
Abstract
Background:
Unplanned readmissions or emergency visits (EVs) after discharge from hospital are frequent in patients in palliative care. Strategies to anticipate and prevent rapid deterioration of health are needed.
Objective:
Assessing feasibility and predictive ability of remote monitoring using wearables.
Design:
Prospective observational feasibility study in a single center.
Setting/Subjects:
Thirty cancer patients with an estimated life expectancy of >8 weeks to <12 months, aged >18 years and being discharged from inpatient to outpatient care were included.
Measurements:
Patients were provided with a smartphone, including the preinstalled “Activity Monitoring” application and a sensor-equipped bracelet. Follow-up was 12 weeks. Both devices recorded several features (e.g., vital signs). Visual analog scale (VAS) for pain and distress was reported once daily and European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC QLQ-C30) once weekly. Statistical methods were applied to explore relationship between sensor data, self-reports, and EVs or readmissions or death.
Results:
Between February 2017 and May 2018, 30 patients were included. Twenty-five of 30 participants (83%) completed 12 weeks of follow-up. On average, bracelet was worn on 53% and smartphone on 85% of study days. Completion rate of daily digital questionnaires for subjective ratings was 73%. Eight unplanned hospital readmissions occurred. Ratings of pain, distress, and QLQ-C30 scores were not associated with readmission, whereas resting heart rate, resting heart rate variability, as well as speed of steps differed significantly in patients with and without readmission.
Conclusions:
Monitoring of palliative cancer patients using wearables is feasible. First results indicate that mobile health features might be promising biomarkers to predict unplanned readmissions.
Introduction
Discharge from hospital is a vulnerable phase in trajectories of patients in palliative care, resulting in frequent unplanned readmissions or emergency visits (EVs). Worsening of symptoms such as pain, dyspnea, nausea, or fatigue is a potential consequence of discontinued structured and multiprofessional care within the hospital environement.1–3 Uncontrolled symptoms are among the most frequent causes for EV in cancer patients—a group that still constitute majority of patients receiving palliative care.4–6 Overall, between 17% and 50% of EVs of cancer patients are deemed avoidable.7–10 Strategies to anticipate and prevent rapid deterioration of health condition are needed. While intensive care is provided within the hospital environment, continuous monitoring and care in an outpatient setting often cannot be given due to lack of resources. Therefore, novel and innovative approaches are needed.
Utilization of smartphones and sensor-equipped devices gives the possibility to obtain objective patient-related parameters in an unobtrusive, continuous, and real-time manner. Mobile health technology has been explored in numerous diseases and patient groups, for example, in cardiovascular diseases, 11 hemodialysis patients, 12 chronic pain, 13 children with cerebral palsy, 14 stroke rehabilitation, 15 Parkinson, 16 and stressed persons. 17
Use of mobile health devices for patient-reported outcomes (PROs) has recently been implemented in oncological care.18–21 Basch et al. reported an overall survival benefit of five months in patients receiving chemotherapy for metastatic cancer. 21 However, research focusing on mobile health technology for health status monitoring of cancer patients is still in its early phase. The sparse investigations on this topic focus mostly on patients with curable disease. Ferriolli et al. could show a strong correlation of findings obtained by an accelerometer with daily physical and functional status, fatigue, and quality of life (QoL) in cancer patients at different disease stages. 22 The international scientific palliative care community therefore promotes the use of mobile health.23,24 However, data on use of these technologies in severely ill patients are very scarce, mostly because these patients are often considered too burdened, fragile, and too old to operate mobile devices or participate in a study using mobile health technology. 25
In this prospective observational study, we aimed to evaluate feasibility as well as patients' acceptance of remote monitoring using mobile health technologies in palliative patients with a limited life expectancy. We hypothesized that health monitoring by wearables can predict a decline of patients' health status.
Methods
Study design and participants
This prospective observational study was conducted at the University Hospital Zurich. The research protocol has been described previously 26 and approved by the local Ethics Committee (PB_2016-00895). All patients provided written informed consent.
