
Abstract
Background:
Patients receiving palliative care often interact with a variety of health care providers across various settings. While patients may experience good care from these services, the connection between these can be disjointed as care providers may work siloed from each other. This is particularly true in out-of-hospital and hospital emergency settings, where providers have no prior knowledge of the patient, particularly their advanced directives (ADs) and goals of care. In the Emergency Department or when paramedics respond to the home, ADs are further challenged by issues of clarity of content, contextual relevance, and accessibility.
Objectives:
(1) What content should be in AD for medical emergencies, and (2) what would ensure the AD is accessible in times of crisis?
Design:
Phase 1 involved a review of existing AD and published literature to generate a list of candidate elements. Phase 2 presented these in an online survey using modified Delphi method to paramedics, emergency nurses, and physicians. During phase 3, a focus group with palliative and emergency care providers and information technology experts was held regarding current accessibility of AD and a vision for improvement. The detailed focus group notes were coded using inductive analysis.
Results:
Fifty-five candidate elements were provided for the Delphi. After three rounds, 36 panelists achieved consensus on 46 elements. Participation was greater than 80% in all rounds. From the focus group on access, six themes emerged; (1) imprecise language, (2) mismatch of protocols, (3) lack of understanding by patients/families, (4) lack of AD, (5) difficulty accessing AD, and (6) opportunities: database, education.
Conclusion:
This project makes recommendations to improve palliative care in emergency or crisis situations and facilitate care consistent with patient's goals: (1) a consensus-based template for AD content; and (2) development of a centralized database. These findings served as the foundation for the “Paramedics Providing Palliative Care at Home” program.
Background
An advance directive (AD) aims to ensure individual and family's wishes are respected, including the noninitiation of nonbeneficial care, (de)escalation of therapy, and location of care and death. 1 In palliative care, patients/families navigate through multiple heath care providers/teams, systems/departments, and settings through their journey of care. Often these providers/teams/systems work exclusively within their own predefined roles and responsibilities, which creates silos particularly in terms of communication, continuity of care, and the gray areas between providers and points of transitions in care.2,3 Silos between the diverse health care professionals who care for patients with palliative goals of care are a key barrier to the shared intention to fulfill these wishes, due to differences in language/jargon, scopes of practice, technology, and protocols.4,5
These silos are even more evident in an emergency or crisis, where providers (emergency medicine physicians, nurses, paramedics) have no prior knowledge of the patient's values or goals of care.6,7 In these moments, where there is an urgency for action, the default is to follow usual care protocols. In the North American out-of-hospital setting, this includes transport to the Emergency Department (ED) and aggressive resuscitation. 8
The goal of this mixed methods study is to explore how ADs may be used as a tool to facilitate improved communication and care and remove the barriers that prevent this between those who write AD, those who use them to guide care, and those who have means to make them accessible.
Objective
The research question is twofold: (1) what content should be in an AD for emergency settings, and (2) what mechanism would ensure the AD is accessible in times of crisis?
Methods/Design
This study is a multiphase mixed methods study that included a literature review, quantitative Delphi survey, and qualitative focus group.
Setting
This study took place between August 2011 and February 2012 in Nova Scotia, Canada. Paramedics, emergency physicians, and nurses who participated were currently registered and actively working in their respective fields. At the time, residential hospice was not an option.
Ethics
The IWK Health Center Research Ethics Board approved this study.
Study protocol
Phase 1: Focused on AD content
To first summarize elements used in local practice, a single research assistant manually abstracted AD content elements, using a template (Appendix A1) built a priori on the expert opinion of our study team of emergency and palliative clinicians, from a binder kept in the ED of the regional tertiary care children's hospital. The research assistant would indicate whether the named element was used, and could add new elements as they were discovered through the abstraction process. This binder was the only centralized source of province-wide AD in our jurisdiction and was felt to represent a broad cross-section of AD. The research assistant was a working paramedic with good knowledge of relevant terminology and reviewed the initial ten abstractions with the study principal investigator (PI) to ensure quality of abstraction.
