
Abstract
Background:
Communication training is a hallmark of palliative care education. The purpose of this article is to report on the development, exploratory outcomes, and lessons learned from a pilot project, “TeamTalk,” which adapted VitalTalk methodology for interprofessional learners.
Materials and Methods:
TeamTalk included a series of interactive workshops led by an interprofessional faculty team at a health sciences university. Teaching methods were small group discussion, reflection, and high-fidelity simulated patient/family encounters, using a “Skills and Capacities” handout. The course was offered between January and May of 2015 and 2016 to medical fellows, advanced practice nursing students, and chaplain interns. Pre- and post-test design and qualitative data analysis were used to assess the learners' response to the TeamTalk curriculum. Validated instruments assessed attitudes toward interprofessional collaboration and self-confidence for interprofessional communication.
Results:
Sixty-one learners participated in TeamTalk over two academic years. Attitudes toward interprofessional collaboration improved from pre- to post-test (126.1 ± 6.9–130.0 ± 7.1; p < 0.01) with no difference among the professional groups. Self-confidence for interprofessional communication improved in “eliciting the contributions of colleagues, including those from other disciplines” (p < 0.001) for all learners during year two; chaplains improved in the greatest number of areas (15/19), followed by nurses (7/19) and physicians (4/19). Learners expressed appreciation for the opportunity to explore their professional roles together with other professions.
Conclusion:
Preliminary findings indicate that TeamTalk improved attitudes toward interprofessional collaboration and self-confidence for participating on an interprofessional team. The lessons derived from creating and implementing this course may be applicable to interprofessional education in serious illness management.
Background
Acornerstone of effective interprofessional palliative care is sensitive and honest communication among the health care team, patients, and their families. 1 Conversations surrounding serious illness can trigger all participants to experience strong emotions, misunderstandings, and confusion that may interfere with the partnership required to provide or receive optimal care. Communication training is therefore consistently recognized as key to palliative care education 2 for the core professions (physicians, nurses, chaplains, and social workers) on the palliative care team.3–6 Existing formal curricula include the Institute for Healthcare Communication Team and Patient-Centered Communication course, 7 ELNEC-Communication, 8 COMFORT communication, 9 and VitalTalk.10,11
Over the past 20 years, investigators and educators have established key skills for serious illness communication, and effective methods for communication skills training, including training around serious illness.12–15 Key skills include eliciting concerns and responding to emotional and information cues.14–16 Characteristics of effective training programs include: at least a day in length, learner-centered approach, and focus on skills practice, for example, using role play and feedback in a small group setting. 14–16 Although communication curricula that meet these criteria improve individual communication skills, many questions remain about how best to deliver communication training for interprofessional palliative care teams, including whether team members should be trained together, should receive profession-specific training, or both.
VitalTalk is an evidence-based communication training methodology that teaches skills and roadmaps focused on disclosing serious news, discussing prognosis, engaging in advance care planning, and exploring goals of care. VitalTalk education has been shown to improve preparedness for end-of-life communication, and effective communication has been shown to decrease both ICU length of stay and family distress. 17 Although developed by physicians primarily for physicians, all palliative care professionals may take VitalTalk training. 2
The purpose of this article is to report on the development, exploratory outcomes, and lessons learned from a pilot project, TeamTalk, which taught team-based communication skills using an adapted VitalTalk training methodology. VitalTalk was chosen as the communication method for this project because it has a strong evidence base and the faculty who developed this project were all trained as VitalTalk facilitators. Faculty team leaders from the four core palliative care professions developed and taught the course to learners in three of these professions. Exploratory outcomes include attitudes toward interprofessional collaboration, self-confidence for interprofessional communication, and qualitative observations.
Materials and Methods
Exploratory pre- and post-test design and qualitative data collection and analysis were used to assess the learners' response to the TeamTalk curriculum. The courses included interactive workshops led by an interprofessional faculty team in classrooms at a health sciences university. Teaching methods were small group discussion, reflection, and high-fidelity simulated patient/family encounters using a “Skills and Capacities” handout (Supplementary Appendix SA1). The course was offered between January and May in 2015 and 2016. The second year's course was modified based on learner evaluations of the first year's course.