Eligibility Criteria were age >18 years, presence of a severe medical condition (incurable cancer with an estimated life expectancy of >8 weeks to <12 months judged by a physician of the project team, severe cardiac disease with New York Heart Association (NYHA) III–IV symptoms or severe pulmonary disease having a chronic obstructive pulmonary disease (COPD) Global Initiative for Chronic Obstructive Lung Disease [GOLD] III–IV), performance status of Eastern Co-operative Oncology Group (ECOG) ≤2 or Karnofsky Performance Status (KPS) ≥50%, absence of relevant cognitive impairment, and good knowledge of German language. In addition, patients had to be able to handle the wearables, which was tested shortly. After instructions and a demonstration, patients were asked to put the bracelet on and off, to turn on and off the smartphone, charge the wearables, and answer the digital questionnaires on the smartphone.
We aimed to include 30 patients expecting discharge from inpatient care. The study was proposed to all eligible patients on the ward. All eligible patients were asked to complete a questionnaire on their experience with electronic devices. Patients, who refused to participate in the study, were asked about reasons for their decline.
Endpoints
The primary endpoint was feasibility of health monitoring in this patient group as well as patients' acceptance. In addition, we aimed to identify features predicting a deterioration of health status with subsequent unplanned rehospitalization, EV or death. Unplanned or emergency rehospitalizations or visits are subsequently referred to as EV.
Monitoring system with wearables
Patients were equipped with a smartphone Samsung Galaxy S5 and the bracelet Everion® (Biovotion AG®, Zurich, Switzerland), henceforth summarized under the term wearables. The sensor-equipped bracelet had to be worn on the upper arm. Use of patient's own Android smartphone was possible—in this case the application (app) “Active Monitoring” was installed. This app has been designed and adapted specifically for the needs of palliative care patients following a patient-centric approach involving user interviews. 27 Reliability tests were performed by laboratory members of Swiss Federal Institute of Technology (ETH) during the entire development. More than two months of data were collected, ensuring its flawless functionality. The app recorded motion sensor data (GPS, acceleration), phone call statistics (anonymized), and the features measured by the bracelet (Supplementary Table S1), which was automatically connected to the smartphone via Bluetooth Low Energy.
Encrypted data were sent once daily to a secured server located at ETH using Wi-Fi networks. In case of successful transmission, data were deleted from the phone. Sensitive data such as real location (GPS) were anonymized, and phone numbers as well as names were not recorded.
Procedures and symptom assessment during observational period
The observational study phase started at discharge from hospital and was planned for a maximum duration of 12 weeks. Patients were asked to wear the wearables as often as possible except for the time needed to charge battery.
QoL was assessed one day before discharge using European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC QLQ-C30), version 3.0, on a paper form. 28 During the outpatient period, patients were called once a week by a member of the study team and were asked the EORTC QLQ-C30 to have a regular symptom assessment. During this phone call, usability aspects of the wearables were evaluated additionally. Severity of common symptoms was evaluated one day before discharge using the Edmonton Symptom Assessment System (ESAS) on a paper form and at the end of the study during a phone call. Patients had to assess their pain and distress level at least once daily via a digital questionnaire using the Visual Analog Scale (VAS) on the app. The scale ranged from 0 (no symptom at all) to 10 (most severe symptom one could imagine).
Statistical analysis
Sensor raw signals were cleaned and preprocessed to extract features using Python 3.5.4 (64-bit), Pandas 0.23.0, NumPy 1.14.1, and scikit-learn 0.19.1. Statistical analysis was performed using R x64 3.5.1.
For quantitative variables, Shapiro–Wilk test was used to determine if parametric (Welch's t test) or nonparametric tests (Mann–Whitney U test) should be applied. For categorical variables, Fisher's exact test was applied. Reliability of the QLQ-C30 in our study cohort was evaluated by means of Cronbach's α. For all statistical analysis, p values <0.05 were considered as statistically significant.
To evaluate acceptance of activity monitoring by this patient group, usage time of wearables, patients' perceptions, and potential problems and barriers were analyzed using semiquantitative questionnaires during the study as well as qualitative interviews at the end of the observational phase.
