
Abstract
Abstract
Objective:
We investigated correspondence between symptom severity and symptom bothersomeness in patients with advanced cancer.
Background:
Symptom severity is commonly assessed in clinical cancer settings, but bothersomeness of these symptoms is less often measured.
Methods:
Participants with advanced cancer enrolled in a cluster-randomized trial of early palliative care completed the Edmonton Symptom Assessment System (ESAS) and the quality of life at the end of life (QUAL-E) measure as part of their baseline assessment. For each symptom, we examined the correspondence between the symptom being indicated as most severe on the ESAS and rated as most bothersome on the QUAL-E.
Results:
For the 386 patients who completed relevant sections of the ESAS and QUAL-E, tiredness (32.8%), sleep (23.8%), and appetite (20.2%) were most frequently rated as most severe, whereas pain (28.9%) and tiredness (24.3%) were most frequently indicated as most bothersome. The most bothersome and most severe symptom corresponded in 42%. Pain and/or tiredness were consistently among the top three most bothersome symptoms, whereas appetite was frequently rated the most severe symptom but was rarely perceived as the most bothersome. The probability that patients rating a symptom as most severe would also rate it as most bothersome was highest for pain (66%), nausea (58%), and tiredness (40%).
Discussion:
ESAS symptom severity does not necessarily indicate patients' most bothersome symptom; regardless of severity, pain and tiredness are most frequently perceived as most bothersome. Further research should investigate the clinical benefits of patients also indicating their three most bothersome ESAS symptoms.
Introduction
Patients with advanced cancer experience numerous physical and psychological symptoms that must be accurately identified and managed to improve quality of life.1,2 Ensuring that patients feel understood by their health care providers is paramount for effective clinical decision making. 3 Evidence has shown that clinicians can obtain substantially more information regarding patients' symptoms through systematic assessment in comparison with open-ended questioning. 4
One of the most well-known and frequently utilized systematic symptom assessment tools is the Edmonton Symptom Assessment System (ESAS). The ESAS is a reliable, valid, widely-used measure that assesses the severity of nine common symptoms on a 0–10 numerical scale.5–7 However, discrepancies have been noted among severity recorded on patient-reported outcome measures, the documentation of severity on medical records, and the symptom-related actions taken by health care providers.8,9 These discrepancies may be related to clinicians taking actions on symptoms based on incomplete information and their own assumptions, but may also relate to the fact that the symptom questionnaires that were used measured only severity and not patients' prioritization of their symptoms.
The quality of life at the end of life (QUAL-E) scale is a 26-item measure of patients' quality of life at the end of life, which includes six domains: sense of life completion, relationship with the health care system, preparation for end of life, symptom impact, social support, and spirituality.10,11 The QUAL-E differs from the ESAS in that its symptom impact domain asks patients to identify their most bothersome symptom. Bothersomeness in relation to a symptom can be defined as the degree to which that symptom causes the patient difficulty 12 or the degree to which the patient perceives that symptom to be important. 13 It can be differentiated from distress, which has been defined as a “multifactorial unpleasant experience” that may interfere with the ability to cope effectively with cancer, its physical symptoms, and its treatment. 14
Symptom bothersomeness is not often measured routinely, and few studies have assessed its relationship to the more often measured construct of symptom severity. In one study, 130 patients with cancer receiving outpatient chemotherapy completed the European Organisation for Research and Treatment of Cancer Core Quality of Life Questionnaire (EORTC QLQ-C30) and reported their most bothersome quality of life issues from categories based on QLQ-C30 domains. 12 Absolute scores were found to identify most bothersome quality of life issues better than change scores. In another study, patients completed the EORTC QLQ-C30, the ESAS, and the hospital anxiety and depression scale, and were asked to name and prioritize up to five symptoms that they considered most troublesome, from a list of 31 symptoms. 13 Symptom prioritization was associated with severity scores of pain, appetite, nausea, dyspnea, constipation, depression, and anxiety, but not fatigue, physical function, role function, or inactivity. Yet another study compared self-assessed symptom severity, measured by a categorical scale (mild, moderate, and severe) with a single question (symptom bothersome/distressful or not), and found that the prevalence of bothersomeness increased with greater symptom severity. 15 However, the assessment tool was a 48-item checklist of symptoms developed by the investigators, which had not been previously validated, and symptom bothersomeness and distress were used synonymously.
