
Abstract
Background:
Home care workers (HCWs)—including home health aides, personal care aides, and other direct care workers—provide functional and other essential support that allows older, disabled, and seriously ill people to live at home. As a growing number of patients are aging and dying at home, HCWs are increasingly providing care at the end of life (EOL). Although prior qualitative studies have shown that patient death is an impactful and challenging experience for HCWs, the majority of HCWs receive almost no training on EOL issues.
Objective:
The goal of this scoping review is to identify intervention studies describing training of HCWs in EOL issues to map types of training and to assess the degree to which existing efforts address HCW health and well-being.
Design:
Our scoping review covered three databases and focused on articles published in English since 2000.
Results:
Of the 393 articles screened, 26 underwent full-text review and 6 met inclusion criteria. Only one article discussed training designed for and implemented with HCWs exclusively. Other trainings simultaneously targeted multiple kinds of workers. Supporting HCWs in reducing their stress and improving their coping skills was substantially addressed in only one article, although HCWs' emotional needs were addressed less centrally in several others.
Conclusion:
Our findings suggest that there is a paucity of EOL training interventions tailored specifically to the experiences and positioning of HCWs. We recommend that future intervention studies address the multiple facets of HCWs' stress related to patient death to improve EOL care in the home.
Background
Home care workers (HCWs)—including home health aides, personal care aides, and other direct care workers—provide functional and other essential support that allows older, disabled, and seriously ill people to live at home. Currently there are an estimated 2.1 million HCWs working in the United States, and experts project a need for 600,000 additional home care jobs by 2024. 1 Importantly, as a growing number of patients are dying at home, HCWs will increasingly provide care at the end of life (EOL).
Patient death can be a powerful and problematic experience for HCWs, however. Research suggests that following patient death, HCWs may experience emotional grief symptoms similar to those of family members, as well as sleep disruptions and physical manifestations of stress.2,3 Compounding this are the isolated work environments in which they provide care; HCWs typically lack support from supervisors and coworkers.2,4,5 They may also experience financial and instrumental disruptions since the death of a patient may threaten an aide's work hours in the near term, impacting take-home pay and eligibility for health coverage and other benefits.2,6
Despite these challenges, HCWs in the United States currently receive little to no training in palliative and EOL care specifically. The need for improved training in palliative care for health professionals has been widely acknowledged, as has the sometimes enduring impact of deaths on providers themselves.7–9 The body of research addressing EOL training for nurses, in particular, is substantial.10–13 A recent review article found that EOL training programs have improved work stress, communication, attitudes, knowledge, and confidence of nurses in providing EOL care. 12 Without attention to developing training and support systems for HCWs who are some of the most marginalized paid caregivers, maintaining and growing a skilled supply of these workers will be challenging.
The goal in this review is to identify studies describing training of HCWs in EOL issues to map types of training and assess the degree to which existing efforts address HCW health and well-being. This article builds on two recent reviews of palliative care education among nursing home staff and among Canadian nurses and HCWs.12,13 While these reviews address largely institution-based workers who may have access to support and training on the job, our article focuses on HCWs specifically, given their unique positioning in relation to patient death, and adds an analysis of the degree to which aides' own health and well-being are addressed.
Methods
Given our goal of mapping types of training, we conducted a scoping review following PRISMA guidelines.14,15 We searched three relevant databases as follows: PubMed, CINAHL, and Sage Premier using predetermined search terms (Table 1). Inclusion criteria appear in Table 2. While we did include international studies, resource constraints dictated that we review only articles in English. Restricting studies to the last two decades ensures that training modalities and health care systems are approximately comparable to those of the present. Studies were excluded if they provided no direct material on training development, implementation, or evaluation. All search results were managed in the web-based systematic review software, Covidence.
Search Terms
Inclusion Criteria
EOL, end of life; HCW, home care worker.
We extracted data in the following areas: target population(s), training content, content devoted to aide health and well-being, program duration, evaluation methods, and evaluation results.
Results
After removing duplicates, we screened 393 articles, of which 26 underwent full-text review and 6 met inclusion criteria (Fig. 1).10,16–20 Two articles referred to supplemental articles that provided more detail on their trainings; we included these in our sample21,22 (See Table 3 for a summary of included articles).