For 80 features (Supplementary Tables S1 and S2) extracted from the mobile sensor raw signals, a Pearson's correlation analysis was performed to investigate the association between sensor measurements and QLQ-C30 scales as well as VAS ratings. Analyses were performed per patient, and we evaluated whether the same features show the same correlation in other patients as well; a cutoff value of |r| ≥ 0.3 was used. 29
A group comparison of patients with and without an EV was performed to test, if there is a feature predicting such an event. Figure 1 illustrates the time windows relevant for this analysis. For the same 80 features as used in the correlation analysis, trends were specified by the ratio of median values during the first week at home after discharge and median values during the last week before an EV or before study end for those patients without an EV, respectively. The same ratios were applied for values from the daily self-reports (pain and distress VAS) and the global health status scale (QL2) assessed by the QLQ-C30. For QL2, relevant changes were defined as decrease of at least 10% compared to the baseline value taken at hospital. For pain and distress VAS, relevant changes were defined as an increase of at least 2 points compared to the rating at the first day after discharge.

Time windows analyzed for group comparison. Trends were specified by the ratio of the median values of a feature during the first week at home after discharge (BL) and median values of a feature during the last week (EV) before an emergency visit
Results
Patients' acceptance
Between February 2017 and February 2018, 68 patients fulfilled study inclusion criteria, of which 31 (49%) consented to participate (Fig. 2). Only one patient otherwise eligible failed to pass the mini test on wearables handling. This patient was diagnosed with a glioblastoma. He had no difficulties to perform daily activities, but struggled with learning a new procedure. Median age of participants was 64 and all had a cancer diagnosis. No patient with severe cardiac or pulmonary disease fulfilled all criteria for study participation. One patient died only three days after discharge before any data were collected and was therefore only included in the analysis of demographic data. Eight patients were using walking aids, that is, crutches, or were sitting in a wheel chair.
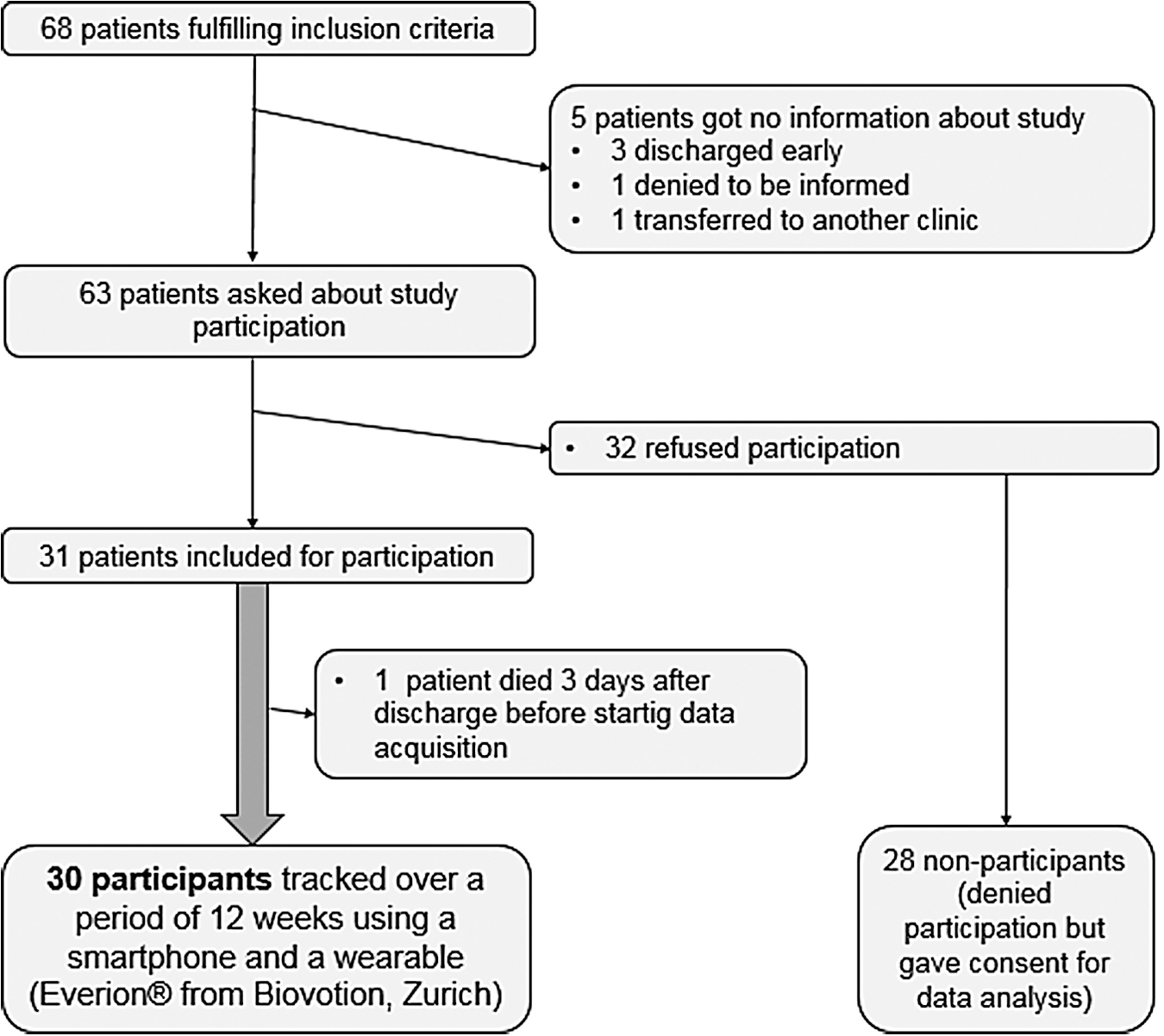
Study enrollment flow diagram. ECOG, Eastern Cooperative Oncology Group; EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30; ESAS, Edmonton Symptom Assessment System; GOLD, Global Initiative for Chronic Obstructive Lung Disease; KI, Karnofsky Index; NYHA, New York Heart Association; VAS, visual analog scale.
