
Abstract
Objective:
To assess the face and content validity, acceptability and feasibility of a French version of the Children's Palliative Outcome Scale (CPOS).
Background:
Instruments in French used to measure outcomes in pediatric palliative care are lacking.
Methods:
After forward-backward translation of the 12-item English CPOS to French, we conducted a qualitative pilot study. During semi structured interviews among children and parents, we used the CPOS, the Schedule for the Evaluation of Individual Quality of Life interview guide (SEIQoL) and the Quality of Life in Life-threatening Illness-Family Carer questionnaire (QOLLTI-F), in addition to three expert meetings with PLTs.
Results:
Fourteen children and adolescents (8-18 years) with life-limiting or life-threatening conditions cared for at home, in hospital or in respite care services, 19 parents, and 9 members of 4 pediatric liaison teams (PLTs) providing palliative care in a Belgian francophone region were included in the study. No families refused to participate. All children with verbal capacities chose to be interviewed in the presence of their parents and a PLT member. The children valued being given the opportunity to share their experiences. New QOL dimensions pertaining to social, emotional, and administrative health-care related issues were added to the original version of the 12-item CPOS, leading to a 22-item CPOS-2.
Discussion:
The CPOS-2 was perceived as relevant and easy to use by the principal stakeholders. Our study paves the way for a large-scale field study assessing its psychometric characteristics and its implementation in routine clinical care.
Introduction
The main objective of pediatric palliative care (PPC) is to achieve the best quality of life (QoL).1,2 Measuring QoL in children facing life-limiting or life-threatening conditions (LLC/LTC) is challenging due to the subjective aspect of the construct, heterogeneity in ages and diseases of the children, the diversity of PPC models and interventions, and the legal and ethical requirements that must be observed when involving children in research.3–7
It has been recommended to develop a short, age-adapted, multidimensional patient-centered outcomes measure. This measure should include children's and parents' perspectives and should be perceived as acceptable by them. Furthermore, this measure should be feasible to use for clinicians.3–5,8–10 In accordance with this recommendation, Downing et al. developed the Children's Palliative Outcome Scale (CPOS),4,11 which is a short 12-item instrument combining self (child) and proxy (parents) reports regarding health status, health-related QoL, and QoL. It covers four dimensions: physical and psychological symptoms, information received, advance care planning, and self-efficacy.
In Belgium, pediatric liaison teams (PLTs) are ensuring continuity of care for children facing LLC/LTC across various care pathways. 12 Their activities as well as the profile of children they care for have been described in previous papers.13,14
The aim of the pilot study was to assess the face and content validity, acceptability, and feasibility of a French version of the CPOS among children facing LLC/LTC, their parents, and PLTs in the French part of Belgium.
Design
This qualitative pilot study is part of the larger Belgian MOSAIK study (Move to Open Shared Advanced Interventions for Kids with LLCs) and aims to develop a measurement instrument to assess children's and parents' QoL while receiving PPC. Figure 1 shows the place of the pilot study within the larger MOSAIK study.
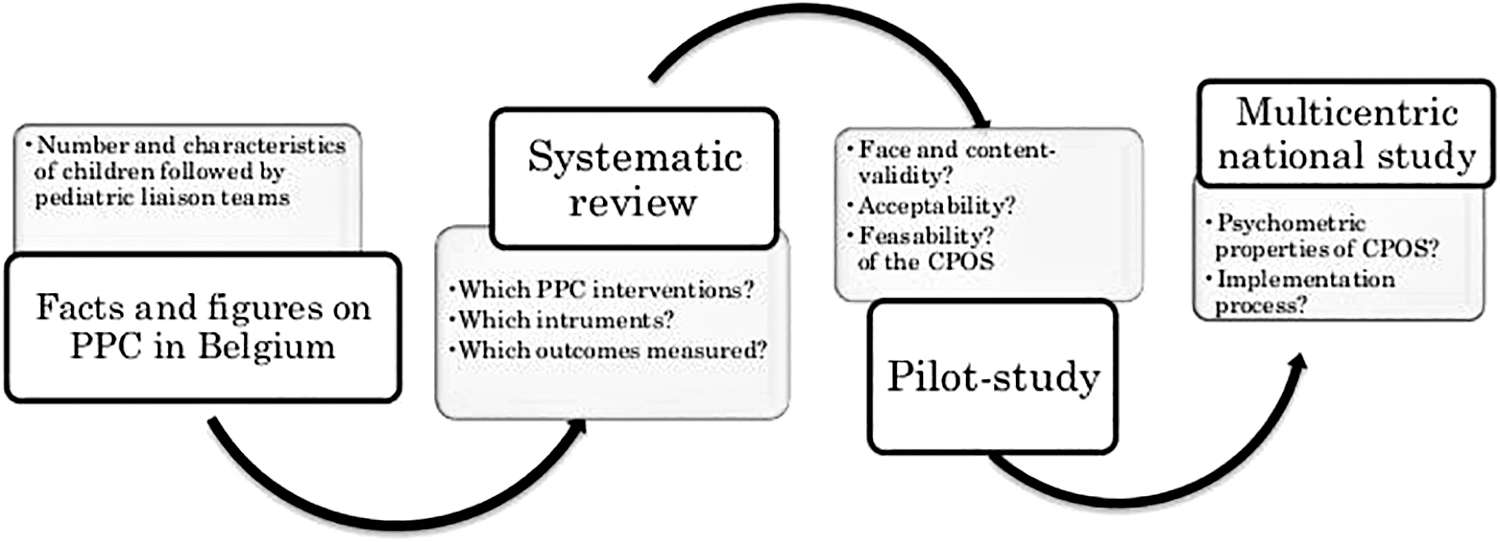
Design of the MOSAIK study with the embedded pilot study. MOSAIC
To comply with standards on ethical issues in palliative care research15,16 and recommendations17–19 on the development of a measurement instrument, especially regarding the assessment of face and content validity, we opted for an iterative and collaborative approach that involved the main stakeholders (children, parents, and teams) in the research process.