Second, a single trained and experienced library information scientist (Master in Library Sciences) conducted a detailed literature review (November 7, 2011) in PubMed/Medline, CINAHL, and EMBASE, seeking input from published literature regarding AD content elements in other systems. The following headings were used and applied across databases: ((“Palliative Care”[Mesh]) OR (“Terminal Care”[Mesh]) OR (“PALLIATIVE CARE”[TIAB] OR “END OF LIFE”[TIAB] OR “TERMINAL CARE”[TIAB])) AND ((“Cardiopulmonary Resuscitation”[Mesh] OR “Resuscitation Orders”[Mesh] OR “Resuscitation”[Mesh]) OR ((“Advance Directives”[Mesh]) OR (“Living Wills”[Mesh]) OR (“Emergency Treatment”[Mesh]) OR (“Advance Care Planning”[Mesh]) OR (“Medical Records”[Mesh]) OR (“LIFE-SUSTAINING TREATMENT”[TIAB] OR “LIFE SUSTAINING TREATMENT”)) OR (“ADVANCE DIRECTIVE”[TIAB] OR “ADVANCE DIRECTIVES”[TIAB] OR “LIVING WILL”[TIAB] OR “LIVING WILLS”[TIAB] OR RESUSCITATION*[TIAB] OR “EMERGENCY TREATMENT”[TIAB] OR “EMERGENCY TREATMENTS”[TIAB])) AND (FORMAT[TIAB] OR CONTENT[TIAB] OR TEMPLATE*[TIAB]). The search was not limited by other characteristics such as age, sex, location of care/facility, medical condition, geography, etc. Abstracts were reviewed by two investigators (two of M.C.G., G.F., or G.M.); those deemed relevant were read in full by one investigator who abstracted AD content elements into the template used in the abstraction from local AD in use (one of M.C.G., G.F., or G.M.).
Phase 2
The AD content elements from phase 1 were assembled in an online survey, including all of the elements identified in the literature review and the abstraction from the binder of local AD, to attempt to offer to the respondent a complete and evidence-informed list of potential elements. An invitation was emailed to all paramedics registered in the province, and a recruitment poster for emergency physicians and nurses was mailed to all EDs in the province; interested parties contacted the PI. If more responses than required were received from a given professional group, a panel was purposefully selected to represent diverse experience (e.g., number of years on the job, training level, etc.), geography (rural and urban), and balance between type of professions. Self-selection is anticipated, resulting in participants who are well informed and engaged in the purpose of the research.
Modified Delphi methodology was used, using multiple rounds of structured edits and feedback on a proposal to reach consensus. In this methodology, panelists with expertise in the subject area (in this case their own clinical practice) offer their opinion in consecutive rounds, by which a consensus can be reached by step-wise elimination of responses reaching, or failing to reach, consensus. Results from these relatively small panels are felt to be stable as compared with opinion surveys of much larger groups. 9 Participants completed the survey online using Opinio (Object Planet, Norway). We planned for three rounds; confirmation of the appropriateness of stopping was by saturation and respondent fatigue. Participants scored each item on 5-point Likert scale with this stem: “How useful is this item when caring for a patient with an AD in an emergency.” Participants had the opportunity to add items during the first two rounds, and items not achieving consensus (or added) were presented in the next round. Consensus was defined a priori as 80% overall, and agreement by all professions.
Phase 3
Key informants were selected for a focus group to explore accessibility of AD by purposeful invitation to stakeholders known by members of the study team to have direct interest in the topic, and further supplemented by a snowball technique through which any member or invitee could suggest someone who represented a potentially missed perspective. Participants included medical dispatchers, paramedics, information technology experts from within the health system, palliative care providers, rural and urban ED nurses and physicians, school board, and department of health policy makers.
A trained/experienced facilitator from a third-party research consulting firm specialized in conducting qualitative data collection led the single half-day focus group using a semistructured guide, which was built through several premeeting interviews with the study team and content experts (included as Appendix A2). The facilitator was not previously known to participants. Participants were asked to discuss their experience with accessibility of AD, their vision for the future, and obstacles and opportunities. Detailed field notes taken by the PI (who participated only as an observer) were triangulated with those taken by the facilitator. The session was neither audio nor video recorded, and nobody other than the listed participants and facilitator was present in the closed meeting room.