None of the patient characteristics, nor primary disease, performance status, or comorbidity status differed significantly between study participants and eligible nonparticipants (Table 1). The large majority (>90%) of screened patients had some experience with electronic devices, mostly personal computers and smartphones. Patients willing to participate more often had previous experience with a tablet and an interest in electronic devices compared to patients, who were eligible but refused to take part. In addition, participants had experience with a smartphone, tablet, or computer for a longer time (Supplementary Table S3).
Patient Demographics and Characteristics
CCI, Charlson Comorbidity Index; ECOG, Eastern Cooperative Oncology Group; IQR, interquartile range; KPS, Karnofsky Performance Status; SD, standard deviation.
Most frequently expressed reasons to refuse study participation were concerns regarding handling of devices being too cumbersome and the effort to complete questionnaires (Supplementary Table S4).
Feasibility of activity monitoring
Twenty-five patients participated for the full study duration of 12 weeks. Study dropouts were mostly due to health reasons; only two patients left the study early due to technical problems with Bluetooth connection between the smartphone and bracelet.
Feedback was mainly positive: 76% of participants stated that they appreciated the monitoring and would recommend it to other patients. Only 2 out of 30 (7%) patients criticized the comfort of wearing the bracelet.
All but two patients had no difficulties to handle the wearables and answer the daily questionnaires. Both patients had no experience with a smartphone before. One of them received strong support by the study team with several visits empowering her to use the smartphone and the app in the designated way. The other patient was the oldest study participant: a 85-year-old female reporting to be forgetful. She experienced difficulties to remember how to use the smartphone. Details on usability aspects and patients' perceptions will be reported in a separate publication. 46
Data completeness
On average, the bracelet was worn on 53% (standard deviation [SD] 28.0) and the smartphone on 85% (SD 19.4) of all study days. Digital questionnaires (pain and distress VAS) were answered on 73% (SD 22.8) of all days patients spent at home. On those days wearables were worn, patients were wearing the bracelet for 63% (SD 16.8), and the smartphone for 50% (SD 24.2) of time between 8 am and 8 pm (Supplementary Table S5). All retention rates remained stable over the study period (more details are shown in Supplementary Figs. S1–S3).
