
Abstract
Background:
Palliative care social workers (PCSWs) play a crucial role in optimizing communication and family-centered care for seriously ill patients. However, PCSWs often struggle to demonstrate and receive open acknowledgment of their essential skill set within medical teams.
Objective:
This case discussion focuses on the care of patients and families surrounding family meetings to highlight the crucial role of the PCSW in (1) preparing the family; (2) participating in the provider meeting; (3) participating in the family meeting; and (4) following up after the meeting. The aim is to illuminate how the PCSWs can demonstrate their unique and essential skill set to medical teams and as a means of furthering the work of psychosocial clinicians throughout medical systems.
Conclusion:
As the medical model continues to shift toward family-centered care, it is crucial for medical teams to optimize their partnership with patients and families. PCSWs can offer a trauma-informed biopsychosocial–spiritual lens that is instructed by continuity of care and exemplary clinical and rapport-building skills. PCSWs can play a critical role in optimizing communication, support, collaboration, and family-centered whole-person care.
Introduction
The unique skills of a palliative care social worker (PCSW) are well defined in the literature and include a biopsychosocial–spiritual assessment; strength-based therapeutic models; family-centered care; a trauma-informed approach to communication, care coordination, translation, and clarification of medical jargon; and anticipatory guidance around disease progression, end of life, and bereavement.1–5 PCSWs often struggle to articulate and navigate their role within medical teams. One way to highlight the distinct and essential role of PCSWs is in preparing for, participating in, and enhancing family meetings. 6 This case discussion aims to emphasize the nuanced, yet critical, role that PCSWs can play in optimizing patient and family-centered care—particularly when medical decision making, communication, and family dynamics are complex.1,5 Through role modeling during family meetings, the PCSW can also aid in creating visible and distinct roles for psychosocial clinicians more broadly within the medical system.
This case discussion highlights the PCSW role during four specific phases of a family meeting: (1) preparing the family; (2) participating in the provider meeting; (3) participating in the family meeting; and (4) following up after the meeting. Throughout this article, the term provider meeting is used to describe a meeting consisting of only interdisciplinary providers, which typically occurs before a family meeting.
Case: Setting the Scene
Nathaniel was a 15-year-old male with Duchenne muscular dystrophy (DMD), who presented with advancing cardiac involvement of his disease, requiring ventilatory support. His parents were married and had two other living children and an older son, Richard, with DMD who had died three years earlier. Nathaniel's physical, emotional, and existential suffering greatly impacted his entire family. His parents often described Nathaniel as “shutdown,” refusing to interact. When he did communicate through his assistive devices, he expressed anger and voiced a sense of injustice toward his limitations. Nathaniel's parents carefully included him in decisions related to mobility and quality of life, but they tried to protect him from information about his death as they were afraid this information would increase his suffering.
The paramount role of the PCSW was to hold Nathaniel's story at the forefront, which required building rapport with Nathaniel and his parents and frequent assessment of the family's state of processing. The PCSW reminded the team of the family's nuanced goals of care, highlighting their desire to balance the quality and quantity of Nathaniel's life.
Phase 1: Preparing the Family
The PCSW can play a crucial role in preparing the family for a family meeting, offering anticipatory guidance about what to expect during the meeting, and ensuring a clear understanding of the patient's and family's goals. PCSWs can help families to determine which providers and family members should be present, as well as optimal timing and location for the meeting. PCSWs often have longitudinal relationships with patients and families and therefore are uniquely positioned to build rapport and trust. This aids provider understanding of individual patient's and family's perceptions about quality of life that are imperative in driving the plan of care and in optimizing communication.7,8 Interdisciplinary presence throughout the patient's care over time is key to formulating a care plan that is consistent with whole-person care and that integrates all relevant medical and psychosocial factors.9,10
Case: What Was the PCSW Role in Preparing the Family?