Data were collected through semistructured interviews conducted by the first author (M.F.) with children and their parents as well as three expert meetings with representatives of PLTs. Children and adolescents 8–18 years of age who were facing an LLC/LTC and their parents were included in the study. Families were recruited through one PLT in the French part of Belgium, and an interview was planned according to their preferences of time and place.
Instruments
A forward/backward translation of the CPOS was conducted based on guidance from Antunes et al. 20 and De Vet et al. 17
Face validity is defined as “the degree to which a measurement instrument indeed looks as though it is an adequate reflection of the construct to be measured” (17, p. 155). To assess the face validity of the CPOS for measuring children's and parental QoL, the researchers relied on previous work by Downing et al. 4 and discussed each translated item in French with PLTs.
Content validity is defined as “the degree to which the content of a measurement instrument is an adequate reflection of the construct to be measured” (17, p. 155). To assess the content validity of the CPOS for measuring children's QOL, the Schedule for the Evaluation of Individual Quality of Life (SEIQoL) was used.21,22 This semistructured interview guide aims to elicit self-generated domains of QoL as expressed by the children themselves. The SEIQoL was validated for use in children with diabetes, 23 children with cerebral palsy, 24 and adults with cancer. 25 As this population was not the one included in our study, we considered the SEIQoL only as a guide. To verify the content validity of the CPOS for measuring parental QoL, the Quality of Life in Life-Threatening Illnesses-Family Carer questionnaire (QOLLTI-F) was administered to parents. 26
All instruments were pretested with two children ages 8 and 10 to ensure the comprehensibility of the questions, but these children were not included in the sample size. Children, parents, and an expert panel composed of PLT members discussed the relevance and comprehension of each item included in the further developed French CPOS (Table 1)
Overview of the Instruments and the Interview Guide Used in the Pilot Study
Acceptability of the CPOS was assessed through the ratio of the number of families willing to participate in an interview versus the number that refused, the duration of the interview, and the families' comments on the acceptability of each item included in the CPOS.
The feasibility of using the CPOS was evaluated by members of the PLT who participated in the interviews through three expert panel reviews and think-aloud techniques that captured their individual spontaneous reflections following each family interview. Expert panel reviews and think-aloud techniques gave the researcher insights into the team's cognitive processes after having used the CPOS. Think-aloud techniques are well-known methods used in health research.27–29
The interviews were led by the first author (M.F.) and, according to the children's preferences, included their parents and/or a member of the PLT to enhance the children's sense of security and to involve the PLT in the use of the CPOS.
Data analysis: All interviews were audiotaped and transcribed verbatim for analysis based on an integrated approach of categorization.30,31 An initial list of codes reflecting the preexisting domains identified in the CPOS and the QOLLTI-F were used as a framework to organize the thematic categories inductively created through the interviews. The content validity of newly generated categories was discussed during three expert meetings with nine members of four different PLTs, including two pediatricians (B.B. and C.F.), six pediatric nurses specializing in PPC (C.T., B.T., D.B., M.M., S.B., and M.S.), one psychologist (M.J.), and two academic researchers (M.F. and I.A.).
