
Abstract
Background:
As the number of geriatric trauma patients rises, end-of-life planning is of increased importance. A community-wide initiative to increase advance care planning was undertaken in the 1990s, resulting in a high rate (85%) of completed advance directives (ADs).
Objectives:
To assess the impact of ADs on quality measures of care and outcomes for elderly trauma patients. To determine if the historically high rate of completed ADs in the community applied to the trauma patient population.
Design:
A single trauma center's registry was retrospectively reviewed. Patients with versus without an AD were compared. A case–control analysis was completed. Statistical analysis included chi-square test, Wilcoxon rank sum, and multivariate linear regression modeling.
Setting:
American College of Surgeons-verified level II trauma center with a 325-bed teaching hospital.
Subjects:
Patients ≥55 years admitted as level I or II activations from January 2007 through April 2017.
Measurements:
Hospital and intensive care unit (ICU) length of stay (LOS), ventilator days, and 30-day mortality.
Results:
Nine hundred thirty-six patients were identified; 173 (18%) had an AD and 763 (82%) did not. ADs were more common among older, female patients. The majority of patients with ADs lived within the medical center's service area (99% vs. 1%) and had a primary care provider within the health care system (72% vs. 28%). Although 30-day mortality was higher in patients with ADs versus without (21% vs. 15%; p = 0.03), this difference was not significant on case–control analysis (20% vs. 15%, p = 0.31). No difference was identified in LOS, ICU days, ventilator days, or charges.
Conclusions:
Presence of an AD was not associated with any difference in 30-day mortality, LOS, or hospital charges. More widespread efforts at AD education and documentation are necessary, particularly in the setting of trauma.
Introduction
There has been increasing emphasis on the role of advance directives (ADs) in providing high-quality, economic, and compassionate care to patients at the end of life. The Patient Self-Determination Act of 1990 required health care systems to provide patients with information about their right to make ADs. 1 In response, the La Crosse, WI area health systems undertook an initiative to increase the education of adult patients about ADs in health care choices. The system trained more than 120 nonphysician educators to provide counseling and informational materials to patients pertaining to end-of-life planning. This included implementing practices and policies for documentation of ADs in patient medical charts. Before the initiative, only 15% of patients surveyed in the La Crosse area reported having written ADs. After the initiative had been in place for two years, 85% of adults who died in La Crosse County had an AD. Eighty-one percent of AD documents were accessible in the medical record and treatment decisions were honored in 98% of patients. 2
The proportion of the U.S. population 65 years of age and older continues to rise, currently at 13% and expected to be greater than 20% in 2020. This exponential rise of an aging population correlates with the increasing volume of geriatric patients admitted to U.S. trauma centers, a 30% acute increase from 2003 to 2009. 3 Previous studies have also shown increased mortality in elderly trauma patients.4,5 The rate of executed ADs in trauma patients has been highly variable, ranging from 4% to 24%.6–9 As Cocanour discussed in her Western Trauma Association presidential address, these changing times call for increased emphasis on end-of-life planning in trauma patients. 10 Trauma happens unexpectedly, frequently well away from home. Family members are often not present or are also injured, and therefore unavailable for advice regarding difficult care decisions. Presence of an AD allows patient wishes to be known, which can make respectful treatment decisions easier when the patient and family are unable to participate.
The study objective was to assess the impact of ADs on hospital charges and outcomes for elderly trauma patients. It was hypothesized that elderly trauma patients with an active AD experience an increase in overall mortality and that the community-wide AD initiative altered the quality and cost of care provided for elderly trauma patients. A secondary objective was to assess if the historically high rate of completed ADs in the broader community would be similar in the trauma patient population.