Participants
All nurses, chaplains, and physicians enrolled in the affiliated programs participated both years. Nursing learners were advanced practice nursing students (RNs working toward a masters degree as nurse practitioners or clinical nurse specialists with a palliative care minor). Chaplaincy learners were trainees in the Clinical Pastoral Education (CPE) program at the university medical center. Physician learners were hospice and palliative medicine fellows and geriatrics fellows. All learners were required to participate by their respective educational programs. Although social workers are important members of the core palliative care team, 18 none was available to join these courses.
Structure/content of curriculum
Both iterations of the TeamTalk curriculum were planned and co-led by the faculty team. The year one curriculum consisted of three sessions (Fig. 1A). Based on feedback from year one, two profession-specific sessions were added, and the course consisted of five sessions in year two (Fig. 1B). Both years included an introductory session, a VitalTalk individual skills training session (Fig. 2), and a team skills training session (Fig. 3). In year two, we added a professional identity session, changed the VitalTalk individual skills session to be profession specific, introduced the interprofessional team members in the second session instead of the first, and added a debriefing/reflection session in preparation for the final team skills training session. The complete curriculum plan for year two and simulated patient case are available in Supplementary Appendix SA2.
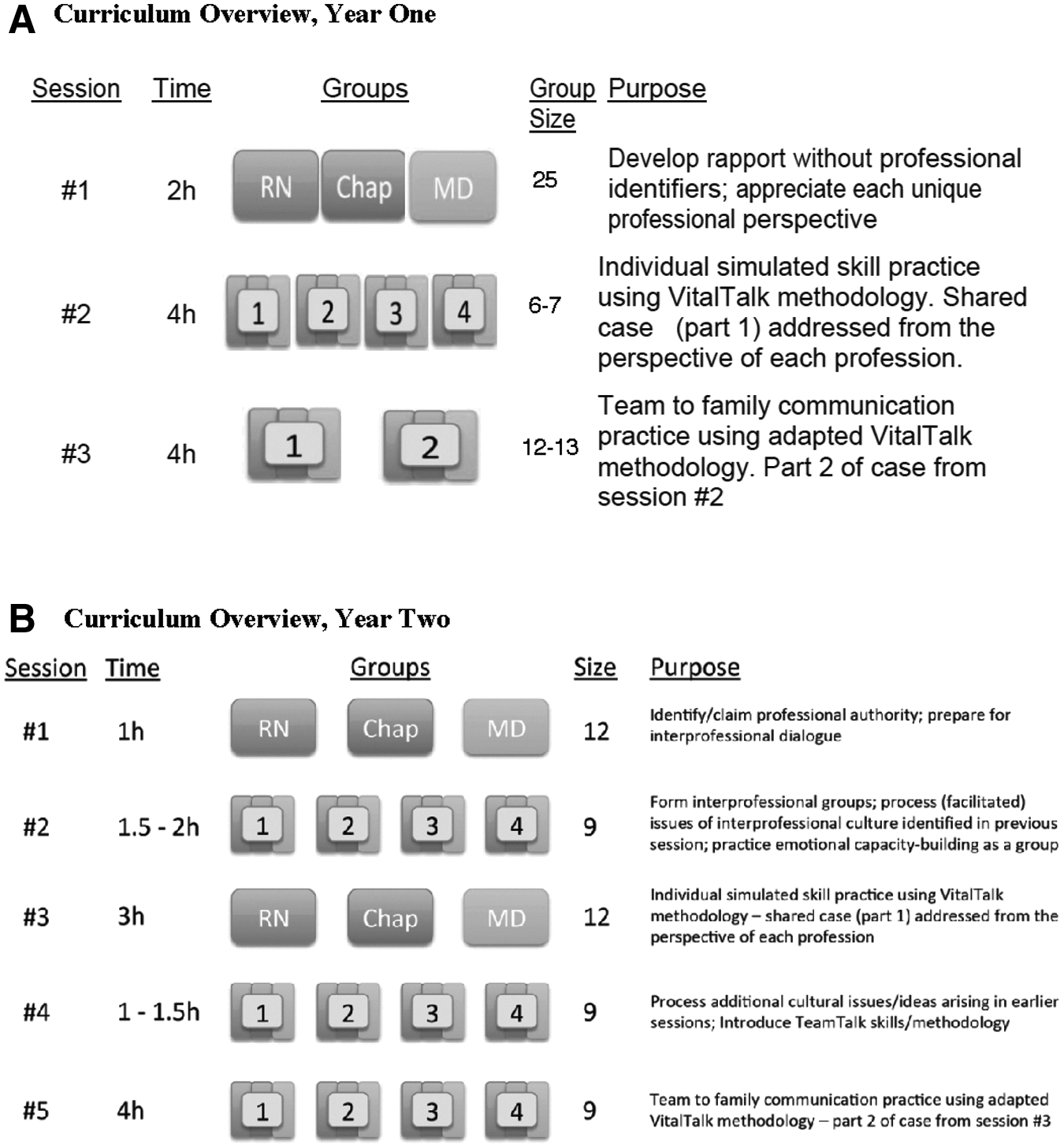
Group numbers indicate interprofessional small group sessions.
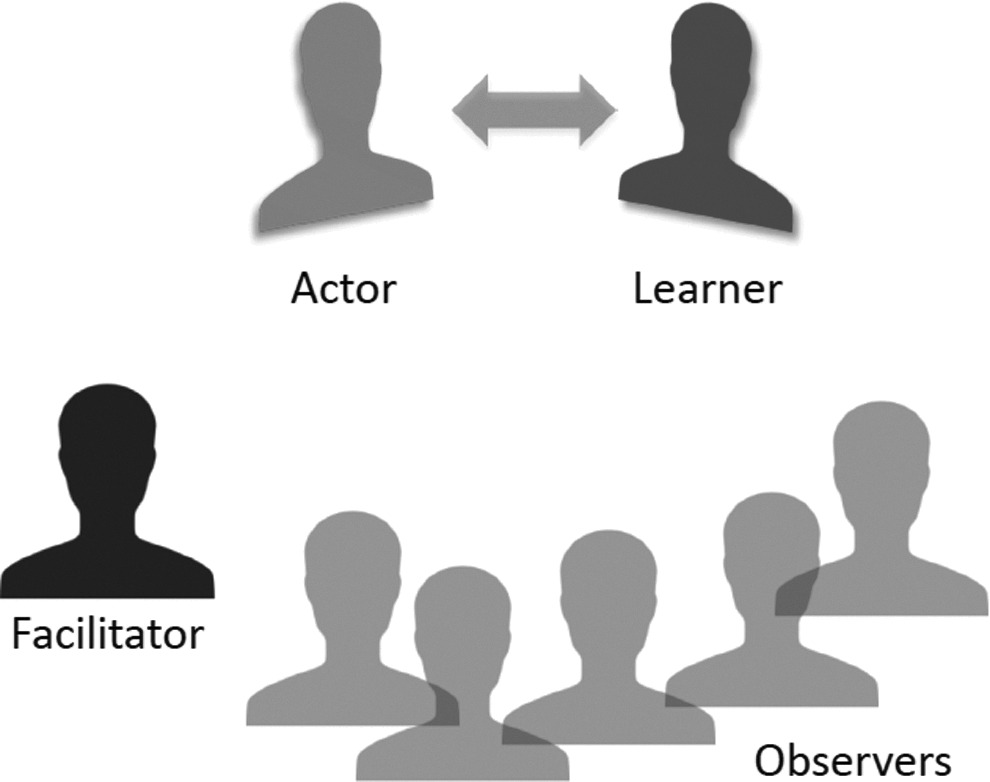
Individual skills practice (session no. 2 during year one, session no. 3 in year two) used the VitalTalk methodology and was delivered by two VitalTalk-trained clinicians of different professions. The VitalTalk session during year one was presented to interprofessional learner groups. The VitalTalk session during year two was profession specific, to enhance the safety of the participants as they learned new skills.
