
Abstract
Background:
Malignant rectal pain (MRP) and tenesmus cause significant morbidity for cancer patients at all stages of disease. There is little evidence to guide management of these symptoms.
Objective:
The objective of this review was to summarize the existing evidence base for palliative management of MRP and tenesmus outside of standard oncologic or surgical management.
Design:
A systematic review of PubMed and Embase was conducted according to PRISMA guidelines using preselected search terms for publications between 1980 and January 2017.
Setting/Subjects:
Studies that described management for patients with tenesmoid pain from malignant tumors of the rectum, anus, or perineum were identified.
Measurements:
The primary outcome was response of pain to treatment.
Results:
The search produced 1412 titles. Twenty articles met criteria for inclusion in the review, including 11 case series and 9 case reports. A variety of treatments were found with most patients receiving interventional procedures, but overall evidence to support any particular intervention is limited and of poor quality.
Conclusions:
This review highlights the limited current evidence base for medical and interventional treatments for MRP and tenesmus. Further study is needed to clarify the best approach to managing these challenging symptoms.
Introduction
Malignant rectal pain (MRP) and tenesmus are often distressing symptoms that can impact quality of life (QOL). They can present in multiple oncologic settings, including primary tumors of the rectum or anus, genitourinary malignancies with direct extension to the rectum or anus, or pelvic metastatic deposits involving the lower pelvic region. These symptoms are frequently difficult to manage given the complex anatomy and innervation of the anorectum.
The rectum travels caudally to the levator ani where it becomes the anal canal, composed of an external (skeletal muscle) and internal (smooth muscle) sphincter.1–3 The pelvic plexus, located laterally and superiorly to the levator ani, innervates the rectum and internal sphincter. It is composed of sympathetic nerves cranially (branches of L1–L3) and parasympathetic nerves caudally (branches of S2–S5). Branches of the pudendal nerve and sacral nerve roots (S2–S5) supply the rectum, levator ani, and external sphincter.2–4 Tumor invasion into this region can subsequently lead to combinations of nociceptive pain, neuropathic pain, and tenesmus (the painful sensation of persistent rectal fullness and incomplete defecation). Tenesmus is felt to be due to smooth muscle stretching and contraction. 5
The complicated pathophysiology of MRP and tenesmus makes this syndrome challenging to manage. Standard cancer pain management strategies include opioids for nociceptive pain and adjuvants such as antidepressants and antiepilectics for neuropathic pain. 6 The purpose of this systematic review is to assess the available evidence for the management of MRP and tenesmus in patients with malignancies involving the anorectal region.
Methods
Search strategy
This systematic review was conducted according to PRISMA guidelines. 7 A systematic search of Pubmed and Embase from 1980 to January 2017 (limited to English language publications) using Medical Subject Heading terms and keywords was compiled by a multidisciplinary team with experience managing MRP and tenesmus (Table 1). In addition, palliative care textbooks were screened for relevant trials and abstracts, as were the United States National Library of Medicine Clinical Trials registry and palliative care and oncology conference proceedings. 8 The bibliographies of included articles were screened for relevant articles.
Search Terms
Study selection
Studies involving patients with rectal or tenesmoid pain secondary to a pelvic malignancy in which the primary outcome was pain management were identified. Studies were first screened by title and then abstract by a single author. Inclusion and exclusion criteria, described in Table 2, were applied to selected articles. Disease-modifying treatments including chemotherapy, radiation, surgery, and tumor ablation were excluded as these treatments themselves can be associated with rectal pain.
Inclusion and Exclusion Criteria
Study assessment and synthesis
Relevant articles were independently graded by two authors using strength of recommendation taxonomy (SORT). 9 The following information was abstracted from each study: author, publication date, design, sample size, age, gender, histology, intervention, and outcome. Patients from each study were pooled according to similar palliative interventions (e.g., drug class and procedure) and discussed descriptively. Data could not be quantitatively pooled in a meta-analysis due to a limitation in study quality and number.
Results
The literature search results are shown in Figure 1. Twenty articles met the inclusion criteria (11 case series and 9 case reports). All were graded as SORT Level 3: other evidence of lower quality. These 20 articles described 40 patients: 13 received medication and 27 received an interventional procedure. The median age was 64 (range 34–83) years. Twenty-two were male, 17 female, and one unknown gender. Twenty-five patients had a gastrointestinal primary tumor, the other 14 had metastatic disease from another primary. One patient was missing data describing the tumor site. Detailed results for patient symptoms, management, response, and potential confounding factors are summarized in Tables 3 and 4.