The primary purpose of this study was to investigate the level of correspondence between the most severe symptom rated on the ESAS by patients with advanced cancer, and the most bothersome symptom reported on the QUAL-E. The second objective of this study was to examine discordant responses to determine which symptoms are being reported as the most bothersome, despite not being the most severe.
Methods
Participants
Participants were enrolled in a cluster-randomized controlled trial conducted at the Princess Margaret Cancer Centre in Toronto, Canada, between December 1, 2006, and February 28, 2011. 16 This trial examined the impact of early palliative care compared with standard oncology care on quality of life, symptom control, and satisfaction with care. Eligible patients were 18 years or older, English speaking, and had stage IV cancer (hormone refractory for prostate and breast cancer; stage III patients with poor prognosis were included at oncologists' discretion). Other inclusion criteria were an estimated survival of 6–24 months (estimated by the treating oncologist), Eastern Cooperative Oncology Group (ECOG) performance status of 0–2, and a passing score on the short orientation-memory-concentration test. 17 Patients provided written informed consent, and the trial was approved by the University Health Network's Research Ethics Board.
Measures
Demographic and clinical information was abstracted from patients' medical records. In addition, all patients completed self-report measures at baseline and monthly for four months; for this study, only baseline data from the ESAS and the QUAL-E measures were analyzed.
The ESAS is a validated self-report measure of severity of nine common cancer symptoms rated on a scale from 0 (none) to 10 (worst); it is widely used in palliative care settings. 5 This study employed an 11-item version (ESAS-CS) that was revised to include constipation and sleep. 18 Patients rated the severity for each of the following symptoms: pain, tiredness, nausea, depression, anxiety, drowsiness, appetite, feeling of well-being, shortness of breath, constipation, sleep, and an additional self-reported symptom.
The QUAL-E is a 26-item self-report questionnaire that assesses quality of life near the end of life with regard to physical and emotional symptoms, relationships with health care providers, preparation for the end of life, and life completion. 11 This measure has been validated for use with seriously ill patients at the end of life, including those with advanced cancer.19,20 For this study, we examined only results from the subscale on physical and emotional symptoms. Patients were asked to list three physical or emotional symptoms that bothered them in the last week, and to identify the one symptom that bothered them the most.
Statistical analyses
Each QUAL-E response was first matched with and categorized into an appropriate corresponding ESAS symptom (by B.L.), all matches were checked by C.Z., and discrepancies were resolved by discussion. Since patients chose their own most bothersome symptoms, not all written responses matched with those listed on the ESAS. QUAL-E responses that could not be matched with an ESAS symptom were left uncategorized and were not included in the analyses (Appendix Table A1).
We examined the frequency distributions of the most bothersome QUAL-E symptoms and most severe ESAS symptoms, as well as the frequency of correspondence between symptoms with the highest severity rating and symptoms identified as most bothersome. In cases where patients listed more than one symptom as being the most bothersome, each symptom was counted separately in frequency analyses. If there were several symptoms rated with the same highest score on the ESAS, symptoms were considered to correspond if the most bothersome symptom on the QUAL-E matched with any one of those ESAS symptoms.
To further explore the relationship between symptom severity and bothersomeness, we examined frequencies and mean ESAS severity scores for individual symptoms within four different participant groups. These groups indicated a symptom to be most severe and most bothersome, most severe but not most bothersome, most bothersome but not most severe, and neither most severe nor most bothersome. A symptom was considered to be most severe if a participant rated it the highest, relative to the other ESAS symptoms. We also calculated the positive predictive value (PPV) for each symptom for all participants. This was defined as the probability that patients would also rate a symptom as most bothersome if they had already rated it as most severe.
Results
Sample characteristics
Of the 461 participants who were enrolled in the trial and completed baseline assessments, 74 (16.1%) did not indicate their most bothersome symptom on the QUAL-E and were excluded from this study. One patient stated that none of the three self-reported QUAL-E symptoms was the most bothersome and was also excluded from the analyses. Demographic and medical characteristics for the 386 study participants are summarized in Table 1.
Patient Characteristics (N = 386)
Data missing for three patients.
ECOG, Eastern Cooperative Oncology Group; ESAS, Edmonton Symptom Assessment System; SD, standard deviation.
Ten patients reported more than one symptom as most bothersome on the QUAL-E, adding an additional 14 most bothersome symptoms, for a total of 400 QUAL-E entries analyzed for their correspondence. Of the 400 QUAL-E entries, 329 (82.2%) were matched to an ESAS symptom, and 71 (17.8%) could not be matched (Appendix Table A1) but were included in the analysis as noncorrespondent symptoms. The most bothersome QUAL-E symptoms that could not be matched were most commonly diarrhea (3.5%), numbness or tingling in the hands or feet (2.0%), and coughing (1.0%).