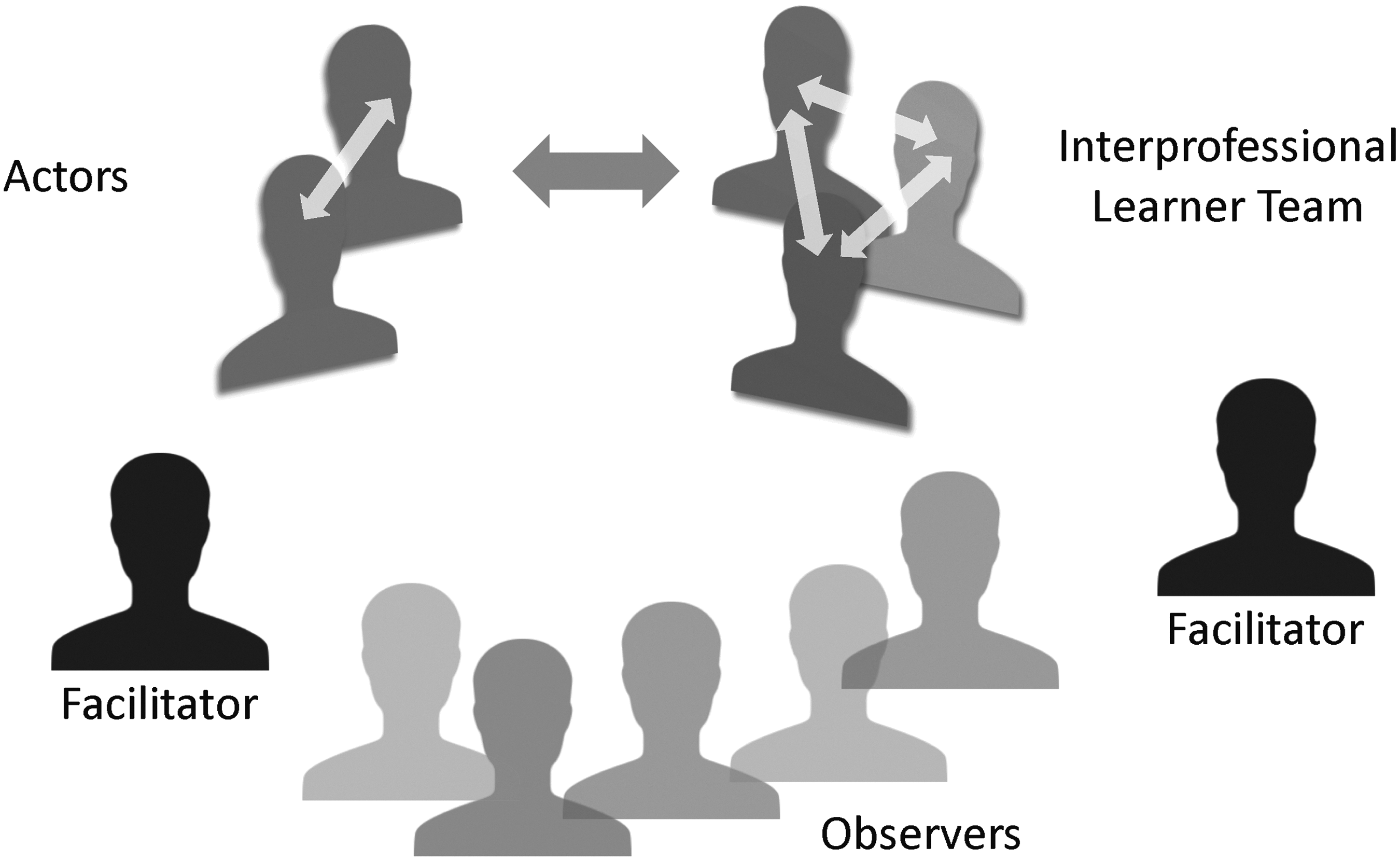
During team skills practice offered during the final session, both years, two actors played a patient and a family member, and two or three learners from different professions worked together during the simulation scenario. The VitalTalk methodology was adapted for use with interprofessional teams during the goal setting and debriefing phases of the interprofessional team skills simulation sessions. Goal setting started with the team identifying a shared team goal and then using that goal to identify individual learner goals. Debriefing began with team self-evaluation focused on the relationships among the team members and generally downplayed individual clinician-to-actor interactions. The learners were then asked to reflect on their performance with both the simulated patient and family, and with the other team members.