A grounded theory approach, a systematic methodology by which emergent theories are generated and form a conceptual framework based on the data, was used in the inductive analysis. Open coding was conducted by two study members (A.C., M.C.G.) independently, to find the concepts of key importance.10,11 The two coders then met to compare and contrast and resolve coding differences (A.C., M.C.G.). The codes were then examined to form common categories and ultimately broader themes. During this process, the researchers checked the themes against the original data set to ensure they were not overly influenced by the researchers' interpretations. 12 The codes were grouped into broader categories which allowed the main themes to emerge, which were validated by discussions between members of the research team (validation by respondents was not financially feasible).
Results
Phase 1: Content
Review of existing directives: 120 directives were found in the binder of provincial palliative care directives at the children's hospital and all were included/abstracted by the research assistant (RA)
Review of published literature: 126 titles; after review of title and abstract, 36 articles were read for full text. Any element proposed in the articles was included in the survey (Table 1).
Candidate Elements Based on Local Practice and Literature Review
AD, advanced directive; CPR, cardiopulmonary resuscitation; DNR, do not resuscitate; HPI, history of presenting illness; ME, medical examiner; OR, operating room; PMH, past medical history; POA, power of attorney.
Phase 2: Delphi
Thirty-six participants made up the Delphi panel with 55% being paramedics and the remaining nurses and physicians. All nurse and physician respondents were included, due to poor response from these groups despite multiple varied strategies. Paramedic panelists were selected based on the strategy described in the methods to ensure representativeness and approach a balanced sample. The group were 61.5% male with an average of 13.8 years of experience in their respective fields. The survey included 55 items (Table 2).
Delphi Panel Participants
Elements were added/clarified in round 1 and 2. After three rounds, 46 unique elements were retained. Participation was greater than 80% in all rounds (Fig. 1). The final template of 46 elements is summarized in Table 3, and listed in detail in Table 4.
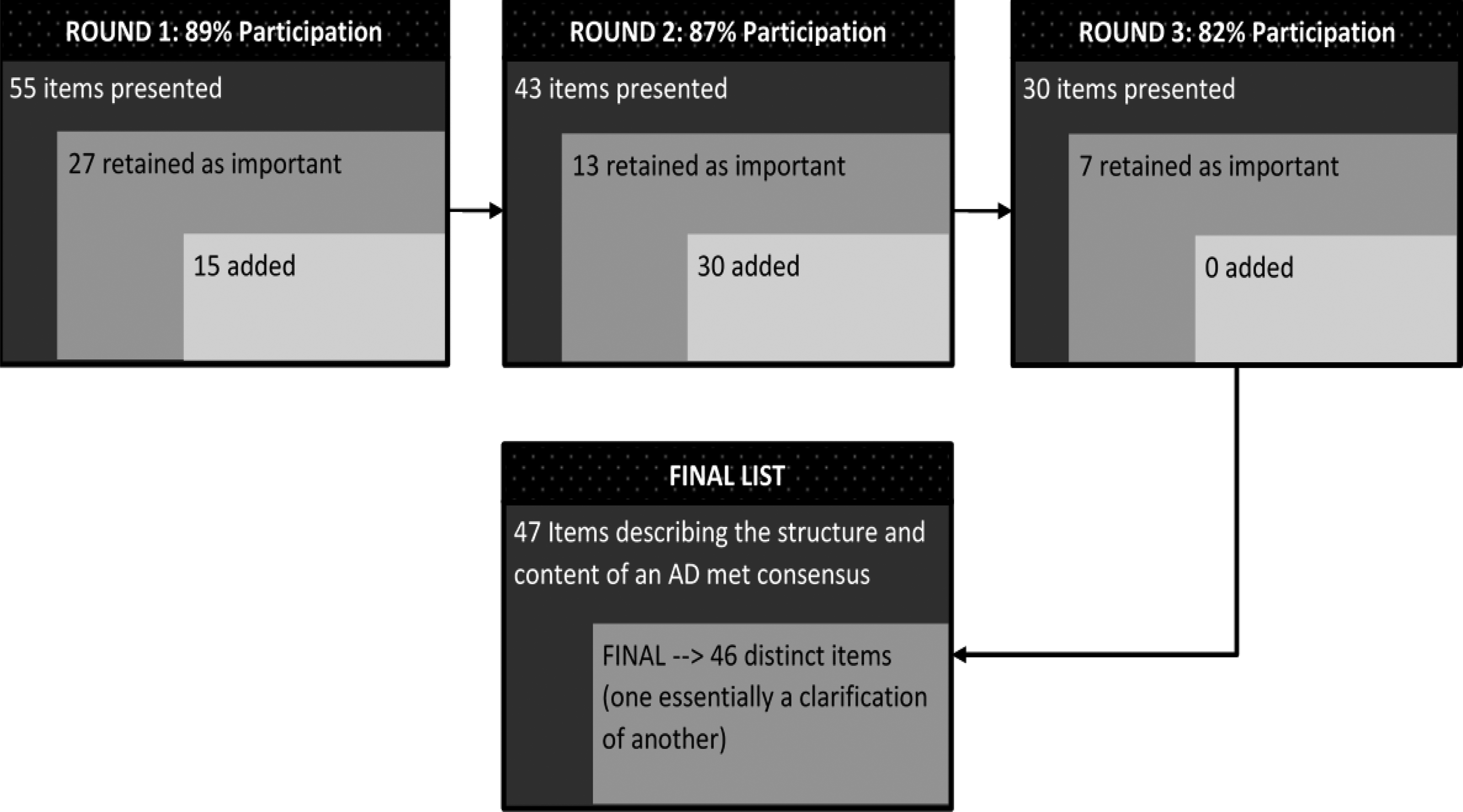
Participation and item consensus.
Summary of Final Content Recommendations for Advanced Directive
An itemized list is available in Table 4.
Consensus Content for Advance Directive Template
Phase 3: Focus group
A total of 13 stakeholders participated in the focus group, including:
two emergency physicians (female) one administrative (female) one IT specialist from medical communications (male) two paramedics (male) one pediatric palliative care physician (female) one palliative care nurse practitioner (female) two palliative care nurses (female) one school board administrator (female) one department of health administrator (female). facilitator (female)