Weekly interviews were completed with an overall rate of 83%. One of the 30 patients was excluded from this analysis because his health status deteriorated such that he was unable to speak on the phone. Cognitive and social functioning scales and nausea and vomiting symptom scale were excluded from further analysis, as this EORTC-QLQ-C30 subscores were not reliable based on Cronbach's α.
Prediction of unplanned emergency readmission
Eleven patients (36.7%) had an EV event, which occurred on average 6.14 ± 3.64 weeks after discharge (Supplementary Table S6). Two of these patients returned for an EV while staying at a medical rehabilitation clinic. As behavioral features, recorded during medical rehabilitation, are not comparable to records at home due to a vigorous exercise schedule, we excluded these two events from the analysis of outcome prediction, but considered all data for data completeness evaluation. One patient experienced the EV in the first week after discharge, such that only insufficient baseline data were available leading to an exclusion from the analysis. One patient experienced four EVs. However, only the first was analyzed, since the data preceding successive events were not sufficient to build a new baseline.
On average, there was a moderate positive correlation between 43 of 80 mobile health features extracted from sensor signals and daily VAS ratings (r = 0.6, p < 0.0001). These features were found in 20 out of 30 patients; for the other 10 patients, the analysis did not show any significant results. Significant correlations with Pearson's |r| ≥ 0.3 for more than one patient are summarized in Supplementary Tables S7 and S8.
There was no significant correlation between mobile health features and the individual QLQ-C30 scores. None of the features extracted from patients' self-reports showed significant differences between the two groups (Supplementary Table S9).
Out of the 80 features extracted from sensor data, 3 were significantly correlated with an EV during the study period. Patients with an EV exhibited an increased resting heart rate (RHR), decreased heart rate variability, and a trend for increased step speed (Table 2).
Mobile Health Features and Their Ability to Predict an Emergency Visit/Unplanned Readmission
An overview of results on some of the features. Not all measured and tested features are displayed (for a comprehensive overview on all investigated features, see Supplementary Tables S1 and S2). All three mobile health features showing a significant difference between patients without readmission patients with readmission are shown here.
df, Degree of freedom; RHR, resting heart rate; RMSSD, root mean square of successive differences (a parameter of RHR variability); Step speed, the number of steps per second as measured with the smartphone; t, Welch's t test for unequal variances; W, test statistics for Wilcoxon rank-sum test.
Discussion
Our study demonstrates that continuous health monitoring using wearables was feasible over a period of 12 weeks in palliative cancer patients with a limited prognosis of <1 year. Wearables were accepted by 76% of patients. The only patient characteristic associated with motivation for participation was prior experience with electronic devices. Three mobile health features were identified as potential biomarker: resting heart rate variability (RHRV), RHR, and step speed. In contrast, patient-reported ratings of pain, distress, and QLQ-C30 scores were not associated with EV—indicating the potential value of physical activity monitoring on prediction of health status deterioration with subsequent EVs. Objective digital biomarkers might therefore complement PROs as a measurement to detect patients` health status deterioration and prevent readmissions.