Results
Fourteen children/adolescents, 19 parents, 9 PLT members, and 2 researchers participated in the pilot study, which was conducted from June 2017 to July 2018 Table 2).
Characteristics of the Participating Subjects (N = 42)
CPOS, Children's Palliative Outcome Scale; HCP, health care professionals; QOLLTI-F, Quality of Life in Life-threatening Illness—Family carer.
The original 12-item CPOS in English can be found in Supplementary Table S1, the adapted French version of the 22-item CPOS in Supplementary Table S2, whereas Supplementary Table S3 presents its translation in English.
The results are illustrated with quotations either from the interviews (I) with the families or from the expert meetings (M) (Table 3).
Comparison of the Dimensions Covered by the Original Children's Palliative Outcome Scale with Those That Emerged from Interviews with Children and Their Parents
The number of the question correspond to the adapted 22 items CPOS in French.
CPOS, Children's Palliative Outcome Scale (multidimensional standardized scale); SEIQoL, Scheduled Evaluation of Individual Quality of Life (semistructured interview guide); Q, Question.
Face and content validity of the CPOS
Regarding children's QoL, all four dimensions included in the original CPOS were confirmed, namely, physical and psychosocial dimension, playing, and the information received.
Two of those dimensions (physical/psychosocial dimensions) led to three more specific questions. One question addresses the quality of sleeping (Q8 of the adapted 22-item CPOS):
I always had nightmares that woke me up… I'm so frightened. (…). It awakens me at once, and my heart goes so fast that… When it happens, I stand up and I'm shouting everywhere. (Adolescent girl. Interview I 3) He struggles with the lying position in his bed. I don't know if it's a physical problem. Sometimes he doesn't sleep at all or he's up already at 5 am. (Father of a young boy. I8)
The second question focuses on the possibility of sharing worries with somebody (Q9):
At night, I am telling my teddy bear all that worries me. (Young girl, I5) No, I keep that inside of me. (Adolescent boy, I10) Indeed, that's the problem! He will shout, criticize, and yell instead of explaining calmly to the psychologist… It seems he doesn't know how to express himself. (Mother of a young boy, I12)
The third question looked at the feeling of being valued and loved (Q12):
A young girl with a progressive illness suggested adding a question about happiness because, according to her, this would be the most important one:
“You should ask if I am happy!” adding, “I am happy because I always have my parents by my side!” (young girl, I5)
This was in line with the father of a young boy (I8), who suggested that the child's perception of being loved contributed significantly to his QoL.
In relation to the dimension of physical symptoms, the initial question concerning the amount of feeding (Q3) was changed to include any type of worry, not just about the amount of food.
In relation to the dimension of playing, the question (Q6) was broadened to all activities and sources of fun and joy to be more adapted to adolescents.
I love playing sports, moving all around. I can't stand to keep calm. (Adolescent girl. I3)
He loves having parties, dancing, being with others and having fun. (Mother of an adolescent boy. I6)
In addition to the confirmed dimensions addressed by the original 12-item CPOS, one new dimension emerged regarding social relations, which was perceived as very important by all children and adolescents and led to two additional questions. One question focuses on friends (Q10) and one on their relations with their family (Q11).
I don't have a lot of friends. I'm missing that. (…) It's complicated to have some. I don't succeed at making them. (Adolescent boy, I6)
I really love my family. (…) I'm so happy when I'm going to see my aunt. It's ok between me and my brother. (Adolescent boy, I6)
In summary, all the dimensions of the original CPOS were confirmed, and questions on the newly generated dimension of social relations were added, leading to 12 questions addressing the children's QoL.