Nathaniel's parents expressed a desire to meet with his medical team to discuss the plan of care as it had become evident to them that Nathaniel's body was too sick to be weaned from ventilatory support. The PCSW met with Nathaniel's parents to understand their perspectives and questions. The PCSW coordinated with the child life specialist to meet with Nathaniel to elicit his personal priorities. Nathaniel expressed his goal to go home, explaining that he was more comfortable in his own bedroom and that he missed his dogs. The PCSW inquired about how Nathaniel would like to receive information and he explained that he did not wish to be a part of the meeting, but that he would like his parents to provide him with an update afterward.
The PCSW learned from the chaplain that Nathaniel's parents had been processing the role of God in Nathaniel's care and were asking whether it was against God's plan to continue to intervene. The PCSW shared a summary of these conversations with Nathaniel's primary teams and vocalized the parents' requests that the meeting be limited to familiar team members, including Nathaniel's primary pulmonologist.
Phase 2: Participating in the Provider Meeting
PCSWs are experts in understanding how individual families function and cope with serious illness and do this through assessment of their daily routine, education level, medical literacy, access to resources, and overall support.5,6,10 These factors are critical—particularly during the provider meeting as medical teams consider how to approach each unique family. Due to their ongoing relationships, PCSWs can offer continuity and perspective regarding past conversations, meetings, and previously proposed care plans.
Given that social workers are trained in communication optimization, psychosocial considerations, and risk management, PCSWs can give suggestions for how to interact optimally with individual family members. 5 PCSWs can also offer awareness of biases and assist in identifying sources of provocation or sensitivity that may result in retraumatization or distress, which can be particularly helpful for individuals with a trauma history or other mental health considerations. Approaching sensitive topics, such as end-of-life conversations, with a trauma-informed lens is crucial as experiencing the serious illness or death of a loved one can be a life-altering hardship, particularly for those who have experienced previous losses and/or have maladaptive emotional regulation. Additionally, there may be instances when the PCSW may recommend against holding a family meeting as for some patients and families, a smaller conversation may be more therapeutic.
Case: What Information and Guidance Did the PCSW Offer During the Provider Meeting?
The PCSW presented a list of the family's questions, including their hope to speak with Nathaniel's pulmonologist about whether it seemed possible to wean him off the ventilatory support to return home for some period of time. The family wished to speak to the palliative care and cardiology teams about symptom management, explaining that Richard had reported a lot of pain at the end of his life and memories of his air hunger frequently replayed in his mother's dreams. The PCSW reminded the team that Richard's death anniversary was the following week and that the parents were upset by discussions about the end-of-life location. The PCSW articulated Nathaniel's update preferences.
Phase 3: Participating in the Family Meeting
The PCSW can ensure that introductions and a supportive meeting agenda are made at the start of family meetings. The PCSW can clarify medical jargon and offer a nonmedical perspective during the meeting to ensure that patients and families are hearing the intended message and that providers are tending to verbal and nonverbal communication from family members. This is important because breakdowns in communication can lead to distrust, moral distress, and poor bereavement outcomes.11,12 While medical providers traditionally acquire communication skills through informal education, PCSWs are taught how to optimize communication with patients as part of their formal training.8,13 PCSWs can also help to bridge communication when conflict or tension arises between family members or between the team and family. 14 Finally, PCSWs can offer a supportive presence and ensure that patients and families have a safe space to pause and process the information being shared so that they have a chance to voice their understanding and perspectives.
Case: How Did the PCSW Support the Family and Team During the Family Meeting?
Nathaniel's parents presented as tearful and nervous. The PCSW sat next to Nathaniel's parents and began by acknowledging Richard's upcoming death anniversary.
The PCSW offered an opportunity for each provider to present their name and role in Nathaniel's care. The PCSW suggested space for silence and reflection following significant portions of information, offering a chance for Nathaniel's parents to ask questions after each subspecialist finished their respective update. The PCSW reframed the medical team's concerns about the gravity of Nathaniel's clinical state as well as his parent's subtle acknowledgments that Nathaniel was nearing the end of his life. This allowed the providers space to hone in on the parents' prognostic awareness and openness to discussions about end of life.
