
Abstract
Background:
The number of hospital-based palliative care consultation teams (PCCTs) has increased in Japan, and quality improvement (QI) of PCCTs is an issue. The Japanese Society for Palliative Medicine is building a framework for continuous QI of PCCT activities.
Objective:
The objective of this study was to develop a program to support QI for PCCTs, and to describe the initial experience with the program.
Design:
The report details the development of a self-check program, followed by a one-year follow-up observational survey.
Methods:
We developed a self-check program using the concept of the Plan-Do-Check-Act (PDCA) cycle and a multidisciplinary expert panel. A total of 114 PCCTs entered the program in the first year.
Results:
We developed three forms for the CHECK, ACT–PLAN, and DO phases aligned with the PDCA cycle. The forms consisted of 34 items across 8 domains. A total of 83 PCCTs (729 members) returned the CHECK, ACT–PLAN forms, and 41 PCCTs returned the DO forms after one year. Overall, 213 high priority issues were identified in the ACT phase. The issues of many PCCTs were “Sharing goals of care is inadequate within the PCCT (33%)” and “Sharing goals of care is inadequate between patient/family or primary team and the PCCT (28%).” Improvements in identified issues were: “achieved” 23% and “almost achieved” 48% after one year.
Conclusions:
We developed a self-check program to support QI efforts for hospital-based PCCTs. The priority issues among PCCTs and improvement goals with examples were identified. These results will support ongoing efforts to develop a continuous improvement model for QI of PCCTs.
Introduction
Palliative care consultation teams (PCCTs) comprising a multidisciplinary group of health care providers improve the quality-of-life of patients and support many with multiple physical, psychological, existential, and social symptoms.1–6 The number of hospital-based PCCTs has increased in several countries, including the UK, the USA, Canada, and Australia, and they play important roles in the health care system.7–10
In Japan, about 75% of deaths occur in hospitals. Hospital-based PCCTs are essential and play an important role in relieving symptoms and improving the quality-of-life of patients. In particular, PCCTs have been established in all cancer hospitals (437 hospitals in 2018) according to the designated cancer hospital system based on the Cancer Control Act established in 2007. The number of patient referrals to PCCTs is increasing steadily. 11 Since 2014, each designated cancer hospital's medical care function has been required to evaluate PCCTs and make systematic improvements through the Plan-Do-Check-Act (PDCA) cycle. 12 The PDCA cycle is an iterative, four-phase management method used in business to improve processes and products. 13 However, it is a challenge to conduct continuous quality improvement (QI) of hospital-based PCCTs.
QI is applied to palliative care on a large scale in accordance with national guidelines and care standards and on a small scale in clinical QI and audit initiatives.14–17 The former is generally the purview of regulatory and oversight bodies and health care payers. The latter arises in the health care system and at the organizational level. A wide variety of individual topic-based audits have led to improvements in practice for managing individual symptoms, coordinate activities, and educate staff.18–22
The new standard for hospital-based PCCTs was developed in a previous study in Japan. 23 This standard indicates the required practices and the role of hospital-based PCCTs. The Palliative Care Consultation Team Self-Check Program Working Group of the Japanese Society for Palliative Medicine (JSPM) is building a framework targeting continuous QI of PCCT activities based on the new standard.
The objectives of this study were as follows: (1) to develop a program to support QI for PCCTs and (2) to describe initial experience with the program, in which the PCCTs check daily practices, identify future priority issues, and develop and implement an action plan through the PDCA cycle.
Methods
This report outlines the development of a self-check program targeting QI in hospital-based PCCTs, followed by a one-year follow-up observational survey.
Program development
To develop a program to improve PCCT practices, we adopted the following procedures. First, the authors discussed the basic assumptions of the program and decided that each facility should aim for the control and continual improvement of PCCT practices. We applied the PDCA cycle concept with reference to the QI program for palliative care units that was previously done in our country.13,24 In accordance with the PDCA cycle, a self-check program was developed (Fig. 1). This program starts with the CHECK phase.

A self-check program summary using the PDCA cycle for quality improvement of palliative care consultation teams. PDCA, Plan-Do-Check-Act.
Second, we developed a form for use in each phase of the PDCA cycle. The forms were prepared by a multidisciplinary expert panel consisting of 10 members (4 physicians, 2 psycho-oncologists, 2 nurses, 1 pharmacist, and 1 medical social worker).
The check items in the CHECK phase were selected according to the basic contents required for PCCT practices based on the Standard for Hospital-based PCCTs in Japan developed in a previous study. 23 The expert panel held a four-hour brainstorming meeting while reviewing the literature in November 2016,12,23,25–28 with subsequent discussions by e-mail over the following three months.