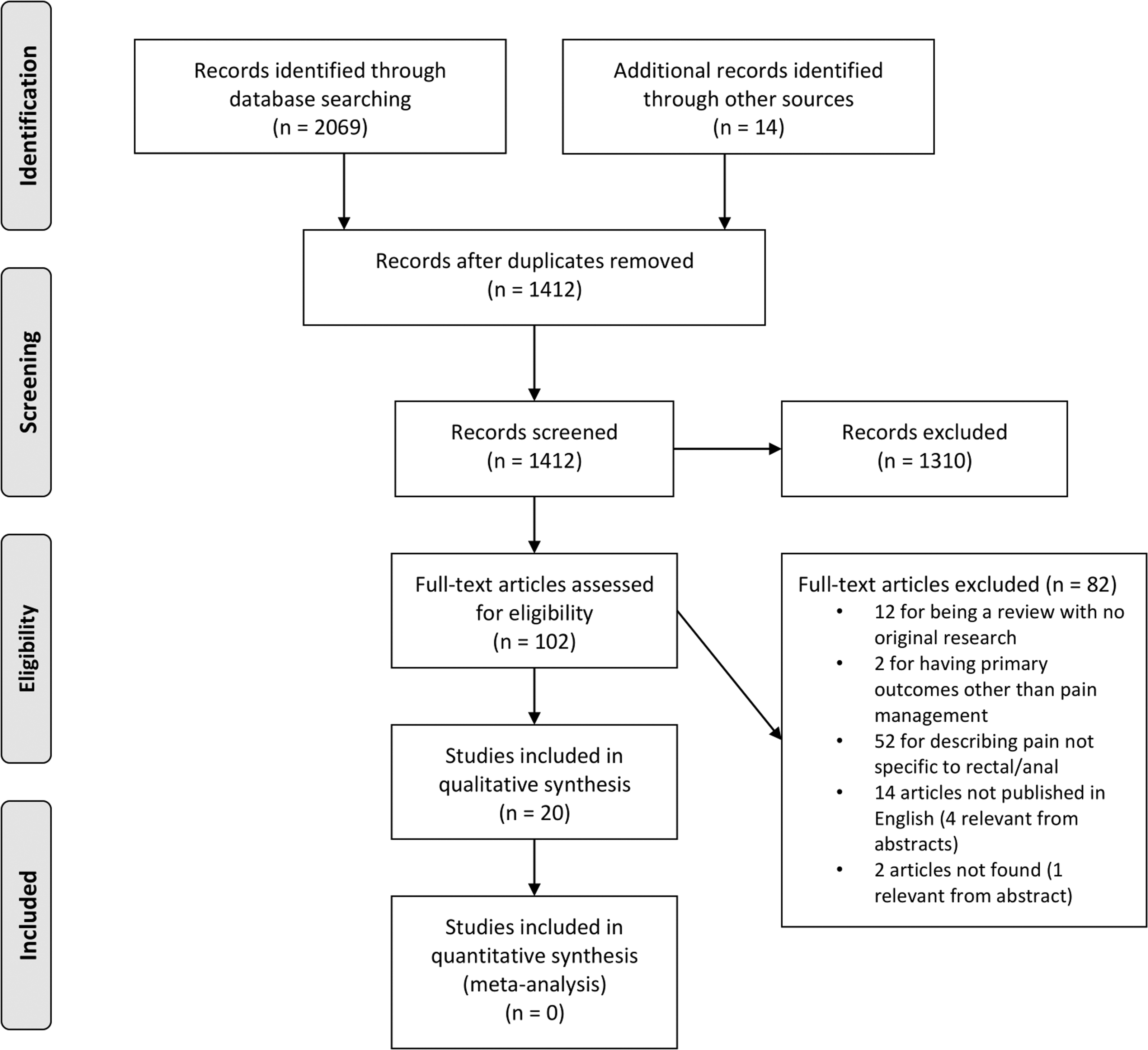
PRISMA flow diagram.
Summary of Patients and Studies Receiving Medical Management
BID, twice daily; Ca, cancer; F, female; IV, intravenous; M, male; TID, three times daily; ?, unknown.
Summary of Patients and Studies Receiving Interventional Management
NSAID, nonsteroidal anti-inflammatory drug; QOL, quality of life; PCA, patient controlled analgesia.
Opioids
Opioids were effective for tenesmus in two patients.10,11 One patient experienced significant pain relief with an opioid rotation from morphine to methadone. A second patient had tenesmus resolution and decreased systemic opioid requirements after the addition of morphine gel per rectum.
Vasodilators
Eight patients received a vasodilator for MRP with or without tenesmus.12–14 Three of four experienced significant relief of tenesmus with nifedipine. 12 Two patients had reduced pain, tenesmus, and opioid requirements with diltiazem. 13 This approach was well tolerated but confounded by the use of other analgesics. Lastly, two patients with anal pain experienced relief with intravenous phentolamine. 14 Of the eight patients in these case series, half experienced hypotension (one requiring ephedrine) and one had a transient arrhythmia.