Theme 1: Inconsistent/imprecise language
Participants felt that ADs were often unclear due, in part, to imprecise, unclear or inconsistent terminology/language such as “do not resuscitate,” “allow natural death,” “no heroic measures.” These terms do not provide clear direction in a time of nonarrest crisis. This was seen as particularly challenging for paramedics, ED physicians, and nurses as a preexisting relationship with the patient was not present to provide insight into care wishes; participants specifically noted that gray areas are problematic.
Theme 2: Mismatch of protocols
A mismatch between the expectations of the providers who write an AD and the scope of practice/training of paramedics who attempt to fulfill that AD was identified.
Theme 3: Lack of understanding by patients/families
Participants described misconceptions as barriers to ADs, including patients/families fearing ADs to mean withholding all care, that a decision cannot be changed once written/signed, and feelings of “signing a death warrant.” Participants also indicated that families do not know when to present an AD, as stated by one participant: “is now the time to show it?” and emphasized the need to ensure all families are aware of the AD.
Theme 4: Lack of AD
Participants highlighted a lack of AD as a common occurrence. Some suspected this was more common in rural areas, where patients were more likely to lack a primary care provider. ADs were felt to be more common when the patient was hospitalized, but the content may not translate easily into the home/community setting.
Theme 5: Difficulty accessing AD
In the home, AD documents were noted as being not easily accessible/available (e.g., off site, nonidentifiable binder or folder, hard to find within a binder, etc.) and may suffer from version control issues. The school setting raised unique challenges, where participants described a lack of awareness (“there are no children with AD in schools”), and paramedics described lack of willingness by schools to share the AD until the parents/guardians arrived. The long-term care setting was also highlighted by paramedics who note responding to different facilities resulted in an array of AD, which were at times difficult to understand and carry out.
Opportunities
In the remaining time of the focus group, opportunities to achieve an ideal future state for accessibility of AD by emergency health care providers were suggested by participants and explored.
Accessibility: To have an electronic, centralized database of AD developed by the patient/care team and made accessible to the emergency health system, including an out-of-hospital setting.
Standardized AD: A standardized AD form with consistent language, including both medical and lay terminology. It should not merely address the moment of death and whether to begin cardiopulmonary resuscitation (CPR)/resuscitation, but also symptom crises (e.g., breathlessness, pain, nausea, etc.).