Methods
The trauma center included in this study has been verified as a level II trauma center by the American College of Surgeons (ACS) and includes a 325-bed teaching hospital that provides care to patients in a 19-county, 3-state region with a population >500,000. An ACS-verified level I trauma center has the resources to care for all trauma patients. A level I facility is a regional tertiary trauma center, where level II centers are often in a more rural environment, but are expected to be clinically equivalent to the level I trauma centers. 11 As part of the Wisconsin statewide trauma system, this is the designated resource trauma center for the large, southwest region; trauma patients are frequently evaluated and stabilized in small, rural hospitals before transfer to La Crosse. In 2017, the trauma center evaluated ∼800 trauma admissions, including 14% high acuity level I and 25% moderate acuity level II activations. Level I and II activations are based on patient clinical status and used as triage to determine trauma center resources needed. Level I activations represent critical trauma patients in extremis. Level II activations represent patients who have the potential to become unstable. 11
After obtaining Institutional Review Board approval, a retrospective review of the center's trauma registry was completed. Eligible patients were identified as level I or II activations from January 1, 2007, through April 30, 2017. Of those patients, all trauma patients older than 55 years with and without an AD known at presentation or noted within 24 hours of admission were identified. Patients were stratified by their county of residence and affiliation of their primary care provider to assess for the impact of the regional AD initiative. The service area was defined as zip codes within 80 miles of the trauma center.
Overall comparison of patients with an active AD versus no AD
Patients who had an AD on file were compared to those without an AD to determine any significant difference in age, injury severity score (ISS), Glasgow Coma Scale (GCS), hospital and intensive care unit (ICU) length of stay (LOS), ventilator days, and mortality. Total hospital charges were evaluated for those with versus without an AD.
Case–control matched analysis
A case–control analysis was then performed to account for any potential confounding factors based on patient characteristics and injury severity. Patients with an AD were matched 1:1 with patients who had no AD, based on age (within five years), sex, and ISS (within two points). Eleven patients with an AD could not be matched with a suitable control due to the specific criteria chosen. Therefore, 162 patients with an AD were compared with 162 matched patients without an AD. The outcomes compared included the following: 30-day mortality, hospital LOS, ICU LOS, ventilator days, and cause of death.
Statistical analysis
For both the overall comparison of patients with versus without an AD, and for the case–control analysis, the chi square and Fisher's exact tests were utilized for comparison of categorical data between groups, while the Wilcoxon rank sum test was utilized for comparison of ordinal and continuous data. A p-value of <0.05 was considered significant. The overall patient population was used to develop three separate multivariate linear regression models to assess the impact of AD on (1) hospital LOS, (2) ICU LOS, and (3) ventilator days after controlling for patient age.
Results
Overall comparison between patients with an active AD versus no AD
Overall, 936 level I or II elderly trauma patients were admitted during the study period. Mechanisms of injury involved blunt trauma in 94% of cases. Level I activations comprised 40% of all activations. One hundred seventy-three (18%) patients were identified to have an active AD, either on admission or within 24 hours, and 763 (82%) patients had no documented AD. Patients with ADs were more likely to live within the service area (99% vs. 1%) versus those without ADs (85% vs. 15%) (p < 0.001). Patients with ADs were also more likely to have a primary care provider within the health care system (72% vs. 28%) versus those without ADs (37% vs. 63%) (p < 0.001). The percentage of patients with an AD was inversely related to the distance from their home to the trauma center (Fig. 1). Patients with an AD were older and were more likely to be female compared to those without an AD (Table 1). Although patients with an AD present were more likely to request do-not-resuscitate (DNR) or DNR/do not intubate, full code status (all resuscitation procedures provided) was designated by the majority of patients (78%, n = 670), regardless of whether they did or did not have an AD on file (Fig. 2).