High-fidelity simulated patient/family encounters
Professional actors recruited from the university simulation center's referral list served as simulated patients and family members during the role play/simulation. We prepared case scenarios for the actors and learners that included the physiological, psychosocial, spiritual, and cultural context of the simulated patients that would be seen. Actors were trained as previously described.12,19 Briefly, the actors received training materials and cases to review before the training. During the training, the cases were reviewed, and the faculty practiced with the actors to ensure that they had consistent responses to different learner and team behaviors, for example, responding or not responding to emotion, eliciting or not eliciting concerns.
High fidelity in this context refers to the emotional and contextual authenticity of the simulated experience. This was achieved by extensive actor training using scripts that focused on background medical and character detail rather than formulaic or standardized responses to learners. The actor's primary goal is to play the role and respond naturally, immersing the learner in a setting that feels real. Low-fidelity simulation (e.g., role play among the learners themselves), typically seeks to introduce students to new ideas and develop basic comfort with certain scripts or situations. The authenticity of the experience is less critical for these lower-level learning objectives.
Skills and capacities handout
An eight-page “Skills and Capacities” handout (Supplementary Appendix SA1) was developed to serve as the core content of the TeamTalk curriculum. The handout included communication skills, which we defined as “observable actions that support positive communication” and capacities, defined as “reflective internal states” that are not observed externally but support effective communication. 8 We adapted skills and capacities content developed by the VitalTalk organization for use in an interprofessional team setting.
A PubMed literature search for real-time within-team communication skills did not reveal any existing literature. The investigators' own experience was supplemented by interviews with local palliative care clinicians and communication experts to identify skills and capacities associated with real-time patient-facing interprofessional team communication and support. We asked for feedback and comments on the interprofessional skills and capacities from 12 national communication physician leaders attending the 2014 annual American Academy on Communication in Healthcare (AACH) meeting as well as additional citywide palliative care teams at three university medical centers. Discrete skills and capacities for both individual and interprofessional team communications identified through this process were presented in the Skills and Capacities handout for TeamTalk participants (Supplementary Appendix SA1).
Procedures
An administrative staff person was assigned to coordinate the workshops. After obtaining schedules of availability from each of the faculty members, the administrative staff worked with the learners to schedule the large and small group sessions at two- to four-week intervals. Learners were divided into four small groups of eight, each of which had two or three learners from each profession. Two physicians, a nurse, and a chaplain led the faculty team, augmented by additional nurse, chaplain, social worker, and physician faculty so that each small group had two assigned interprofessional faculty leads.
The same patient scripts were used for simulated patient sessions for all small groups during both years. The case involved a woman or man (depending on gender of actor) with interstitial lung disease. The first patient encounter was an outpatient discussion of prognosis and goals of care; the second patient and family encounter was during a hospitalization to discuss serious news (Supplementary Appendix SA2).
Evaluation and data collection
Participants in both years were evaluated with the Jefferson Scale of Attitudes Toward Interprofessional Collaboration (JeffSATIC) tool, and learners' self-confidence was measured by a 10-point self-efficacy survey based on curricular learning objectives. The Institutional Review Board evaluated this project to be “exempt” (RB no. 17–21990).