Regarding parental QoL, all dimensions from the original CPOS were confirmed, namely, psychosocial elements, the need to plan the future, information received, and the sense of self-efficacy. Within the psychosocial dimension, one question about worries was changed to focus on the impact that such worries have on daily life (Q13):
There was always this fear inside of us. We really couldn't sleep, couldn't eat, nothing. A permanent anxiety. (Mother of an adolescent girl. I3)
Another question was added to the overall perceived QoL (Q22), raising parental awareness of self-care and potential respite needs:
My quality of life is almost good, although we are struggling. (Mother, I8)
Within the dimension on self-efficacy, one question was added in relation to the perceived burden of taking care of their child (Q21):
Yes, it's a psychological burden. An enormous mental load. (…) The whole day, we are thinking about which medication we have to give him. (Father of a young boy. I8)
Two new dimensions of parental QoL emerged. The first dimension addressed the type of support perceived:
Dr X is open from Monday to Sunday and from Sunday to Monday. You can even call her late in the evening. … Dr X, you are super! And at that moment you feel supported. When they told us that we could always call her, ahhhhh, I had shivers up and down. Really! (Mother of a young boy. I2)
The second dimension focused on administrative issues (Q19):
Those files for the administration, these are crazy proceedings. We must ask Peter, Paul and Jack every time we need something. Stop now! All these papers take so much energy. (…) Even if they knew who my son his, we had to refile the paperwork, to start from the beginning, again! (Parents of a young boy, I2)
The relevance of one question included in the original CPOS, “Did you receive help and advice to Which future? We must learn how to live day after day, so this question isn't logical! (Mother, I4)
Conversely, for one parent of a severely handicapped child, preparing for the future was paramount:
The biggest fear since she was 7 years old is: What will she become when we won't be there anymore? D. will always be dependent on somebody…. (Mother of a young girl. I7)
We decided to remove that question because half of the population of children followed up by PLTs face neurological conditions.
Furthermore, we observed that one emerging dimension on death and dying could not be made operational in a questionnaire. In our study, one adolescent boy raised this topic by expressing how much he would like to see a dead street neighbor, yet he was facing a categorical refusal from his mother:
“Oh, come on, I'm in good spirits. I want to go outside and see the dead. I won't be sad, I promise you. Please! At least, I‘d seen a dead person in my life. (…) Everybody will go and see him, why not me? Why are you afraid?” (Adolescent boy, I6) “And what will I do If you will be shocked?” (Mother, I6) “I know what a dead person looks like. I'm not afraid of death, because my grandmother already died.” (Adolescent boy, I6)
Although this dimension was considered very important for PLTs, they decided not to add a related question to the CPOS, arguing that good practices would recommend waiting for children to initiate any questions on death and dying rather than broaching this topic directly in a questionnaire.
In summary, all the dimensions of the original CPOS were confirmed, and new dimensions, namely, support received and burden of administrative procedures and financial issues, were added to the adapted CPOS, leading to 10 questions addressing parental QoL.
Acceptability of the CPOS as perceived by the children and their parents
All invited families (n = 14) agreed to be interviewed, and the duration of interviews was considered acceptable by them (mean of 25 minutes, ranging from 12 to 75). Positive feelings about being interviewed were expressed by all children and parents:
“It was good.” (I3) “I liked it.” (I5) “I appreciated this moment.” (I6) “The questions are easy to understand, and it was easy to respond.” (I13) Their parents also expressed positive reactions: “Very good, very pleasant.” (Father I6) “Nothing else to say. It's not intrusive at all.” (Mother, I8) “I found that very good. That's why I always agree to participate.” (Mother, I7)
Furthermore, parents said that it allowed them to identify what helped them and to express to one another their mutual sense of gratitude:
For 75%, it was her fathers' merit, because he was always there for her, being a huge force. And this inner force inside him never diminished. Sometimes I was asking myself: how can he stand all this? Day and night, day and night, day and night to care for her and to care for us, to clean the house, to transport here and there with the car… (Mother, I3)
Feasibility of using the CPOS as perceived by the PLTs
As detailed in the methods section, the PLTs were involved in the entire process of the study. They perceived the CPOS as a useful tool that shined a “warning light” on overlooked domains, helping them to individualize and to improve the care provided. For instance, a teenager expressed during the interview that he was longing for more contacts with his peers. The liaison nurse who had conducted the interview consequently made suggestions for him to take part in monthly gatherings of an inclusive scout movement. One month later, the mother reported that her son greatly appreciated this new activity and felt less depressed.
Discussion
Our study confirmed the face validity and strengthened the content validity of the primary dimensions included in the original 12-item CPOS, the acceptability of the CPOS to families and its feasibility of use for caregivers. Questions related to meaningful domains as expressed by the children, parents, and PLT members were added to the original instrument, ultimately leading to a 22-item tool that explores children's and parents' QoL. Several issues can be discussed.
Challenges identifying meaningful outcomes to be included in a measurement instrument
Outcome measurement instruments should be derived from meaningful outcomes, defined by the patients themselves. Many studies exploring meaningful outcomes in PPC rely only on parents' and/or professionals' perspectives, which is a first step to assess the content validity of an instrument.32,33 However, directly identifying among what matters most to children, that is, measuring individual QoL, is recommended but challenging. Following recommendations by previous studies3,4,10,17,34,35 and to further strengthen the evidence of the CPOS to assess meaningful QoL domains, we used the SEIQoL interview guide,21,22 through which children spoke out, elicited self-identified QoL domains, and appreciated being consulted. However, in a PPC context, where many children lack cognitive capacity or are very young and consequently have difficulties expressing themselves, PLTs perceived the SEIQoL to be too complicated to be routinely used.