Communication and knowledge translation: A mechanism to “close the loop” back to the usual care team when emergency support was provided. Also promotion and communication about the standardized AD to facilitate use and uptake. Paramedic protocols for care at home: Allowing paramedics to work more effectively in a manner that respects the AD (e.g., type of support, location of care and death). As put by one participant: “I would love to offer them something so they can stay home and don't have to be dragged in the middle of the night.”
Limitations
There was some difficulty in recruiting nurses and physicians and thus these groups are under-represented, but we required that consensus be achieved across all groups, and participation was greater than 80% in all rounds. The relatively small sample size of the qualitative portion of the study should be also considered in considering the findings—a larger sample set may have provided differing perspectives not captured in this study, however, the stability of Delphi panels of this size has been demonstrated. This work did not include the patient/family voice as it was focused on what emergency clinicians needed in a crisis; likewise although the candidate elements were selected by palliative experts, the respondents were all emergency clinicians indicating their perspective. Before implementation, patient/family, palliative, emergency medical services (EMS), and ED perspectives were consulted. The Delphi process, the sampling frame (purposeful selection), and snowball technique present inherent limitations and may lead to bias. We have attempted to adhere to Consolidated Criteria for Reporting Qualitative Research (COREQ) reporting of the focus group; however, it is not possible to reconstruct some of the checklist; of note transcripts/summary notes/themes were not returned to participants for verification, and although themes were clear and agreed upon by the two coders by consensus, a specific inter-rater reliability was not calculated, and it is not always possible to support themes with direct, attributable quotes from participants. It is noted that new literature has been published since the survey was built and template developed; this is mitigated by the opportunity participants had to add items, and the template is a living document. Finally, this consensus is derived from a single paramedic-based provincial health system.
Discussion
The findings of this study point to the importance of not simply having an AD in place, but that ensuring the content is clear, understood, and available across health care providers/settings is critical. Families need to be involved in and understand the purpose of the AD to help alleviate fears commonly associated with an AD and need to be educated about when they present this during an emergency. This study highlights the opportunities associated with AD, as a key tool to help break down silos between community and emergency, proposing its content and mechanisms of access which may help improve the palliative care experience during a crisis. This study specifically addresses a means of ensuring the AD is also designed to be helpful to ED physicians and nurses, and to paramedics in the out-of-hospital setting. These settings are not studied as often, and in particular the role of paramedics in providing palliative care is emerging.
ADs provide a mechanism to clarify and share goals of care. They can provide critical direction to health care providers in times of crisis, particularly in the ED and out-of-hospital settings where there is no prior relationship with the patient. 6 However, silos exist as a variety of health care providers may play roles in patient care but they tend to work parallel to one another, in an uncoordinated fashion, rather than collaboratively. 13 They separate the stakeholders who write AD and those who try to follow them; health professionals attempting to provide care consistent with AD in a crisis may find it challenging to understand and apply goals in the context of their setting and scope of practice.39–42 Various reasons for this were cited by our participants and in the published literature, including lack of training, differences in language, legal or policy constraints, and lack of access or clear content.40–42 This conflict often results in defaulting to usual care: transport and resuscitate. ADs should have clarity of meaning across the multitude of interdisciplinary providers and be available/accessible in a variety of in- and out-of-hospital settings.7,41 Burnod et al. reported on a study comparing a group of patients for whom the out-of-hospital care team provided care without speaking with the palliative care provider or referring to the care plan, to a group where that collaboration did occur. They found that the siloed approach (no collaboration) resulted in AD being followed only 40% of the time in the out-of-hospital setting, and collaboration with palliative care networks increased that to 83% of cases. 43 Access to information was a strong theme in all phases of this project, and is echoed in work from Australia by Lord et al. 41 Quality of communication of goals of care decisions has been increasingly recognized as a key element of end-of-life care. 44
This study proposes a method to improve content and accessibility of communication regarding goals of care to health care providers in the emergency setting by presenting an evidence-based template for AD content and structure, built by consensus across emergency health care providers. These 46 recommendations also include guidance for structure which would enhance the content of the AD. This study has several strengths. First, we used an explicit literature search to inform the initial selection of elements for the survey. Second, we used a Delphi process and explicit scoring of importance. Third, the panel included emergency physicians, nurses, and paramedics to refine the final selection of content items. Therefore, the final list of indicators has both face and content validity. Finally, this project also brought together a focus group to examine improving access to the enhanced content.