Local anesthetics
One patient on opioids for a protruding rectal cancer experienced immediate and sustained analgesia after the application of topical lidocaine and prilocaine. 15 Another patient with rectal pain and tenesmus refractory to opioids, ketamine, and midazolam was treated with bupivacaine per rectum. 16 Pain response was achieved within 15 minutes. A higher dose provided 11 hours of pain relief without side effects.
Ketamine
The N-methyl-D-aspartate (NMDA) antagonist, ketamine, was used to treat nociceptive and neuropathic anal and perineal pain in a single patient. 17 The patient's pain improved, but she still needed a saddle block for pain while sitting.
Sympathetic neurolysis
Eighteen patients received sympathetic neurolytic procedures for MRP with or without tenesmus. Twelve received lumbar sympathectomy, with 10 experiencing complete relief of tenesmus. 18 Four patients received a superior hypogastric block resulting in improved MRP and tenesmus in all and significant opioid reduction in three patients.19,20 Two patients received a ganglion impar block.21,22 One had immediate and sustained analgesia for a month. 21 Another patient with severe pain with defecation experienced a significant pain reduction and discontinued multiple analgesics. 22
Neuraxial blockade
Three patients received intrathecal neurolysis.23–25 One patient had complete pain relief with three consecutive blocks lasting ∼10 months until death. 24 The other two patients had >50% reduction in pain and >70% reduction in opioid requirements.23,25 Among the three patients, one experienced transient mild leg weakness 23 and one developed right foot paresthesia and left leg pain. 24
One patient received an epidural phenol neurolysis, resulting in “excellent pain relief” for nine days until death. 26 Another patient received epidural ropivacaine resulting in reversal of motor blockade secondary to bupivacaine. Pain control and QOL improved (described in limited details) for two months until death. 27 An intrathecal morphine and bupivacaine infusion titrated according to pain level were administered in boluses by a pump to another patient. 28 Pain was managed for nearly a year.
Three patients from a prospective consecutive case series had abdominal visceral pain, rectal pain, and tenesmus. 29 After receiving punctate midline myelotomy—cordotomy of the dorsomedial spinal column visceral pain pathway 30 —pain response allowing for opioid reduction varied from transient to 11 months in duration. The only adverse effect was transient urinary retention in one patient.
Conclusions
This systematic review highlights the challenges associated with management of MRP and tenesmus and the limited evidence available to guide treatment decisions. Twenty articles describing 40 patients identified interventions ranging from medications to targeted neurolytic procedures. Although no particular strategy has sufficient evidence to support widespread use, it is useful to consider the reported interventions in the context of their mechanism of action and pathophysiology of MRP and tenesmus. The most commonly reported interventions (18/40 patients) comprised sympathetic neurolytic procedures targeting various levels of the sympathetic nerve supply of the pelvis. These procedures are thought to block the visceral afferents transmitting localized pain and interrupt the sympathetic afferents perpetuating complex sympathetic maintained pain. Vasodilators were the most commonly reported medical intervention (eight patients). Calcium channel blockers (e.g., nifedipine and diltiazem) reduce smooth muscle contraction in the gastrointestinal tract. 31 Phentolamine, an α-adrenergic antagonist, also relaxes smooth muscle and mimics the effect of sympathetic neurolysis in interrupting sympathetic maintained pain. 32 Interestingly, only two patients were successfully palliated with opioids alone. At least 34 patients had symptoms refractory to opioids and at least 25 had no relief with common adjuvants including antidepressants and antiepileptics. These findings would suggest that the standard WHO analgesic ladder alone may not be sufficient for management of MRP and tenesmus. 6
A major limitation of our search strategy was the inability to identify patients with MRP and tenesmus who were enrolled in studies exploring the impact of an intervention on cancer pain. For example, several high-quality studies were excluded for pooling patients into nonspecific pain syndromes such as “pelvic pain.” All studies in this review are case reports or case series at high risk for bias. Some reports have very limited descriptions of the clinical setting, pain etiology and character, and patient demographics. Most do not describe the methodology used to select cases for presentation and were assumed to be retrospective and nonconsecutive in nature, allowing for selection bias. This review highlights the paucity of readily accessible high-quality literature to guide clinicians in the management of MRP and tenesmus.
The complex pathophysiology of MRP and tenesmus combined with the findings of our review may suggest that standard approaches for managing cancer pain alone are insufficient. 6 A combination of interventions that target smooth muscle and autonomic pathways in addition to opioids may be the most logical approach while considering the patient's extent of disease and goals of care.
Footnotes
Funding Information
No funding was received.
Author Disclosure Statement
No competing financial interests exist.