Frequency and correspondence of QUAL-E bothersomeness and ESAS severity scores
The frequency distributions of the highest-rated ESAS symptoms and most bothersome QUAL-E symptom are shown in Figure 1. Tiredness (32.8%), sleep (23.8%), and appetite (20.2%) were most often the highest-rated ESAS symptom, whereas nausea (5.2%) was least often rated the highest. On the QUAL-E, pain (28.9%) and tiredness (24.3%) were most often reported as the most bothersome symptom, whereas drowsiness (0.3%) was least often reported.

Number of participants indicating symptoms highest on ESAS, most bothersome on QUAL-E, and simultaneously most severe and most bothersome (N = 400). ESAS, Edmonton Symptom Assessment System; QUAL-E, quality of life at the end of life. Color image is available online.
Overall, the most bothersome QUAL-E symptom corresponded to the highest-rated ESAS symptom in 168 (42.0%) participants. The symptoms that were most often rated simultaneously as most bothersome and most severe were tiredness (n = 52 [13.4%]) and pain (n = 31 [7.7%]) (Fig. 1). The number of participants rating an ESAS symptom as most severe was typically greater than the number of patients stating that the same symptom to be the most bothersome on the QUAL-E. This was most apparent for sleep (n = 92 [22.9%] rated most severe vs. n = 15 [3.7%] rated most bothersome), appetite (n = 78 [19.5%] vs. n = 6 [1.5%]), and drowsiness (n = 51 [12.7%] vs. n = 1 [0.2%]). Only pain and nausea showed the inverse pattern: only 48 (12.4%) patients gave pain the highest severity rating on the ESAS, but 112 (27.9%) patients reported pain to be the most bothersome on the QUAL-E. A total of 20 (5.2%) patients gave nausea the highest ESAS severity rating, whereas 25 (6.5%) patients reported nausea to be the most bothersome.
Most bothersome symptoms reported together with highest-rated ESAS symptoms
The top three most bothersome QUAL-E symptoms reported by those participants who indicated the highest severity rating for each ESAS symptom are shown in Figure 2. Regardless of which ESAS symptom was rated as most severe, tiredness was consistently one of the top three most bothersome symptoms. Furthermore, pain was consistently one of the top three most bothersome symptoms except when nausea was the highest rated ESAS symptom.
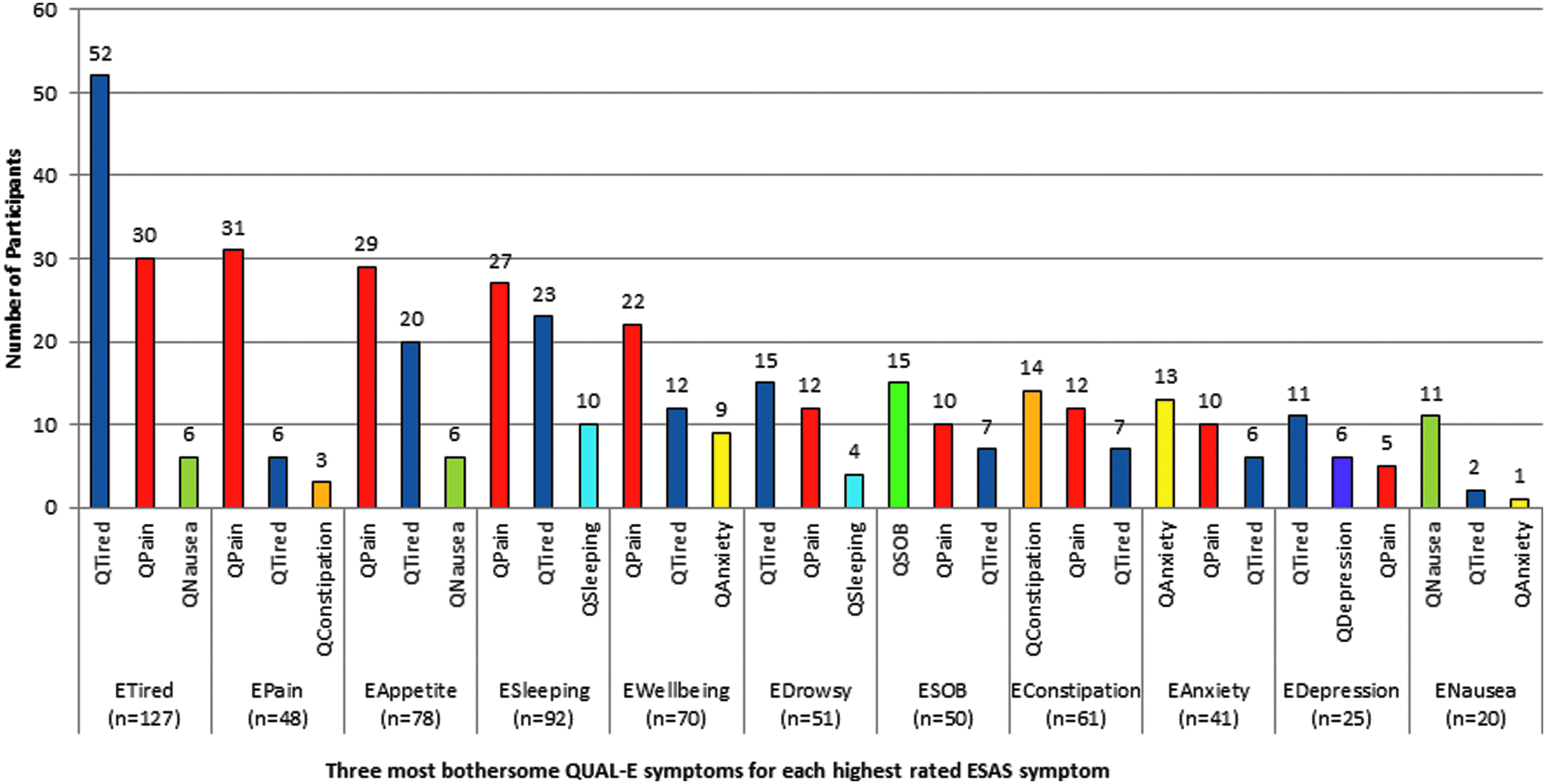
Frequency distribution of the top three most bothersome QUAL-E symptoms reported by participants indicating an ESAS symptom as most severe (N = 400). E[symptom], signifies highest-rated ESAS symptom. Q[symptom], signifies most bothersome QUAL-E symptom. SOB, shortness of breath. Color image is available online.