As Nathaniel's parents became increasingly emotional, the PCSW offered to pause the meeting and resume the conversation at a later time. His parents expressed appreciation for the opportunity to absorb the information and discuss the options with their family before making further decisions. The PCSW worked with the medical team and parents to formulate a plan for what information they wished to communicate to Nathaniel and his siblings, including what language was familiar to their family.
Phase 4: After the Meeting
PCSWs can collaborate with the primary social workers and other psychosocial providers to determine how to delineate supportive roles and tasks. PCSWs can aid the family in voicing lingering questions regarding medical treatment options, the plan of care, or in processing their grief. 4 PCSWs are well suited to ensure that all family members have been updated about the meeting outcome and that they have opportunities for supportive processing and assistance with logistical arrangements.
PCSWs can also assist in creating space for providers to process the outcome of the meeting and their emotional experiences. PCSWs can ensure that members of the medical team who were not present for the meeting are aware of the plan of care and next steps.
Case: How Did the PCSW Assist in Moving Care Forward After the Meeting?
The PCSW met with the family to debrief the information that was discussed during the meeting. Nathaniel's parents and extended family were tearful as they voiced realizations about his critical state. Nathaniel reiterated his desire to see his dogs. The PCSW offered psychoeducation and reframing regarding disease progression.
The PCSW then met with Nathaniel's parents away from the beside. Nathaniel's father reflected on the first few months of Nathaniel's life and how his dreams for Nathaniel had shifted over time. The PCSW reflected that Nathaniel's parents had always made loving and thoughtful decisions for their children. His mother voiced concerns about losing control of Nathaniel's comfort and asked how other families moved forward with decisions. The PCSW offered that some families find it helpful to talk through which interventions they hope to protect their child from. The PCSW asked permission to include the palliative care attending physician in the discussion about limiting invasive interventions should Nathaniel's condition worsen. His parents also expressed that they would prefer for Nathaniel to die in the hospital surrounded by his siblings and familiar providers and asked about the possibility of Nathaniel's dogs visiting the ICU. The PCSW advocated to hospital leadership to allow Nathaniel's dogs to visit given his end-of-life status (Fig. 1).