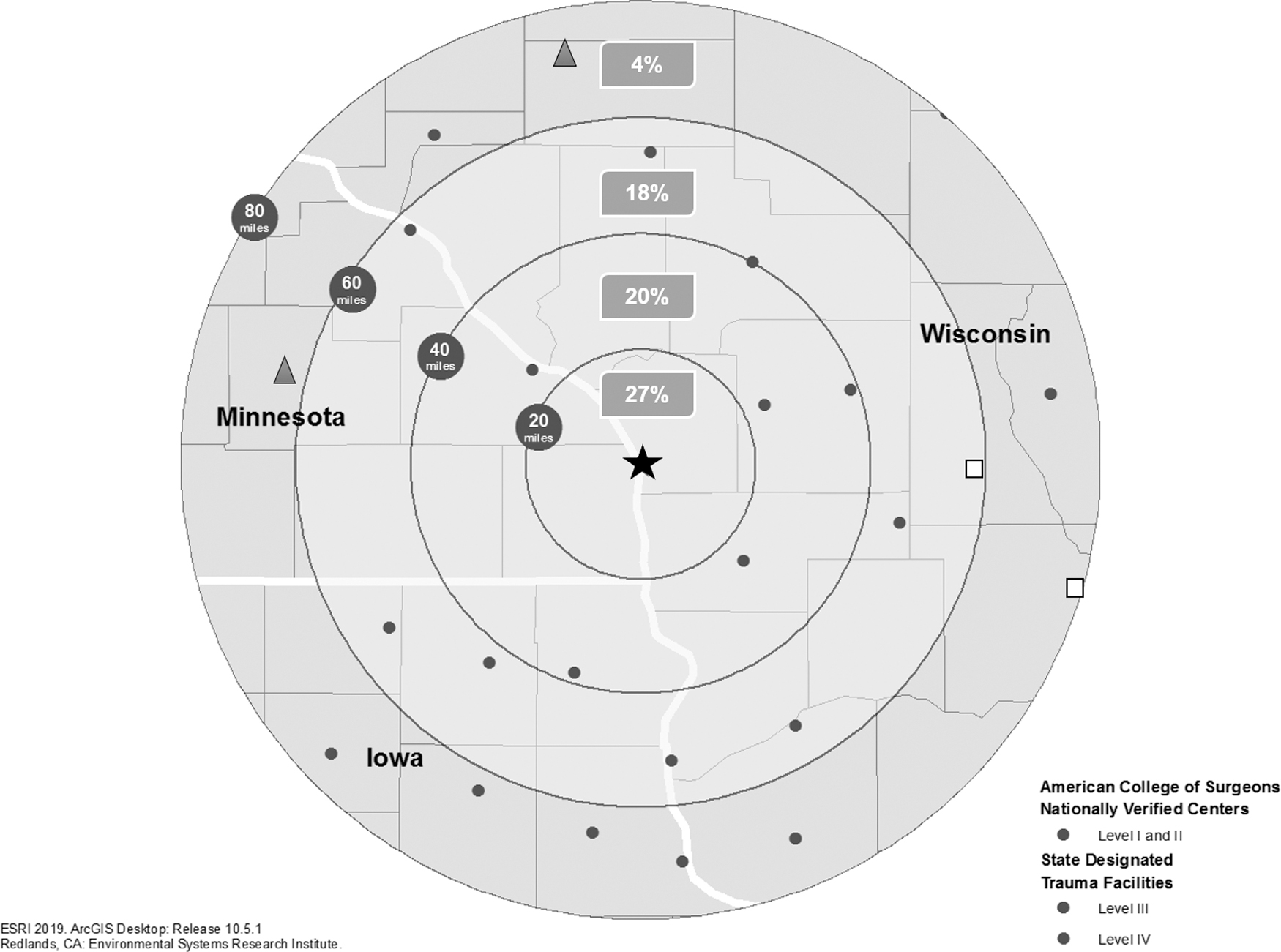
Percentage of patients, overall, with an AD based on distance from trauma center. AD, advance directive.