Attitudes toward interprofessional collaboration
The JeffSATIC tool was designed to “measure attitudes toward interprofessional collaboration in health profession students regardless of their academic backgrounds or areas of practice.” 20 JeffSATIC consists of a total score and two subscales that measure working relationships and accountability. The instrument includes 20 items, with 12 positively worded and 8 reverse scored. All of the positively worded items are included in the working relationship subscale; all of the reverse scored items are included on the accountability subscale. We decided not to use the subscale scores in our analysis. Range of scores is 20–140 with higher scores indicating positive attitudes toward interprofessional collaboration.
Validity testing on three cohorts of interprofessional students revealed mean scores of 114.2 ± 13.5–119.4 ± 16.7; range 30–140. Women obtained higher mean scores than men in all three samples. Medical students consistently scored significantly lower than other students. Students at a university in Australia scored lower than students at two universities in the USA (median 116 vs. 121 or 124). 20 The minimal important difference has not been published for the JeffSATIC.
Self-confidence for communication
Self-efficacy is commonly defined as “self-confidence” for lay audiences. 21 Since actual self-efficacy cannot be measured, perceived self-efficacy is used as a proxy measure, based on what the person believes they can do in a variety of situations. We developed our perceived self-efficacy survey using standardized methodology recommended by Bandura. 22 Perceived self-efficacy must be specific to one activity, so we reframed each of our specific learning objectives into separate perceived self-efficacy ratings measured in intervals from 0 (“cannot do”) to 10 (“certainly can do”), which correspond to the likelihood that the task can be accomplished (Supplementary Appendix SA3). This method of rating self-efficacy is commonly used and well validated in studies of a variety of conditions.23–25
Qualitative analysis
Data for qualitative analysis was collected from written feedback provided by the learners after completion of the course and from faculty debrief discussions after each session. Qualitative data from year one was used to inform the changes implemented in year two. Written learner feedback from year two was evaluated and classified into themes by two of the authors with different professional backgrounds (D.D.; T.T.R.). The two authors met twice to build consensus and then presented their thematic analysis to the other authors for discussion and verification.
Analysis plan
Data collected on JeffSATIC and the self-efficacy survey were entered into SPSS statistical software version 19.0 (IBM Corp., Armonk, NY). We used the JeffSATIC scoring algorithm provided by the JeffSATIC authors to prepare the survey instrument for analysis. Mean and standard deviations were calculated for each year, and for profession-specific groups. Paired sample t-tests were used to calculate statistically significant differences between pre- and post-tests.
Results
During the first year, 25 learners were split among Advanced Practice Nursing students (n = 8), Geriatrics, Hospice, and Palliative Medicine fellow physicians (n = 8), and Chaplain Interns (n = 9). All of the learners were female except two male physicians. During year two, 36 learners were split among the same three professional groups (10 physicians; 12 nurses; 14 chaplains). Ten learners were male, including one physician, four nurses, and five chaplains.
Attitudes toward interprofessional collaboration
JeffSATIC was only administered as a post-test during year one, so change from pre- to post-test was not analyzed. For year two, there was a statistically significant improvement in JeffSATIC pre/post-test total results (126.1 ± 6.9 to 130.0 ± 7.1; p < 0.01) with no difference between performance of individual professional groups (MD: 126.8 ± 9.8–130.3 ± 7.5; RN: 128.4 ± 3.3–131.9 ± 6.3; Chaplain: 124.8 ± 6.5–129.3 ± 8.3 [p = 0.95]). Means were higher and standard deviation lower at baseline than in the initial validation study of the assessment tool. 20 There was no difference in post-test scores between learners in year one and year two (129.5 ± 7.2 vs. 130.2 ± 7.2).
Self-confidence for communication
Of the 10 self-efficacy topics assessed during the first iteration of the course, the entire group showed significantly improved confidence in two (Table 1). During the second iteration, the overall group improved in 14 of the 19 topics assessed. Chaplains significantly improved in 15 topics, nurses significantly improved in six topics, and physicians in four.
Quantitative Evaluation: Self-Efficacy (Self-Confidence)
For complete question phrasing, please see Supplementary Appendix SA1.
p < 0.05; **p < 0.01; ***p < 0.001.
Qualitative theme analysis
Qualitative feedback from the learners centered around five themes, we evaluated as “Successes,” and four themes we identified as “Challenges” (Table 2).
