
Abstract
Introduction:
In 2013, the Vermont legislature passed Act 39: The Patient Choice and Control at End-of-Life Act, which legalized medical aid in dying (MAID) under specific circumstances for terminally ill Vermont residents. In the five years since the law was passed, 52 patients in Vermont have been prescribed medications to hasten death; however, important information regarding the experiences of the patient, caregiver, or physician involved in this process is lacking.
Objective:
To survey the subspecialty physicians with the greatest contact with these patient populations, to better understand the physicians' attitudes and experiences with Act 39, and to gather more data about the utilization of Act 39 in Vermont.
Design:
Physicians practicing Hematology/Oncology, Neurology, and/or Palliative Care at the University of Vermont Medical Group and affiliated hospitals in the state of Vermont were invited to participate. Participants were contacted via e-mail to complete blinded surveys, and responses were collected over several months in 2018.
Results:
The attitudes and practices related to Act 39 were collected from 37 subspecialty physicians in Vermont. Seventy-one percent of the participants supported MAID via Act 39; however, many felt that they could use more information and resources to counsel a patient (51.4%) and complete the paperwork and prescription for life-ending medication (37.4%).
Conclusion:
This is the first study to collect information regarding physicians' attitudes and experiences regarding Act 39 in Vermont. Most respondents supported Act 39, but there is a need and desire for more physician education and resources regarding patient counseling and paperwork.
Background
On May 8, 2013 Vermont Governor Peter Shumlin signed into law Act 39, the Patient Choice and Control at the End-of-Life Act, which legalized medical aid in dying (MAID). 1 MAID is available to patients with terminal illness, judged by two physicians to be likely to result in death within six months. 1 Patients must voluntarily submit oral and written requests for the prescription with at least 15 days between requests and the prescription must be written at least 48 hours after the second request. The patient must be a Vermont resident, a voluntary participant, and capable of informed decision making. Prescribing physicians must report to the Department of Health when a prescription is filed under Act 39. 1
Vermont is one of the seven states (Oregon, Washington, Vermont, Montana, California, Colorado, Hawaii, and Washington D.C.) with laws allowing for MAID and was the first state to enact this law through legislative action. 2 In January 2018, the Vermont Department of Health released the first biennial statistical report of information related to Act 39. 3 In the reporting period of May 31, 2013 to June 30, 2017 there were 52 prescriptions generated. 3 The underlying diagnoses for the prescriptions were cancer in 83% of cases (43 total cases), amyotrophic lateral sclerosis (ALS) in 14% (7 cases), and 3% related to other illnesses. Forty-eight of the 52 cases had a death certificate on file, and the remaining four patients are assumed to still be living. Among the 48 confirmed deaths, 60% (29 patients) utilized the patient choice prescription, 35% died from underlying disease (17 patients), and the remaining 2 patients died of other or unknown causes. 3 This information summarizes the mandatory reporting data; however, important information regarding the experiences of physicians practicing in Vermont is lacking. The state legislature allows any Vermont physician to prescribe medication under Act 30, so long as they abide by the legislative process for consenting and reporting. No additional training is required. The goal of this study is to better understand physicians' practices and attitudes related to Act 39 in the five years since its inception in the state of Vermont.
Methods
This study was a self-administered survey that elicited information about physicians' attitudes and experiences regarding Act 39. The survey was composed of 22 questions and developed after discussions with experts in caring for terminally ill patients. Surveys were approved by the Institutional Review Board and distributed via e-mail lists to attending physicians in hematology/oncology, radiation oncology, neurology, and palliative care at the University of Vermont Medical Center and affiliated hospitals in 2018. Participants received an informative e-mail with details about the study and responded via Survey-Monkey, an online survey software. Survey results were collected anonymously and tabulated, and descriptive data analysis was performed by using Microsoft Excel.
Results
Of the 65 physicians contacted regarding our survey, 37 (57%) completed our survey (Table 1). Respondents were 51% neurologists and 35% hematologist/oncologists, and there were more male (62%) than female (35%) participants. The majority (55.6%) of respondents had more than 10 years of experience in their field.
Characteristics of Survey Respondents
Denotes fellowship training after neurology residency, subspecialization within oncology, or second fellowship.