When tiredness, pain, shortness of breath, constipation, anxiety, and nausea were rated as most severe, they were also found to be the most bothersome symptoms. When the two ESAS symptoms of sleep and depression were rated as most severe, they were among the three symptoms that were most frequently mentioned as most bothersome. However, when the ESAS symptoms of appetite, well-being, and drowsiness were rated as the most severe, they were not among the top three most bothersome symptoms.
Mean ESAS scores for most severe and most bothersome symptoms
Table 2 gives mean ESAS severity scores for participants indicating a given symptom as most severe and most bothersome, most severe but not most bothersome, most bothersome but not most severe, and neither most severe nor most bothersome. Physical symptoms tended to have the highest mean rating if they were most severe and most bothersome. However, ESAS scores for depression and anxiety were highest when they were rated as most severe but not most bothersome. Of note, mean severity scores for depression, anxiety, sleep, appetite, and nausea in the “most bothersome but not most severe” category were in the range of <4/10, indicating that these symptoms can be experienced as bothersome despite being rated as “mild” on the ESAS.
Mean Edmonton Symptom Assessment System Scores for Most Severe and Most Bothersome Symptoms
The most severe symptom is the symptom rated by the patient as most severe on the ESAS, relative to other symptoms; the most bothersome symptom is the symptom rated by the patient as most bothersome on the QUAL-E. The highest mean severity across categories for each symptom (i.e., in each row) is indicated in bold.
CI, confidence interval; PPV, positive predictive value.
Table 2 also shows the PPV for each symptom, indicating the probability that patients rating a symptom to be most severe would also rate it as most bothersome. PPVs were highest for pain (66%), nausea (58%), and tiredness (40%); for the remaining symptoms, PPVs were all <30%.
Discussion
Our study demonstrates that symptom severity does not correspond consistently with symptom bothersomeness. Although the ESAS captured the majority of the most bothersome symptoms reported on the QUAL-E, there was low correspondence between the most severe and most bothersome symptoms. The symptoms most commonly rated as most severe on the ESAS were tiredness, sleep, and appetite, whereas those rated most frequently as most bothersome on the QUAL-E were tiredness and pain. The symptoms most commonly listed as simultaneously most severe and most bothersome were tiredness and pain; these two symptoms appeared consistently in the top three most bothersome symptoms, regardless of which of the 11 symptoms patients rated the highest in severity. The probability that a symptom rated as most severe was also rated as most bothersome was highest for pain, nausea, and tiredness.