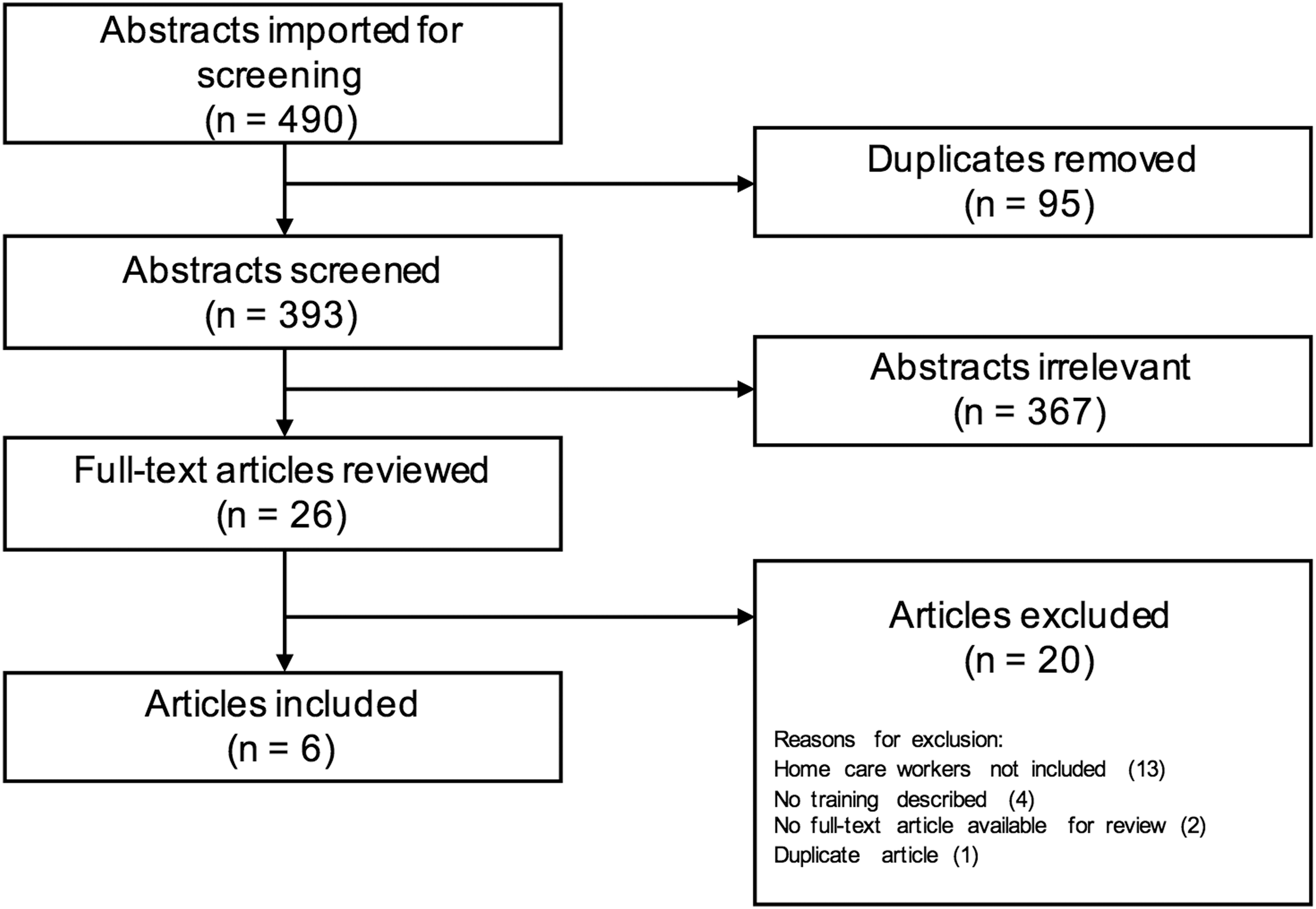
PRISMA flow diagram.
Characteristics of Included Studies
Substantial = training modules and/or program objectives address HCW health and well-being with significant description/discussion of these topics in article; Some = training modules and/or program objectives address HCW health and well-being but not discussed in article; Minimal = training modules may address HCW health and well-being but not discussed in article.
ECAT, Enhanced Care Assistant Training; ELNEC, End-of-Life Nursing Education Consortium.
Audiences for training
Of the six articles, only one discussed training designed for and implemented with HCWs exclusively. 16 Other training efforts targeted home health aides and home care nurses 17 and registered nurse and nursing assistant students trained in home settings. 20 One training was tailored to home- and community-based care workers. 19 Two trainings were developed for an even broader audience: nurses and nursing assistants (including home health aides), working in both home and institutional environments.10,18
Training content
Training content varied depending on the programs' aims and audiences. The program most tailored to HCWs was the Recognition, Respect, and Responsibility: Enhanced Care Assistant Training curriculum implemented in Virginia. 16 The curriculum aimed to increase empowerment, retention, and professionalism and included 4 seven-hour modules followed by 12 practicum hours. 21
Modules addressed were as follows: (1) improving communication and professionalism, (2) recognizing and meeting complex patient needs, (3) dealing with loss, death, and mourning (for patients, families, and workers), and (4) preventing and reducing burnout. The program was delivered through video with an in-person facilitator present. The extensive EOL material addressed, among other topics, ways workers could “help themselves and others cope with death.”16(p.315) Modules 3 and 4 addressed coping skills relevant to managing stress stemming from patient death.