Qualitative Evaluation Themes
Faculty debriefs
Topics during faculty debriefs included scheduling details, challenges when teaching together, ground rules, and goals given unique learner needs.
Discussion
The TeamTalk series of workshops provided interprofessional palliative care learners an opportunity to explore their personal professional identity and their attitudes about interprofessional practice while experiencing interprofessional teamwork in a high-fidelity communication opportunity with simulated patients/actors. The exploratory outcomes suggest that the experience improved attitudes toward interprofessional collaboration and self-confidence for participating on an interprofessional team, although larger studies are required to confirm those findings. Learners expressed appreciation and enthusiasm for the opportunity to explore their professional identities and roles together with other professions.
Attitudes toward interprofessional collaboration
Similar improvements among the profession-specific groups in attitudes toward interprofessional collaboration from an above-average baseline suggest that the TeamTalk course may increase readiness for interprofessional collaboration, even in a group with relatively positive initial attitudes.
Self-confidence for communication
Iterative development of the curriculum design led to large improvements in self-confidence in year two. While only 2 of 10 perceived self-efficacy measures showed improvement in year one, 14 of 19 perceived self-efficacy measures improved for the group as a whole in year two. Notably, most of the improvement appears to have been driven by the chaplain subgroup, with other professional subgroups showing less robust gains. The reason(s) for this disparity are unclear; it may be because there was a larger number of chaplain participants relative to the other two professions in year two. Alternatively, qualitative chaplain feedback and evaluation suggested that simply being included as equal professional partners was viewed as beneficial relative to the perceived cultural norm of struggling to be included as part of the care team.
Qualitative comments
Consistent with the experience of the instructors, participant comments focused at least as much on intra- and interprofessional culture and dialog as on practical communication skill and capacity practice. During both years, learners commented that the practical skills and capacities provided on the “Skills and Capacities” handout and brought alive through practice were helpful tools to reify concepts of interprofessional collaboration. In fact, many participants desired more practice time, indicating that one four-hour simulation session was not enough practice to fully grasp the intragroup dynamics we aimed to convey.
Learners also noted two practical problems: (1) scheduling, especially the long gaps between sessions during both years, and (2) a perception that learner skill levels were not well matched. The former might be addressed by formatting the course as a two-day intensive, which was not possible in our setting. On the other hand, using an intermittent workshop format supports interleaving, 26 the educational practice of studying various subjects repetitively over time—a practice that has been shown to improve retention.
In both years, learners perceived that the subject matter was “overly basic” for physicians who were also perceived to be more experienced clinicians than the other learner groups. In actuality, although experience was not formally measured, the faculty realized that many of the nurse learners had significantly more years of clinical experience than the physician fellows. Since physicians typically have more experience than other clinicians with conveying prognosis and leading family meetings, we hypothesize that professional culture and role expectations may have been the source of this perception.
Some physician learners from both years commented that when they left openings for other professions to speak during the simulation, they felt their colleagues pushed them to reassert control. The limited time for interprofessional simulation may have been insufficient for learners of other professions to assert themselves in unfamiliar roles. This may also point to the need for more profession-specific work on professional identity to prepare learners for joining an interprofessional team.
The TeamTalk project represents two iterations of an intervention that continues to be refined. The majority of the five-session TeamTalk project has been implemented in Practice-PC, an interprofessional palliative care continuing education course for physicians, nurses, chaplains, and social workers. During Practice-PC, practicing clinicians from throughout the greater San Francisco Bay Area meet for monthly full-day sessions that include VitalTalk and professional identity sessions interleaved with other curriculum cotaught by four faculty from each of the core palliative care professions and focused on the National Consensus Project guidelines and resilience/burnout prevention. The relationships built over time by the interprofessional learner cohort provide an opportunity to learn communication and team skills in an emotionally safe environment. The TeamTalk skills are offered as options for those who already have a level of comfort with the individual communication skills and capacities. The scheduling complexity and financial burden of TeamTalk is relieved when integrated into a continuing education course like Practice-PC.