Seventy-one percent of the participants supported MAID via Act 39; however, many felt that they could use more information and resources to counsel a patient (51.4%) and complete the paperwork and prescribe the life-ending medication (37.4%) (Table 2). A few (2.9%) Vermont specialty physicians discuss Act 39 as a part of routine end-of-life conversations, and most (48.6%) engage in this conversation only if the patient specifically inquires about it. The information sources regarding Act 39 that participants use are diverse, and many use their own research on the Internet to stay informed.
Provider Attitudes and Experiences Regarding Medical Aid in Dying, Act 39
Of the 198 patients identified in our survey as requesting information about Act 39, 75 requested a prescription for life-ending medication and 28 filled that prescription (Table 2). Twenty-two patients are known to have used this medication to end their life. Respondents reported that life-ending medication was prescribed for the following diagnoses: ALS, lung cancer, multiple system atrophy, prostate cancer, and brain cancer. Most survey respondents (66.7%) were the consulting providers for a patient requesting a prescription for life-ending medication, and of these providers, 41.7% reported that the prescribing provider was the patient's primary care physician. Although most respondents were not aware of any complications at end of life as a result of Act 39, 26% did report complications, including unsuccessful terminal ingestion, medication side effects, and use of the prescription as a threat against family members to seek more help with care. Forty percent reported barriers to prescribing the life-ending medication, with the most frequent barrier reported being cost. Lack or uncertainty of participating pharmacies and lack of provider education were also reported as barriers. Data on patient circumstances at the end of life were limited, but 9 of the 12 reported patients were enrolled in hospice at the time of requesting a prescription through Act 39. Half of the family members of patients participating in Act 39 received bereavement counseling. Patients reported concerns at the end of their life with loss of autonomy, bodily control, and dignity (Fig. 1).
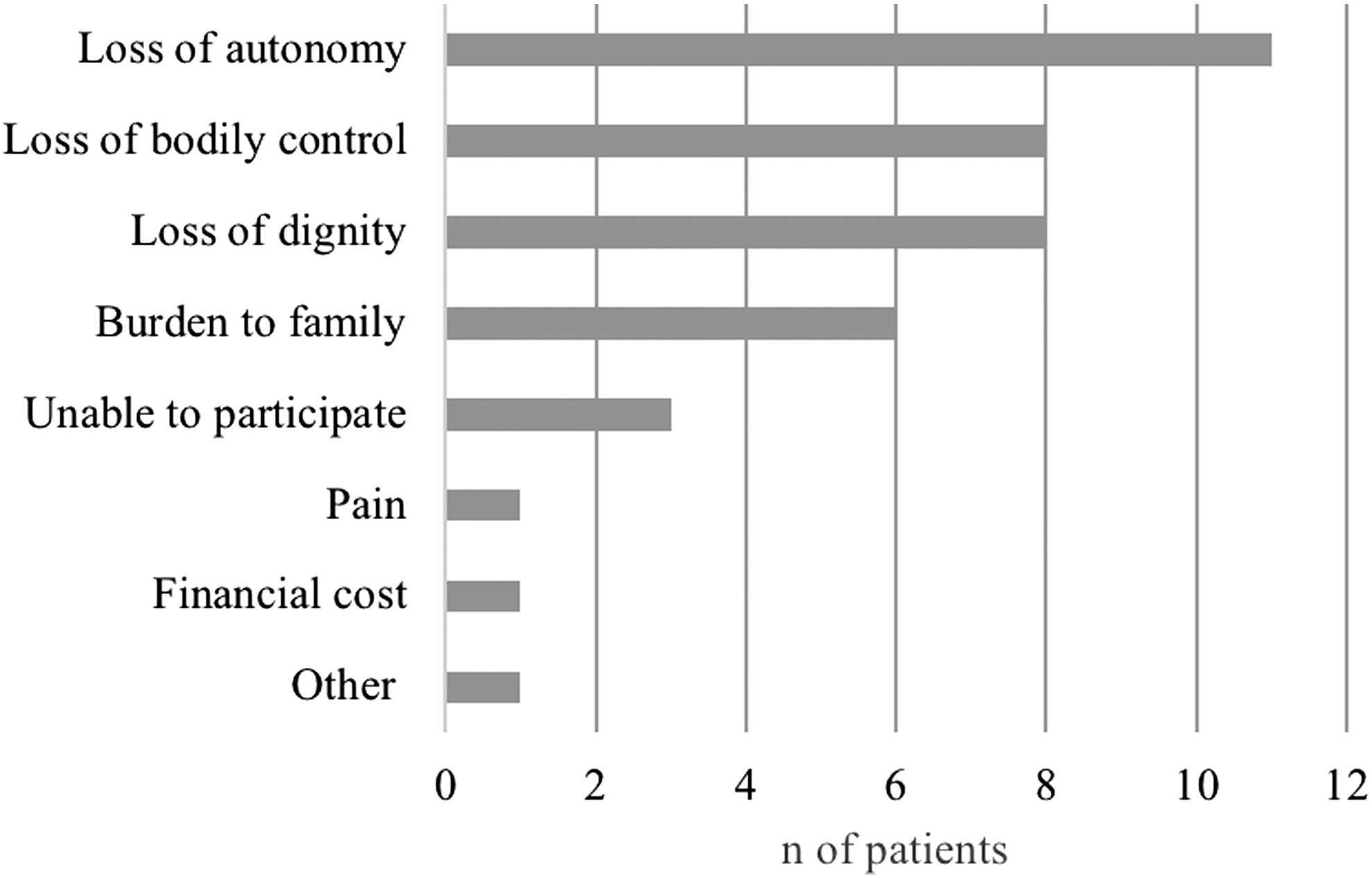
Patients' major concerns at the end of life, as reported by their physicians.
Discussion
The attitudes and practices related to Act 39 were collected from 37 subspecialty physicians in Vermont. The majority of survey respondents supported Act 39, which is consistent with results of a prior survey of U.S. physicians regarding MAID.4,5 Survey participants were subspecialty physicians, mostly experienced neurologists, and oncologists. Since the vast majority of patients involved with Act 39 are patients with neurological or oncologic-qualifying diagnoses (97%), we hypothesized that specialists in neurology, oncology, and related fields of palliative care and radiation oncology would have the most experience and information about Act 39 among Vermont physicians. We were surprised to find that many respondents felt that they needed more information and resources to counsel patients and complete paperwork. This presents an educational opportunity to boost physicians' confidence with the prescribing and counseling process.