Our study directly investigated correspondence between symptom severity and symptom bothersomeness using data obtained from two clinically validated patient-reported symptom assessments. The findings indicate that although symptom severity is an important aspect of symptom experience, it is not synonymous with symptom bothersomeness in patients with advanced cancer. The lack of consistent correspondence between severity and bothersomeness in our study aligns with previous findings, suggesting that symptom severity and symptom bothersomeness are only moderately correlated. 15 Similarly, it has been reported that highly distressing symptoms do not necessarily have the highest severity scores.21,22 The symptom experience is understood to encompass more than just severity: frequency, duration, chronicity, interference, and patients' subjective experiences of their symptoms may all contribute to the bothersomeness of a symptom and, therefore, play key roles in symptom management. 23 Severity is a crucial aspect of symptom experience and has been shown to be the top contributor to changes in quality of life for patients with advanced cancer. 24 However, ESAS severity responses should trigger an in-depth patient-centered assessment of the extent of bothersomeness of corresponding symptoms and their specific physical, emotional, and psychosocial impact.
That pain and tiredness were almost always among the top most bothersome symptoms reported likely relates to the nature of these two symptoms. It may be difficult to ignore their presence even at mild levels, and they may exacerbate, or be exacerbated by, other symptoms. Cancer pain is also particularly difficult to manage due to the multitude of factors that can either influence patients' subjective experience of pain (e.g., cultural, emotional, behavioral, and spiritual) or the success of their pain treatment (e.g., side effects, adherence, and comorbidities). 25 Similarly, tiredness is one of the most common and troublesome symptoms of cancer. 26 Cancer-related fatigue is persistent and debilitating and interferes with employment, social relationships, daily activities, and other important aspects of a patient's quality of life.27,28
Appetite was frequently rated as the most severe symptom but was rarely perceived as the most bothersome. Indeed, for patients who rated appetite as their most severe symptom, it did not appear in the top three most bothersome symptoms, which were instead pain, tiredness, and nausea. Although anorexia may be profound in patients with cancer, and may be associated with loss of weight and weakness, 29 the loss of appetite itself may not be prioritized as bothersome by patients compared with other symptoms, since it is an expected consequence of cancer and is understood that little can be done to alleviate it. Symptoms such as pain and nausea may also cause or exacerbate anorexia, and appetite may improve when these secondary causes are treated. 29 Family members tend to place more importance on anorexia than patients themselves, and require counseling on how patients should be allowed to prioritize their own symptom control and how cancer-related cachexia is a complex syndrome that cannot be rectified by increased feeding.30,31
Our data indicated that the average severity of the psychological symptoms, depression and anxiety, tended to be rated highest when a physical symptom was rated as most bothersome. This finding aligns with other studies showing a positive correlation between physical symptoms, particularly tiredness and pain, and psychological symptoms such as anxiety and depression.32–34 Uncontrolled physical symptoms associated with advanced cancer may contribute to and exacerbate depression in this population.35,36 It is noteworthy as well that ESAS cutoff values for depression and anxiety are relatively low, at ≥2/10 and ≥3/10, respectively.37,38 This corresponds to the mean ESAS rating for anxiety and depression of 2.55 and 3.17 in the “most bothersome but not most severe” category.
Our study has strengths and limitations. The sample size was large and consisted of a balanced proportion of males and females as well as tumor sites. The use of two clinically validated questionnaires to compare symptom severity with symptom bothersomeness is an additional strength. Participants who consented to participate in the randomized controlled trial might have differed from those who did not participate. Patients completed the ESAS questionnaire before the QUAL-E, which may have influenced patients to choose their most bothersome symptom from the symptoms written on the ESAS. Matching QUAL-E symptoms with ESAS symptoms required subjective judgment, and in some cases there was ambiguity in the terms respondents used to describe their most bothersome symptoms. Lastly, the ESAS and the QUAL-E specify different time frames in which patients rate their symptoms: the ESAS indicates the previous 24 hours, whereas the QUAL-E indicates the previous 7 days for the most bothersome symptom. However, a study conducted on patients in hospice found that although symptoms may fluctuate from day-to-day, this fluctuation is generally small within the span of five days. 39
In conclusion, the symptoms given the highest severity ratings on the ESAS are not necessarily the most bothersome for patients with advanced cancer. Further research should investigate the relative benefit and burden of asking patients to indicate the three most bothersome symptoms on the ESAS questionnaire. This could add another important dimension to symptom assessment and allow health care providers to capture important information that may be hidden by low severity ratings. More comprehensive symptom assessment may, in turn, trigger more effective symptom management in patients with advanced cancer and thereby enhance their quality of life.