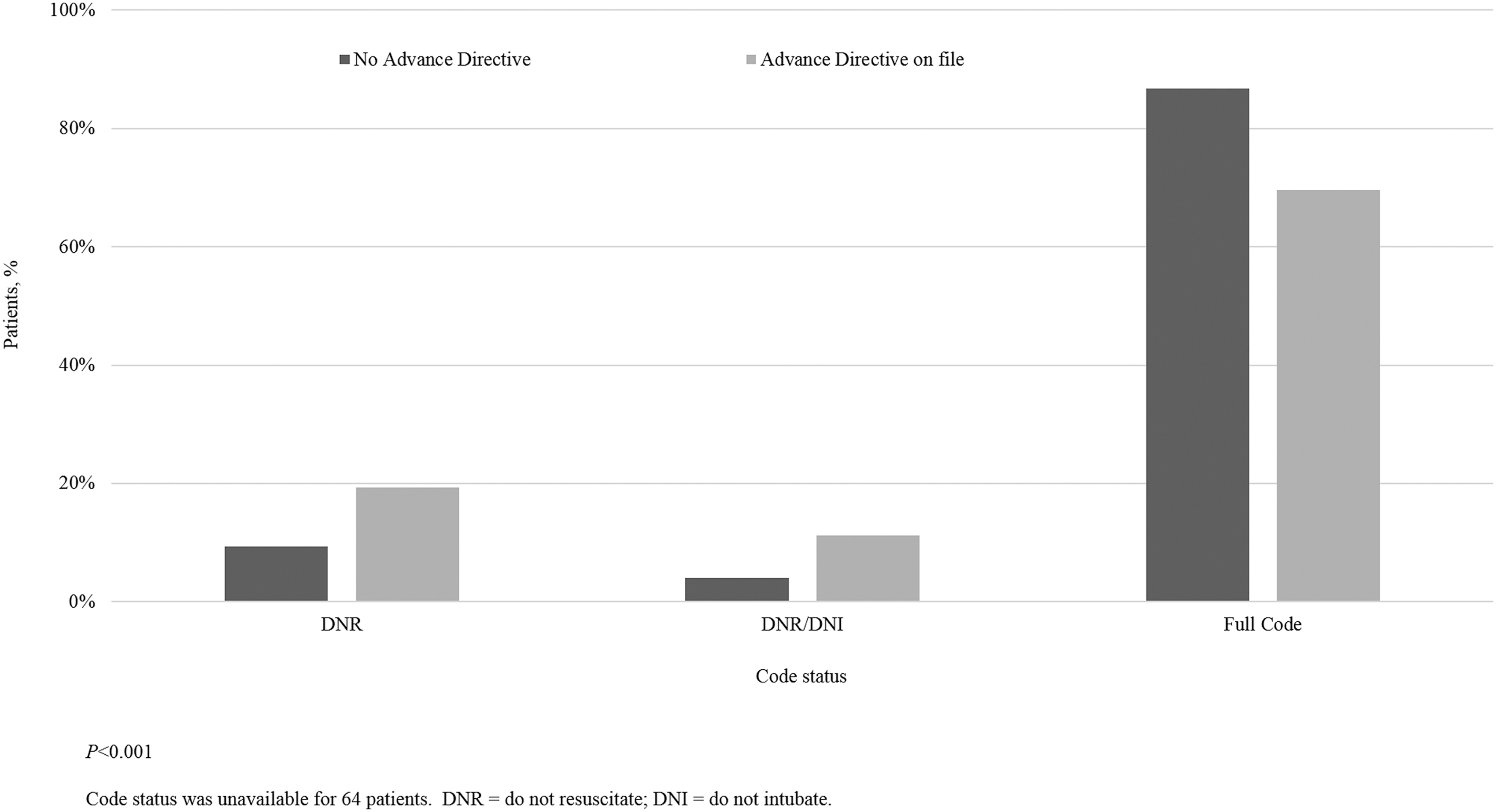
Code status based on presence of advance directive on file for the overall study population. DNI, do not intubate; DNR, do-not-resuscitate; Full Code, all resuscitative procedures provided.
Overall Patient Characteristics and Outcomes for Those with an Advance Directive Present versus Those without an Advance Directive Present on Admission
AD, advance directive; GCS, Glasgow Coma Scale; ICU, intensive care unit; ISS, injury severity score; LOS, length of stay; SD, standard deviation; USD, U.S. dollars.
The 30-day mortality rate was higher in patients with ADs versus those without ADs (21% vs. 15% p = 0.03). The cause of 30-day mortality was available for 139 out of 149 patients who died within 30 days of admission. Among those with an AD versus without an AD, the cause of death was neurologic in 57% versus 50%, cardiac in 8% versus 20%, respiratory in 3% versus 4%, and other in 32% versus 26%, respectively (p = 0.42). Overall hospital charges were similar for patients with an AD versus those without AD on file (Table 1).
In a multivariate linear regression model, after controlling for the effects of patient age, there were no significant associations between the presence of an AD and hospital LOS, ICU days, or ventilator days among the overall patient population (Table 2).
Multivariate Linear Regression Models to Assess the Effect of an Advance Directive Present versus No Advance Directive
Data were generated from three separate models, adjusted for patient age, for each of the three variables listed.
CI, confidence interval.
