legal, patients are still using it, or where it is legal, some patients are obtaining it through illegal means.
Conclusion
MC is an important and frequently misunderstood treatment for many symptoms commonly experienced by hospice patients. The consensus of our survey sample is that MC appears to be relatively safe and effective for a variety of conditions and is being used by several routes of administration. The data suggest overwhelming support for legalizing cannabis on a federal level for medical use. Our findings highlight important opportunities to support hospice providers and their patients through education and the development of policies. Based on the support for its use among hospice staff, its increasing availability and acceptance among the public, and anecdotal reports of its effectiveness in managing symptoms at the end of life, MC could one day be commonly used in hospice. Policies, protocols, education, and additional research to support its safe and appropriate use are needed going forward.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Appendix
Hospice Location by State
| What state do you currently practice in? | ||
|---|---|---|
| Result | Responses | Percentage |
| North Carolina | 45 | 14.50 |
| Pennsylvania | 26 | 8.30 |
| Michigan | 19 | 6.10 |
| Florida | 16 | 5.10 |
| Ohio | 16 | 5.10 |
| Illinois | 14 | 4.50 |
| New Jersey | 12 | 3.80 |
| Texas | 12 | 3.80 |
| California | 11 | 3.50 |
| Colorado | 11 | 3.50 |
| New Mexico | 11 | 3.50 |
| Kentucky | 10 | 3.20 |
| Oregon | 10 | 3.20 |
| Connecticut | 8 | 2.50 |
| Minnesota | 8 | 2.50 |
| Maine | 7 | 2.20 |
| Wisconsin | 7 | 2.20 |
| Indiana | 6 | 1.90 |
| New York | 6 | 1.90 |
| Delaware | 5 | 1.60 |
| Iowa | 5 | 1.60 |
| Arizona | 4 | 1.20 |
| Maryland | 4 | 1.20 |
| Massachusetts | 4 | 1.20 |
| Tennessee | 4 | 1.20 |
| Arkansas | 3 | 0.90 |
| Missouri | 3 | 0.90 |
| New Hampshire | 3 | 0.90 |
| Oklahoma | 3 | 0.90 |
| Vermont | 3 | 0.90 |
| Alabama | 2 | 0.60 |
| Georgia | 2 | 0.60 |
| Rhode Island | 2 | 0.60 |
| South Carolina | 2 | 0.60 |
| Hawaii | 1 | 0.30 |
| Idaho | 1 | 0.30 |
| Mississippi | 1 | 0.30 |
| Montana | 1 | 0.30 |
| North Dakota | 1 | 0.30 |
| Virginia | 1 | 0.30 |
| Alaska | 0 | 0.00 |
| Kansas | 0 | 0.00 |
| Louisiana | 0 | 0.00 |
| Nebraska | 0 | 0.00 |
| Nevada | 0 | 0.00 |
| South Dakota | 0 | 0.00 |
| Utah | 0 | 0.00 |
| Washington | 0 | 0.00 |
| West Virginia | 0 | 0.00 |
| Wyoming | 0 | 0.00 |