What we learned
As investigators, our most profound lesson was the fundamental role of interprofessional understanding and dialog, in both the faculty and the learner groups. Interprofessional practice is considered to be the standard of care for the delivery of palliative care. In the traditional paradigm for family meetings, a physician is expected to lead the conversation and act as the authority for most issues, even those outside the physician's core expertise. Interprofessional team members typically observe or play ancillary roles (e.g., providing emotional support or offering limited information at the physician's direction). In our observation, learners steeped in this paradigm tend to slip into their standard roles rather than those that would best help the patient or family. The physician learners accepted a shared leadership model in principle, but became frustrated at what they perceived to be passivity or inaction by their colleagues from other professions.
New skills, capacities, and especially roles are exceedingly difficult to graft onto professional relationships built on the traditional paradigm of physician leadership. Even within our own interprofessional palliative care faculty group, which prides itself on a collaborative team structure, the dynamics of course development uncovered previously unexamined assumptions. When we learned to view frustrations and judgments of our colleagues as indicators of potential interprofessional misunderstanding, we were able to explore our different perspectives and gain insight into interprofessional differences that we had not previously recognized.
The resulting lesson for course development was that interprofessional learners cannot work together effectively until they understand the professional identities, assumptions, and capabilities of their colleagues from different professions. The practical import of this realization is that intra- and interprofessional culture matters as much as practical skill-focused content. A major change from year one to two was an expansion of the time devoted to professional identity, as well as a shift from large to small groups to explore these issues. This change helped to ground learners in their own professions and roles, exposing their assumptions and arousing curiosity about others before they engaged with other professions.
Limitations
There were several limitations to this exploratory study. The learner groups were relatively small and may not be representative of the myriad possible audiences for this intervention. No prelicensure learners were included in these cohorts. As noted elsewhere, it is also unclear if the professional groups were optimally matched in terms of clinical experience.
Although the JeffSATIC tool is well validated for prelicensure learners, it has not been tested in post-licensure learners or chaplains. A minimal important difference has not been identified for JeffSATIC, so we do not know whether the statistically significant changes we measured from pre- to post-test are clinically significant. Additionally, while we did measure learner-perceived self-efficacy and attitude change, we did not measure behavior change or clinical impact. Improvement in communication skills should be measured in future studies. Because all quantitative outcomes were considered exploratory, adjustments were not made for testing multiple hypotheses. Given the exploratory nature of the quantitative findings, the lessons learned from this study are primarily based on qualitative and experiential findings.
Conclusions and Future Directions
Components of the TeamTalk program have already been adapted successfully by colleagues in other institutions for a variety of learning environments and experiences.2,27 Similar trainings are also conducted with prelicensure learners in the context of palliative care education. 28
The skills, capacities, and roles developed to teach intrateam and team-to-patient/family communication in the TeamTalk course relied on a semistructured distillation of expert opinion from a limited number of individuals. Future studies might observe highly functional intact interprofessional teams to refine and validate our framework. It would be interesting to offer TeamTalk to intact teams and evaluate whether their interactions improve. Training intact teams that frequently engage together in patient/family interactions might help to ensure a similar level of learner experience, but would exclude a majority of learners and would ignore the often ad hoc nature of many such interactions.
The lessons derived from creating and implementing this course are more broadly applicable to interprofessional education in serious illness management. TeamTalk provides a methodology for training team members from multiple professional backgrounds with communication tools to successfully navigate messy real-world communications with patients, families, and colleagues.
Footnotes
Acknowledgments
Michelle Milic, MD initially conceptualized the TeamTalk project and graciously provided her enthusiastic support for the project development after she moved to a new institution. The authors express appreciation to Susan Barbour, MS, RN, Bentley Stewart, BCC, and Lynn Flint, MD for their collaboration on planning and facilitating the small groups during this project. The authors appreciate the editorial assistance of Melanie Fisch.
Author Disclosure Statement
W.A. is the director of the San Francisco Bay Area Vitaltalk Hub and all other authors declare that no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.