Case–control matched analysis
The case–control matched analysis included 162 patients in the cohort of patients with an AD and 162 patients without an AD documented. No significant differences were observed for GCS, code status, hospital LOS, ICU LOS, or ventilator days (Table 3). Thirty-day mortality rates were similar for those with versus without an AD in the matched analysis (20% vs. 15%; p = 0.31). The cause of mortality was available for 56 of 57 patients who died within 30 days of admission and were included in the matched cohort analysis. The causes of death in the AD group and no AD group were neurologic in 59% and 46%, cardiac in 9% and 21%, respiratory in 3% and 4% and other in 28% and 29%, respectively (p = 0.62).
Case–Control Analysis for 162 Patients with an Advance Directive Compared to 162 Matched Patients without an Advance Directive at the Time of Admission
Match criteria; patients were matched 1:1 based on age within five years, sex, and ISS within two points. Eleven patients with an AD were not able to be matched to a control.
Discussion
Only 18% of the elderly trauma population had ADs available at the time of admission, which is similar to percentages seen in previous studies.6–9,12 The prevalence of active ADs for patients who lived within 20 miles of the trauma center was only 27%. This was much lower than the 85% prevalence reported in the 1998 La Crosse community initiative. The difference is likely due to vastly different patient populations, as the majority of patients reviewed in the original study had a chronic illness or terminal disease and almost half of the patients died in a long-term care facility. 2 Trauma occurs unexpectedly and often involves otherwise healthy individuals who may not have felt the need to complete an AD. Trauma frequently occurs at a distance from one's hometown; trauma patients are often admitted to a distant regional trauma center in which they have never been treated before. There may be no familiar provider and no established medical record available for review. Family members are often not present or are also injured and therefore unavailable for advice regarding difficult care decisions. Presence of an AD allows patient wishes to be known, which can make respectful treatment decisions easier when the patient and family are unable to participate.
Older, female patients were more likely to have available ADs when making treatment decisions. It is likely that the La Crosse “Respecting Choices” initiative influenced the study population as evidenced by the fact that the number of patients having an AD was inversely proportional to the distance from their home to the trauma center and 72% of patients with a completed AD had a primary care provider within the health care system. A consistent difficulty that the trauma teams encountered was the inability to access medical records outside of the regional health care system in a search for a potential AD. Electronic medical records (EMRs) from an outside provider's office or local hospital in which a trauma patient may have received care were difficult to access in a timely manner. Also, it was a rare patient who traveled with a copy of their current AD. Solutions to this problem must involve a nationwide initiative to standardize the way in which ADs are completed and entered into EMRs, which are interactive across all health care systems.
As the population of the United States continues to age and with it the trauma population, it is important that advance care planning is integrated into the discussions with patients. There have been national proposals such as the Patient Self-Determination Act aimed at improving AD completion. Unfortunately, studies have shown few increases in documented ADs when they are needed most to guide patient care.13–16 Nkomo et al. found that even when ADs were available at hospital admission, they were often incomplete in guiding treatment decisions. 17 Wooster et al. noted that ISS was the only predictor of withdrawal of care in patients with geriatric trauma. 18 Furthermore, data have shown that the presence of a named health care agent is different based on race or ethnicity. 19
Despite regional efforts at AD education in the health system studied, this did not translate into a large number of active ADs upon admission to the trauma center for many of the aforementioned reasons. Nationally, the Physician Orders for Life-Sustaining Treatment (POLST) initiative has provided a method to improve discussions with patients once they arrive at trauma centers. It has allowed for a standardized, transferrable form to record patient wishes. Studies have shown that implementation of POLST has been effective. 20 Of course, the obvious limitation of this initiative is that it depends upon an awake, alert patient who can cogently voice their wishes. In the absence of an existing AD, POLST has been found to be an effective tool for this select set of trauma patients.
As more standardized forms and methods for documenting ADs are developed, it seems only natural to integrate these into EMR systems. Incorporating template-style notes and orders into the EMR workflow has improved provider discussions and implementation of preferred end-of-life treatment. 21 There are also positive reviews of patient-directed EMR integration with patient portal-based AD planning tools. 22 At this time, few EMRs are integrated across different hospital systems nationally, hindering easy passage of patient AD information. This is clearly an area for improvement as EMRs expand nationally.