Third, we prepared a procedure manual to guide the implementation of the program. The procedure manual describes how to implement each practice and the key points to consider in each phase. We recommend that each team decides on a program manager to facilitate program execution.
Fourth, we conducted a pilot study with 52 participants in 6 PCCTs and confirmed the feasibility of the program in February 2016. 29 A total of 87% of participants answered that the program was useful to address their issues and make improvements.
Lastly, the developed program was approved by the Specialized Palliative Care Promotion Committee, JSPM, and finally approved by the JSPM board in March 2016.
Formative and implementation evaluation
Survey subjects and procedures
We widely canvassed members of the Japanese Society for Palliative Medicine to participate in the program using leaflets and e-mails or at an academic conference in May–June 2016. As a result, a total of 114 PCCTs entered this program.
The survey forms and the program's procedure manual were sent by e-mail to all team representatives in June 2016.
Implementation evaluation
We asked the teams to return the completed CHECK, ACT, and PLAN forms within three months. One year later, we asked them to return the completed DO form aligned with the PDCA cycle, including a four-level goal achievement assessment: “achieved,” “almost achieved,” “not much achieved,” and “not achieved.”
Formative evaluation
We asked the participants about the usability of, and satisfaction with, the program after three months.
For participants.
Do you find the program useful for improving your team issues?
Could the team members discuss the team issues adequately through the program?
For program managers of participating teams.
How satisfied are you as a manager with the improvement plans created in the program?
Background information on participating PCCTs was linked according to the PCCT registration data of the Specialized Palliative Care Promotion Committee, JSPM, and included the type of hospital, number of beds, presence of full-time members, frequency of direct team medical treatment, and the number of patient referrals. 11 Use of the PCCT registration data was approved by the Specialized Palliative Care Promotion Committee, JSPM.
Data analysis
First, descriptive statistics were calculated for participating teams' characteristics, as well as the formative evaluation, the assessment of CHECK items, and the goal achievement level. Furthermore, to identify factors associated with the structures and the practices of the PCCTs, such as the type of hospital, presence of full-time members, and frequency of direct care or treatment, univariate analyses were conducted using the unpaired t test, ANOVA (analysis of variance), and Pearson's product-moment correlation coefficients where appropriate. Thereafter, the association of each hypothesized factor with the total score of each domain was confirmed using multivariate linear regression. All statistical analyses were carried out using the statistical package SAS version 9.4 (SAS Institute, Inc., Cary, NC).
Second, a content analysis method was used to synthesize the qualitative data regarding high-priority issues in team practices in the Act and Plan form and the reasons for their goal achievement level after one year. The content was analyzed according to the method outlined by Krippendorff. 30 First, units with similar contents were classified into groups and summarized. Next, subcategories were grouped according to similarity, and then subcategories were classified and categories were created. Content analysis was conducted by two researchers (N.Y., K.M.), after which discussions were conducted with two researchers (S.A., K.M.). All six researchers confirmed that the subcategories and categories were appropriate.
Results
The self-check program
CHECK phase: The check items consisted of 34 items across 8 domains, including “Referral to specialist palliative care team,” “Collecting patient information,” “Symptom assessment,” “Care goal-setting,” “Symptom management,” “Care evaluation,” “Improvement practices,” and “Comprehensive assessment.” Each item was evaluated using a five-level Likert scale “Not done,” Not much done,” “Mostly done,” “Done,” and “Undecided.”
ACT and PLAN phase: The ACT and PLAN form was filled in with one to three high-priority issues in terms of team practices discussed at the members meeting as a result of the self-check, improvement goals, and concrete plans.
DO phase: The DO form was filled in with what the team actually did or struggled to do, and the achievement level of goals was assessed using a five-point Likert scale “Not achieved,” “Not much achieved,” “Mostly achieved,” “Achieved,” and “Undecided,” as well as the reasons for the goal achievement level after one year.
For more information, see https://www.jspm.ne.jp/pct/jishisetsu.html (in Japanese).