In the accessibility portion of the project, we sought to understand the current experience, opportunities (e.g., database, education), barriers, and future vision for access to ADs. The focus group highlighted opportunities for targeted knowledge translation and improved care, and an overall recommendation regarding a centralized database. The discussion revealed that long-term care and schools were particularly challenging environments. Inconsistent existence of/awareness or compliance with ADs at long-term care facilities, a setting in which providers might be most consistent and familiar with patients and the end-of-life process, is a challenge. Lack of awareness that children with ADs and complex health needs are present in the school system need to be addressed. Rural physicians also commented on the need for more advance care planning, and awareness in primary and palliative care teams. Also, the public needs to value and be aware of the goals-of-care conversations and documentation. They describe being first to bring up goals of care as ED clinicians, and highlight misperceptions about the intent of AD.
It was strongly supported that a centralized, electronic solution be developed that could be accessed in a variety of settings and updated in a timely fashion. The current Nova Scotia Emergency Health Services Special Patient Program was proposed as a solution. It already was in operation and supporting some populations with ADs across the province but would require some enhancements to meet the vision of electronic, timely, and addressing more than the moment of death. This is similar to the concept of the Palliative Emergency Sheet in a German study, and also the MOLST/POLST guidelines in use in Oregon, although our consensus recommendations expand on the content of each of those to some extent.42,45 This focus group ultimately informed the upgrade of the Special Patient Program, which also presents an opportunity to provide public education on ADs and advance care planning. It is certainly anticipated that the enhanced accessibility of ADs would improve the effectiveness of paramedic-delivered care in the community to those with ADs, and it is hoped that even the existence of such a database could increase awareness, common language, and discussions regarding goals of care.
This type of enhanced communication of end-of-life goals is the subject of other work, as our Western population ages and quality end-of-life care is increasingly recognized as important. 44 European physician-based out-of-hospital systems have begun to approach palliative care goals with a different lens, shifting from that “usual care” approach and, in collaboration with palliative care programs, begin to support comfort care without transport. 46 Australia has begun paramedic-based service in collaboration with their palliative care networks. The Southern Australia system has reported being able to keep 90% of callers home after a palliative care emergency. 47 The United Kingdom National Health Service has also begun to see the role of paramedics in end-of-life care. 48 Our system in Nova Scotia has used the results of this study to develop the Paramedics Providing Palliative Care at Home program, including a paramedic clinical practice guideline, which allows for care at home without transport to the ED and a standardized electronic AD template with set language which is electronically accessible.49,50
Conclusion
Individuals with goals consistent with palliative care needs encounter a range of health care providers. Silos have separated these providers, for example, in- and out-of-hospital settings; and silos separate the writers from the implementers of ADs. This study proposes a consensus-based solution that breaks down silos to facilitate care consistent with expressed wishes and care/death in the preferred location. The first recommendation is that AD must detail the person's wishes not just at end of life, but throughout the journey of palliative care. The standardization of the content and language is critical to ensuring it is understood by a variety of health care providers across settings. The second recommendation is a centralized provincial database accessible to a range of providers. These recommendations serve as the foundation for the development of the Nova Scotia Paramedics Providing Palliative Care at Home program.
Footnotes
Acknowledgments
The authors would like to thank the participants for their time and insights, and also acknowledge the contributions of Ms Michelle Harrison and Dr Judah Goldstein to the final article.
This study was presented as a poster at the National Association of EMS Physician January 2012 Tucson, USA, and as an oral abstract at the Canadian Association of Emergency Physicians June 2012, Ottawa, Canada.
Funding Information
This study was funded by Network for End of Life Studies—Interdisciplinary Capacity Enhancement (NELS-ICE), a CIHR-funded research network.
Author Disclosure Statement
No competing financial interests exist.
Appendix A2. Semistructured Focus Group Guide on Access to Advanced Directive