The hypothesis of this study was that elderly trauma patients with an active AD would have an increased 30-day mortality rate and decreased hospital LOS, ICU LOS, and hospital charges. Although the overall group of patients with an AD had a higher 30-day mortality rate than the group with no AD, this difference was not evident when patients were matched by age, sex, and ISS. The effect of age on increased mortality has been shown previously when looking at timing of and the decision for withdrawal of care in trauma and ICU patients.23–25 Also, contrary to the hypothesis, presence of an AD did not otherwise significantly influence hospital outcomes such as hospital LOS, ventilator, or ICU days. This may be due to the majority of study patients with ADs indicating wishes to be fully resuscitated. Interestingly, McCredie et al. found that despite some institutions withdrawing care of patients with severe traumatic brain injury early, there was no difference in the aggressiveness of the care provided until the time of withdrawal. 23 Similarly, Street et al. observed that decisions of care in the emergency department did not appear to be influenced by the presence or absence of an AD. 12 These results suggest that acute care of elderly trauma patients may be comparable with or without an AD.
No difference in total hospital charges between elderly trauma patients with an AD and those without an AD was identified. Although charges and cost are not equivalent, resource allocation is becoming an increasingly important consideration when caring for trauma patients with a poor prognosis. It has been shown that in severely injured patients with a high probability of death, it might require treatment of 20 patients to save 1 life. This would come at the significant cost of greater than $700,000. 26 It is important to note that this represents only inpatient cost and does not reflect continued out-of-hospital care. As Kozar et al. identified, elderly trauma patients frequently require discharge to skilled nursing and long-term care facilities, which would increase the out-of-hospital cost to patients, families, and society. 3
It is important to emphasize that activation of an AD does not equate to patient desire to forego treatment, withdraw care, or undergo less aggressive treatment unless specifically stated for carefully defined situations. The AD process allows for a discussion of precisely what a patient would wish for medical decision making, given a specific set of circumstances in the event that they are unable to voice those wishes. It also promotes discussion of the “what ifs” with family and providers and may formalize the process of designation of a Power of Attorney for medical decision making. The fact that 70% of elderly trauma patients in this series with an active AD actually specified that they desired full resuscitation reinforces the concept that healthy patients who activate an AD may dictate that they desire aggressive treatment until such treatment may be considered futile, and only then would further treatments be withheld or withdrawn. For some patients, reticence to complete an AD has revolved around the concern that they might not receive appropriately aggressive treatment if they have an AD in force. The results of this study clearly support the conclusion that for elderly trauma patients, acute care as measured by 30-day mortality, hospital LOS, ICU LOS, ventilator days, and hospital charges was not different for patients with and without an AD.
There are a several limitations of this study. First, this was a retrospective review of a single institution's trauma database, which relied on the accuracy and completeness of the registrar. Because only 18% of patients had an AD on file at the time of admission, the sample size for some statistical comparisons was small, which could have led to the inability to show differences in the comparison groups even if they existed, that is, potential for a type 2 statistical error. The level II trauma center studied is part of a health system with an integrated EMR that includes 29 regional medical clinics and 5 regional hospital clinics across 3 states. However, due to the transient nature of trauma populations and the size of the referral area with many nonintegrated health care systems, it was difficult to reliably confirm preexisting ADs from nonaffiliated health care facilities. Finally, the trauma registry did not have the capacity to gain qualitative information on trauma patients. Therefore, it was not possible to quantify success in following patient wishes or how that affected the family or caregivers when making difficult decisions at the end of life.
Conclusion
Only 18% of elderly trauma patients had an active AD when admitted to the trauma center. Patients most likely to have an AD were older, female and lived near and/or received care in the same health care system. There were no differences in 30-day mortality, LOS, ICU LOS, ventilator days, or hospital charges when comparing matched patients with and without an AD. Future research addressing the process and timing for end-of-life decision making and the ability to meet patients' and family wishes with or without the presence of an AD in the trauma setting is needed. More widespread efforts at both AD education and standardized methods of AD recording are clearly necessary to help trauma teams identify patient choices in this transient population.
Footnotes
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.