Footnotes
Acknowledgments
This study was funded by the Canadian Institutes for Health Research (Grant No. 152996, C.Z.) and the Ontario Ministry of Health and Long Term Care. Dr. Zimmermann is supported by the Rose Family Chair in Supportive Care, Faculty of Medicine, University of Toronto. The views expressed do not necessarily reflect those of the funding agencies, which also had no role in the study design, data collection, analysis and interpretation, writing, or decision to submit for publication.
Author Disclosure Statement
No competing financial interests exist.
Appendix
Symptom Categorization for Matched and Unmatched Quality of Life at the End of Life Symptoms
| ESAS symptoms | QUAL-E most bothersome symptoms reported |
|---|---|
| Pain | Leg pain, liver pain, back pain, some pain, pain in hip, abdominal pain, back/neck pain, back and side chest pain, abdominal soreness–dull aching pain × 4 days, pain in fingertips–left hand, pain in back, pain (left shoulder and lower back), pain and itchiness, pain postpeeing, headache, joint ache, URQ pain, pain in side, pain in right leg and lower back, foot/leg/hand pain, severe pain and inches to right of belly button, pain in joints and muscles from kidney stent, arthritis, arthritic-like soreness, sore hands and feet, heartburn, hand-foot syndrome (cuts in skin), mouth sores, neuropathy, bowel discomfort, sensitivity in left breast (last week), tightness under left armpit, old joint/kneecap injury |
| Tired | Tiredness, lack of energy, no energy, no energy for life, poor energy, moderate decreased energy, lack of usual energy level, decrease in energy, tired/stamina, no energy, feeling tired, exhaustion, tired during Rx, energy level, fatigue |
| Nausea | Nausea (daily) |
| Depression | Mood swings |
| Anxiety | Worry, mild anxiety, worry of dying |
| Drowsy | |
| Appetite | Loss of appetite, lack of appetite, no appetite |
| Shortness of breath | Shortness of breath |
| Constipation | Gastric distress (constipation and gas and diarrhea) |
| Sleep | Lack of restful sleep, poor sleep at night, need to sleep, sleeping problems, waking at night—difficulty getting back to sleep, sleeping (lack of), unable to sleep, lack of sleep, dropping off to sleep |
| Unmatched most bothersome symptoms | Symptom descriptions |
| Bleeding | Bleeding caused by chemo treatment, nose bleeds |
| Bowel problems | Bloating, bloating and nausea, bowels, digestive disruption, bloating, poor digestion |
| Blurred vision | Blurred vision |
| Breast | Breast |
| Chills | Cold-chilled |
| Difficulty concentrating | Inability to concentrate, memory loss, memory loss/confusion, confusion |
| Cough | Cough, coughing to expel mucus in chest, tight lungs–coughing |
| Diarrhea | Diarrhea, loose bowels, frequent bowel movements |
| Difficulty swallowing | Difficulty swallowing, trouble swallowing |
| Dizziness | Dizziness |
| Dry mouth | Dry mouth |
| Dry skin | Dry skin |
| Eye difficulties | Eyes, watery eyes, eye watering |
| Feet/finger numbness and tingling | Feet syndrome, tingling in feet and hands, numbness if feet/fingers, numbness of feet, numbness of fingers and toes, numbness, feet, feet and toes tingle, fingers tingling, finger/nail numbness |
| Frequent urination at night | Frequent urination at night |
| Hiccups | Hiccups |
| Hot flashes | Hot flashes |
| Immobility | Immobility |
| Itchiness | Itchy |
| Lack of sex drive | Lack of sex drive |
| Lymphedema | Lymphedema |
| Sinuses | Sinuses |
| Skin rash | Skin rash |
| Stress | Stress |
| Weakness | Slight weakness, weakness, weakness in legs/difficulty walking, lack of strength |
ESAS, Edmonton Symptom Assessment System; QUAL-E, quality of life at the end of life.