Response rate and participant characteristics
A total of 83 PCCTs (73%) returned the CHECK, ACT, and PLAN forms in September 2016, and 41 PCCTs (36%) returned the DO forms in September 2017 (Fig. 2). The characteristics of participating PCCTs are summarized in Table 1. A total of 66% of designated cancer hospitals, 77% of hospitals with over 400 beds, and 49% of the PCCTs had full-time physicians, and the average number of in-patient referrals to a team per year was 189 (SD ±150). No demographic differences were observed between the teams that enrolled and those who returned the DO forms. The members of the participating teams are summarized in Table 2. A total of 729 health care professionals participated in the CHECK, ACT, and PLAN phases, and each team had an average of 9.1 members (SD ±4.0). One year later, 418 health care professionals participated in the DO phase, and each team had an average of 11.3 members (SD ±6.7).
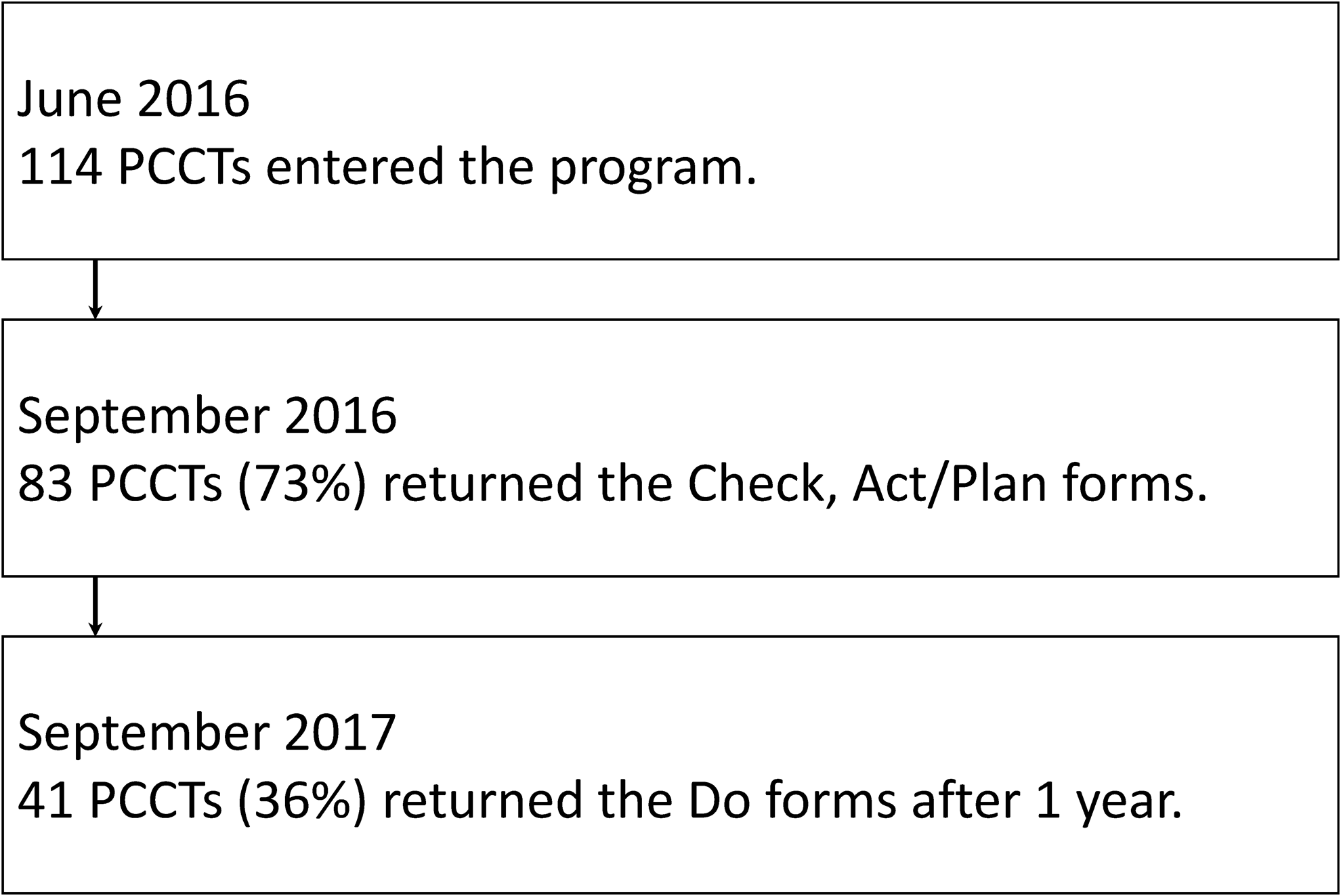
Responses to the follow-up survey after one year.
Backgrounds of the Participating Palliative Care Consultation Teams
A designated cancer hospital is a hospital designated by the Ministry of Health, Labor, and Welfare for the purpose of equalizing cancer medical services throughout Japan. In total, 439 hospitals, including university hospitals and specialist cancer hospitals were declared as designated cancer hospitals in 2017.