Two other efforts included HCWs as trainees18,22 and were based on the End-of-Life Nursing Education Consortium (ELNEC) curriculum, a train-the-trainer program developed in the early 2000s. 10 These two programs each tailored the core ELNEC curriculum, which involves nine training modules: (1) Palliative nursing care, (2) Pain management, (3) Symptom management, (4) Ethical issues, (5) Cultural considerations in palliative care, (6) Communication, (7) Loss, grief, and bereavement, (8) Achieving quality palliative care, and (9) Preparation for and care at the time of death. 10
Both efforts sought to train nurses and nursing assistants (some of whom were home health aides), but only one, which was based in California, tailored materials for nursing assistants specifically, including addressing their grief. 22 The other, based in New England, altered the topics slightly, adding modules on advanced directives and dementia and removing the session on loss, grief, and bereavement. 18
Similar topics were covered in a program for nurses and home health aides based at home health agencies in Southern California. 15 In this program, 5 three-hour modules covered: (1) Palliative care and EOL issues, (2) Pain management, (3) Symptom management, (4) Communication, spirituality, and family caregivers, and (5) the “good death.” While aide health and well-being does not appear to be a strong priority of this curriculum, some aspects of the communication and “good death” modules (e.g., “interventions for grief and self-care”) may be relevant. 17
The final two studies took place outside of the United States and used substantially different approaches. One study from rural Canada involved two days of training, followed by a practicum for registered nurse and nursing assistant students to improve their ability to care for those living at home with advanced chronic illness. 20 While this training did address EOL, it did not devote a specific module to it nor did the training address health and well-being of would-be HCWs specifically. A second study trained home and community-based care workers in South Africa caring for very sick children at home. 19 A three-day pilot of this train-the-trainer effort covered pediatric palliative care and ways of supporting family caregivers caring for HIV-infected children. One additional goal was supporting workers “to care for themselves.” 19
Evaluation methods and results
All studies discussed basic evaluation efforts, although no rigorous designs testing effects of training on HCW health and well-being were reported. Evaluations focused on assessing outcomes of program satisfaction, 21 perceptions of training,18,21 knowledge,17,18 perceptions of competence, 20 and number of people trained,10,22 using both quantitative and qualitative approaches. Programs were generally well received, and a few demonstrated increased knowledge and perceived competence in several areas. Notably, one study did not include HCW participants in their knowledge assessment, 17 and another evaluation found a high attrition rate among HCWs and other health care assistants. 18
Discussion and Conclusion
Our review indicates that, despite HCWs' frequent exposure to EOL issues, there are few studies documenting interventions designed to improve their training and preparedness in this area. Of the programs identified, only one 16 was specific to HCWs and many trainings targeted multiple kinds of workers simultaneously. Evaluations of these programs were limited and did not address HCW health and well-being. The circumstances and needs of HCWs are unique when it comes to patient death; therefore, trainings should explicitly address their positioning and experiences. For example, to our knowledge none of the trainings directly acknowledge the job insecurity associated with patient death for many HCWs in the United States, which recent studies suggest is an important component of the stress associated with patient death.2,5
Supporting HCWs in reducing their stress and improving their coping was substantially addressed in only one article, 16 although HCWs' emotional needs were addressed less centrally in several others.17,19,22 For HCWs, job-related stress impacts job satisfaction and turnover. 23 Turnover among HCWs in the United States is exceptionally high, with estimates ranging from 25% to 200% annually.24–26 This is a critical issue given the rapidly expanding need for HCWs. HCWs themselves have identified relevant support mechanisms like additional training in EOL issues, greater support from employer agency staff, and greater availability of paid time off,2,5 which should be addressed in future research.
In conclusion, we found a paucity of studies that address the EOL training needs of HCWs specifically. We recommend that future intervention studies develop and rigorously evaluate programs that address the multiple facets of HCWs' stress related to patient death. This will help enable this workforce to grow and thrive, while providing essential EOL care in the home.
Footnotes
Acknowledgments
The authors are grateful for feedback on an earlier version of this work received at the American Public Health Association Annual Meeting, Occupational Health and Safety Section in 2018. Thanks also to Emily Pagano for her assistance in developing the search strategy.
Funding Information
No funding was received to support the development of this article.
Author Disclosure Statement
No competing financial interests exist.