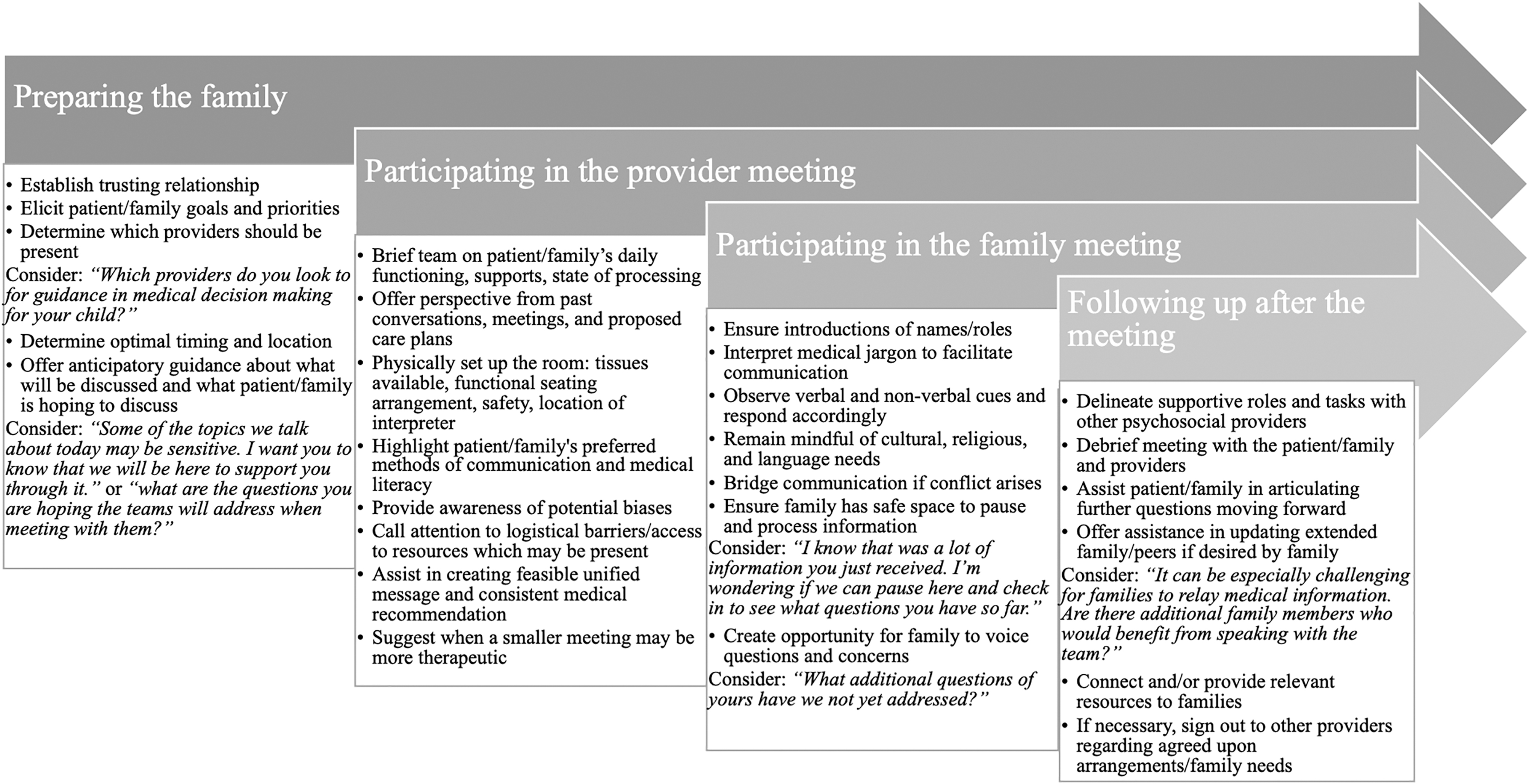
The social work role in family meetings.
Discussion
PCSWs play a critical role in optimizing communication, collaboration, and whole-person care. 5 This case discussion explores the ways in which PCSWs can demonstrate their unique skill set during family meetings. Although the PCSW role varies by case, institution, and team, their skill set needs to be further acknowledged and emphasized across medical systems. 5 PCSWs can do this in numerous ways. Specifically, PCSWs can highlight their unique role during family meetings by consistently attending and sitting near patients and families so that team members can visually see their supportive roles. Adding their assessments during provider and family meetings can serve as education for interdisciplinary team members about the PCSW role. Palliative care team members can also help raise awareness about the importance of the PCSW voice by prompting their colleagues to share their viewpoints in meetings. Consistent presence in the medical record can add additional value as documentation offers an expedited demonstration of the PCSW role in collaborative care. Over time, these practices can expand the impact of the PCSW and also raise awareness about the critical role played by the primary social worker, as well as other interdisciplinary providers, which are essential to family-centered care.
Conclusion
PCSWs have a crucial role in patient and family care. By raising awareness of social work roles and practices that are integral to high-quality palliative care services, patients and families will receive better care. The medical and psychosocial patient needs are inextricably intertwined. Representation of the patient and family's psychosocial factors is imperative when striving toward whole-person care. 15 The PCSW role is a necessary component of optimal family-centered, trauma-informed, and goal-concordant care.
Footnotes
Funding Information
No funding was received.
Author Disclosure Statement
No competing financial interests exist.