PCCT, palliative care consultation team; SD, standard deviation.
Participants in the Self-Check Program
CHECK phase
The items with low mean values were as follows: in the domain “Care goal-setting,” “Set realistic and measurable care goals for symptom relief” (mean ± SD; 2.7 ± 0.7) and “Share goals and expectations for symptom relief with the primary team” (2.9 ± 0.9); in the domain “Improvement practices,” “When a recommendation was not adopted, ask the referring team why” (2.8 ± 0.7) and “When a recommendation was not adopted, consider an alternative approach” (2.8 ± 0.6). Each assessment of the CHECK items is shown in Supplementary Table S1.
Factors associated with check-item score
The results of the univariate analysis showed a significant association with the domain scores for certain variables (Table 3). The number of days the team was directly examining the patient each week was associated with higher scores for the domains such as “Referral to the PCCT” (r = 0.46, p ≤ 0.001), “Symptom management” (r = 0.36, p ≤ 0.01), and “Care evaluation” (r = 0.37, p ≤ 0.001). The number of in-patient referrals to the team was also associated with higher scores for domains such as “Referral to the PCCT” (r = 0.37, p ≤ 0.001), “Care evaluation” (r = 0.34, p ≤ 0.01), and “Improvement practices” (r = 0.34, p ≤ 0.01).
Factors Associated with the CHECK Items According to Univariate Analysis (N = 83)
Numbers in the table represent means or Pearson's correlation coefficients.
p < 0.05, **p < 0.01, ***p < 0.001.
In addition, multivariable linear regression confirmed an association between a higher score and frequency of team direct medical treatment for “Referral to the PCCT” (β = 0.40, p ≤ 0.001), “Symptom management” (β = 0.29, p ≤ 0.05), and “Care evaluation” (β = 0.27, p ≤ 0.05).
ACT and PLAN phase
A total of 83 PCCTs found 213 high-priority issues in the ACT phase, and set goals and action plans for improvements that they wanted to achieve within one year in the PLAN phase. Table 4 summarizes the results of content analysis on the issues, and gives examples of goals for improvement. The following are the issues shared by many PCCTs in descending order and examples of respective improvement goals:
Issues Associated with the Palliative Care Consultation Team Activities Found Thorough the ACT Phase, and the Improvement Goals Set in the PLAN Phase (N = 83)
Issue (1) “Sharing goals of care are inadequate within the PCCT (33%).”
Example of goal (1) “Set short-term and long-term care goals in the first team member meeting or discussion” and “Describe care goals and evaluation criteria in the medical record.”
Issue (2) “Sharing goals of care are inadequate between patient/family or primary team and the PCCT (28%).”
Example of goal (2) “Share care goals using meetings, discussions, and during rounds” and “Enhance medical records by utilizing screening and assessment sheets.”
Issue (3) “Discussions at meetings with the primary team are inadequate (25%).”
Example of goal (3) “Regularly participate in primary team meetings” and “Directly contact the primary team face-to-face or by phone.”
Issue (4) “Assessment at each consultation is inadequate (22%).”
Example of goal (4) “Evaluate after consultation using an assessment sheet” and “Assess the goal achievement level in three steps.”
DO phase and goal achievement
A total of 96 issues reported by 41 PCCTs were assessed for goal achievement after one year. Improvements in identified issues were: “achieved” 22 (23%), “almost achieved” 46 (48%), “not much achieved” 22 (23%), and “not achieved” 6 (6%). The main reasons why the goals could not be achieved were as follows: “The plans could not be carried out due to a manpower shortage or lack of details,” “The goals were inappropriate,” “It is necessary to rediscuss what the problems are,” and “The plans were difficult to sustain.”
Program usability and satisfaction
A total of 527 team members from 83 PCCTs responded regarding the usability of the program, and 489 (93%) = indicated it was useful for improving team activities, 460 (87%) that there were sufficient discussions throughout the program, and 470 (89%) gave their own opinions on the improvement plan.
Of 78 program managers who responded regarding satisfaction with the program, 70 (90%) indicated they were satisfied.