In European countries where MAID is legal, including the Netherlands, Belgium, and Luxembourg, national surveys and reporting information give more insight into the patients' end-of-life concerns and the physicians' attitudes about MAID. 4 In Oregon, the Death with Dignity Act reporting requirements include a follow-up questionnaire to be completed by the attending physician documenting whether the patient ingested the medications, the process, any complications, and the patient's end-of-life-concerns. 6 Prior studies have also examined Oregon physicians' attitudes and experiences with MAID. 7 Mandatory reporting data regarding Act 39 in Vermont is limited to basic prescribing data and death reporting, and information regarding the experiences of the patient, caregiver, or physician who exercise this right is lacking. To our knowledge, this is the first study to collect and analyze physicians' attitudes and experiences regarding Act 39 in Vermont. Such information is needed to understand possible complications and barriers as well as to improve the process. 4
Our target population included physicians in cancer-related specialties and neurology at the largest health network in the state of Vermont and the only academic medical center. The state report on Act 39 identified 52 prescriptions for MAID, 97% of which were written for cancer or ALS. Our survey participants reported writing 28 prescriptions, which suggests that our survey respondents represent more than half of the Act 39 prescribers in the state over the past five years. Vermont has more than 2200 practicing physicians, 1 and it is a strength of this survey that a large portion of the MAID participants responded. The prescriptions not accounted for by this survey may have been written by specialists who did not receive or chose not to answer the survey, by specialists in other fields, or by primary care physicians. Five of the 10 respondents to our survey reported that they were acting as consultants for Act 39 prescriptions written by the patient's primary care provider, which suggests that primary care physicians are significantly involved in this process. Even within our survey, the majority of respondents were the consulting physicians for Act 39, and they reported that the patient's primary care physician was the prescribing provider. Our data suggest that community practice and primary care physicians are involved in Act 39 and surveying this physician population may provide a deeper understanding of the application of this law.
Footnotes
Funding Information
No funding was received.
Author Disclosure Statement
No competing financial interests exist.