In contrast to our trial, previous studies focused on interventions such as telephone follow-up, questionnaires or web-based apps for reporting of symptoms.30–33 Most mature data have been reported by Maudlin et al. Introduction of a combination of text messaging and videophones achieved a reduction of hospitalizations by 66% and of EVs by 19% in veteran patients with end-stage illnesses, including cancer, chronic heart failure, emphysema, or dementia. In contrast to our study, these patients had a better life expectancy of minimum two years. 34
Use of mobile health technologies to predict deterioration of cancer patients' health status was investigated by few studies. Most focused on mobile health devices providing only limited features, that is, pedometer or accelerometer mainly addressing step count.22,34,35 Consequently, most studies excluded patients in need of walking aids. In two independent investigations, a correlation among daily physical activity, functional status, and severity of symptoms was reported.22,36 In our study, step count did not predict a deterioration of health status and was not correlated with subjective symptom scores. This may be explained by inclusion of disabled patients using walking aids.37,38
Speed of steps was identified as a novel feature that significantly differed between the groups of patients with and without EVs. None of the afore mentioned studies investigated step speed as a mobile health biomarker. Gait velocity declines with age and is a predictor for mortality with slower walkers experiencing a worse survival in community-dwelling people aged >75. 39 Our results show significantly faster steps in patients with readmissions. We did not measure their gait velocity and we therefore hypothesize that higher speed of steps may be a surrogate for gait disorders. Further research is required to investigate this issue.
The other two predictive features are in line with existing literature: as a general health indicator, an increased RHR may be a sign for a worsened health condition. RHRV (root mean square of successive differences [RMSSD] value) showed a smaller ratio in the group of patients experiencing a readmission, which is in concordance with the literature. Mean RHRV for healthy adults is 42 mseconds, 40 whereas a study focusing on cancer patients found a reduced value of 24 mseconds in mean. 41 The authors of a systematic review conclude that RHRV seems to be a useful parameter to assess the general health condition of cancer patients 42 and several investigations showed an inverse correlation of RHRV and survival.43,44
Limitations of the study include the small sample size of 30 patients and heterogeneous patient features with respect to primary tumor, demographics, and comorbidities. Consequently, the small and diverse sample impeded identification of representative parameters for all patients. Furthermore, the few incidences of EV (1 per patient) did not allow for training of patient-specific models except of anomaly detection (e.g., one-class support vector machines). Hence, it was not possible to identify patterns that are specific for EV (i.e., that occur mainly/only before an EV). The study phase was limited to 12 weeks—therefore, it cannot be stated or predicted if patients would be able and willing to wear the devices for an extended period of time. Weekly phone calls could serve as a repetitive reminder to wear the devices and therefore compliance could be overestimated.
However, the study cohort reflects a real-world scenario with every single patient being distinct in terms of the above-mentioned parameters. Study design and inclusion criteria were adequate to test feasibility of the selected tracking procedure in the patient group we were interested in. One strength is the simultaneous acquisition of subjective and electronic longitudinal data in this patient group over a long period of time considering their short life expectancy. Moreover, we provide reasons for patient's refusal to use mobile technology, an important issue recently raised by others. 45
In conclusion, this study showed that use of mobile health technology is feasible and accepted by palliative patients in an ambulatory setting. Group comparison revealed three mobile health features significantly differentiating between patients with and without EVs. These mobile health biomarkers require further prospective validation, for example, in a follow-up study investigating the impact of an intervention—based on these novel predictive features—on patient outcomes.
Footnotes
Acknowledgments
We thank Debora Mittner and Sonja Schwenne for their valuable work and effort during data acquisition.
The only data so far presented are:
Research protocols: Theile G, Klaas V, Tröster G, Guckenberger M: mHealth technologies for palliative care patients at the interface of inpatient to outpatient care: Protocol of feasibility study aiming to early predict deterioration of patient's health status. JMIR Res Protoc 2017;6:e142.
Klaas VC, Calatroni A, Hardegger M, et al. (eds): Monitoring patients in ambulatory palliative care: A design for an observational study. In: Wireless Mobile Communication and Healthcare. Cham: Springer International Publishing, 2017, pp. 207–214.
Poster presentation: Poster presented at ESTRO 2019 in which the main findings of the study are described: Pavic M, Klaas V, Theile G, et al.: PO-0879: Mobile care for monitoring of health status in palliative care patients: A feasibility study.
Funding Information
The study was funded by the foundation program “Research in Palliative Care” of the Swiss Academy of Medical Sciences (SAMW) and the “Gottfried and Julia Bangerter-Rhyner Foundation” and “Stanley Thomas Johnson Foundation.”
Author Disclosure Statement
The authors declare no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.