Discussion
A self-check program targeting QI in hospital-based PCCTs
We developed a self-check program to support the QI of hospital-based PCCTs. The most important finding in this study was the development of the first QI program targeting hospital-based PCCTs. The program provides PCCTs with an opportunity for continuous QI using a PDCA cycle model. In particular, we believe that preparation of the procedure for carrying out programs and the use of forms in each phase affected the implementation of QI. We recommended choosing a program manager in the program set-up procedure. The role of the manager during QI efforts is important. The manager is required to summarize the opinions of team members and to take initiatives to improve activities. Although 83 PCCTs completed the improvement action plan in the PLAN phase, about half of these teams did not submit the form for the DO phase that evaluated the goal achievement level after one year. This may have been because it was difficult to coordinate member discussions, the workload of the leader was heavy, or the leader's initiatives were inadequate. It is necessary to improve the program procedure to reduce the manager's workload.
The second finding of this study was to show the essential elements for PCCTs in terms of check items to use in the CHECK phase. Although some studies have described the activities of PCCTs,4,6,31 or recommended consultation etiquette, 32 the essential elements of PCCTs have not been noted. Using the CHECK items, we believe it is possible to focus on specific problems regarding team activities and to review these activities in the QI process. Even so, the CHECK items consisted only of basic team activities; therefore, we will increase the number of assessment domains for patient symptom management.
Issues in terms of hospital-based PCCT activities
The third finding of this study was to identify the main issues and improvement goal examples based on team activities. In the CHECK phase, the mean score for check items was low for setting realistic and measurable care goals, and sharing the care goals and expectations for symptom management with the primary team. However, it should be noted that the overall differences in mean scores were small. The most common as well as the least common items are both informative for QI activities.
The most common issue among the PCCTs was “sharing goals of care is inadequate” within PCCTs, and between patient/family or primary team and PCCTs in the ACT phase after the check. As a general medical issue in Japan, most outpatient medical services take less than 10 minutes. 33 This is likely one reason that not enough time for medical care can be secured for each patient. Therefore, if medical professionals do not have time to communicate verbally, it will be necessary to have nonverbal communication using medical charts and screening sheets, as shown in the improvement goal examples. The PCCTs could work in conjunction with the primary team to facilitate decision making by putting the effectiveness and adverse effects of various therapies into perspective, and allowing patients to acquire the necessary knowledge to select treatments consistent with their goals. At the end of life, palliative care may also help patients to avoid unnecessarily harmful therapies that have no chance of meeting their goals of care. 34
After examining the association between the check score of each team and background factors, the frequency of direct medical examinations by PCCTs and the number of in-patient referrals to the PCCT were related to a higher check score. This suggested that improving the check items leads to a higher number of referrals to the PCCT and improved PCCT motivation.
Herein, we described the experience of the first implementation of this program. In the future, to deliver more effective QI it will be necessary to consider systems to respond and support QI efforts, monitor quality, and give awards for the best QI efforts. Furthermore, indicating the behavioral changes of PCCTs following QI initiatives will be needed.
This study had several limitations. First, the actual objective of the QI program was to improve the quality of life of patients and their families. The feasibility of the program has been confirmed, but it is unclear whether the quality of life of patients and their families was improved. To clarify this, further studies will be needed using patient-reported outcomes. Second, this report produced results for the CHECK, ACT, and PLAN phases for 83 teams out of 114 teams that enrolled; 41 teams completed all phases of the program, but about half of the teams dropped out. The usability and feasibility after completion of all phases and the program effects could not, therefore, be evaluated clearly. Formative and effectiveness evaluations after completing all phases of the program are further issues to be addressed. In addition, the program included five types of health care professionals, but did not include other health care professionals such as a physical therapist, psychotherapists, or dietitians. Furthermore, the psychometrical validity of the program has not been confirmed. These are also future issues. Third, a program that works well in a Japanese hospital setting may not work well elsewhere because of differences in systems and supporting evidence may not translate across settings. Therefore, further research is needed to determine whether the program can be applied to other settings.
Lastly, the optimum check items are constantly changing with advances in science and evolving policy. The check items will need to be updated periodically, just like practice guidelines. We believe that continuous QI efforts will improve the quality of PCCTs in Japan and benefit patients and families.
Conclusion
We developed a self-check program for hospital-based PCCTs to support QI efforts. The priority issues among PCCTs and improvement goal examples throughout the PDCA cycle were examined. These results will support ongoing efforts to develop a continuous improvement model for QI of PCCTs.
Footnotes
Acknowledgments
This study was conducted as part of the Palliative Care Consultation Team Self-Check Program Working Group, Japanese Society for Palliative Medicine. The authors would like to express their gratitude to all participants and the PCCTs for taking part in this study.
Funding Information
Financial support from the Japanese Society for Palliative Medicine has been received for the publication of this study.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.