Furthermore, our results are consistent with a systematic review that identified five domains of meaningful outcomes in PPC: physical, psychological, psychosocial, existential, and information access. 36 More specifically, the importance of relationships for children found in our study was highlighted in two further studies.37,38 The complexity of those relationships could be analyzed through the concept of normalcy, which was found to be paramount in one study, including children with brain tumors. 39 Children want to have relationships, but on the other hand, they are suffering due to feeling different than their peers. Furthermore, existential dimensions should be explored through hopes, worries, meanings, and life perspectives, 40 rather than using words such as religion or spirituality.
Acknowledging the Ethical and Psychological Requirements When Including Children in Research
The necessity of collecting data directly from children facing LLC/LTC entails adapting methods that are appropriate for their cognitive and age-specific development and ensuring a safe space by valuing their preferences.41,42 Accordingly, in our study, we respected children's choice to be interviewed in the presence of their parents, even if this might introduce social desirability bias. However, reporting noninvitation rates and selection bias whenever possible may aid in the interpretation of research findings. 43 The ethical imperative that research in PPC must benefit children 35 was acknowledged by PLTs, who conducted the interviews and offered individualized care, responding immediately to the needs expressed by children during the interview.
Limitation and Strength
Comparison of the data among the different children has not been possible because of the evolutive nature of the questionnaire. Although this study is monocentric, the relevance and comprehension of each item has been discussed by an expert panel composed of multicentric PLTs. Potential social desirability bias could have been a factor on account of the children having been interviewed in the presence of their parents and their usual PLT. Furthermore, our sampling did not represent the wide variety of diseases labeled LLC/LTC, potentially restricting the emergence of other self-identified domains of QoL. Finally, the perspectives of very young children or those with serious verbal and cognitive deficiencies could not be considered.
Nevertheless, to our knowledge, this is the first study to test a French version of the CPOS in a European context of PPC. Moreover, triangulation of data sources contributed to the content validity of the CPOS. Finally, the collaborative approach planted the seeds for a sustainable implementation process of the instrument in clinical care, as recommended.19,44–47
Conclusion
Face and content validity, acceptability, and feasibility of a French version of the CPOS were assessed by integrating the perspectives of 14 children, 19 parents, and 9 PLT members, leading to three major results. First, using a specific and unique procedure, a revised 22-item CPOS-2 was developed. Second, this instrument was perceived as relevant and easy to use by the principal stakeholders. Third, this study paves the way for an additional large-scale multicentric field study, in which the psychometric characteristics as well as the challenges linked to its implementation in routine clinical care will be studied.
Research Ethics and Patient Consent
The pilot study was approved by the Ethics Committee number 403, attached to University Hospital Saint Luc, Brussels, Belgium under the name MOSAIK 2017/16MAI/271 and registered under the number B403201732735. The Ethics Committee declared that the study followed Good Clinical Practice (GCP). Informed written consent was obtained from each parent who agreed to be interviewed. Whenever the child/adolescent was able to understand or communicate, he or she was invited to sign an adapted age-appropriate written informed assent form.
Footnotes
Acknowledgments
The authors would like to express their deeply felt gratitude to each child/adolescent and parent who agreed to share their experiences within this study; the African Palliative Care Association for their permission to use the APCA-Children's Palliative Outcome Scale; Prof. Robin Cohen for permission to use the Quality of Life in Life-threatening Illnesses-Family Carer (QOLLTI-F) questionnaire; Mandana Mehta, Pauline De Becker, and Claire Mougenot, who contributed to the linguistic and semantic forward/backward translation of the CPOS; and Sophie Agboli, Thérèse Van Durme, Nathalie Chaidron, Valérie Dory, and Nataly Filion for their informal support. For their unwavering support since the beginning, the authors would like to thank the Fonds de Soutien Marguerite-Marie Delacroix, who funded the study in the frame of a PhD thesis conducted by M.F.
Authors' Contributions
M.F., I.A., and J.M. designed the study. M.F. conducted the interviews and meetings and analyzed and interpreted the data. B.B., S.B., C.T., B.T., D.B., and M.M. contributed to the collection and analysis of the data, and C.F., M.J., M.S. and I.A. participated in the interpretation of the data collected. I.A., J.D., R.H., J.D., and E.N. critically revised the article. All authors approved the final article as submitted.
Funding Information
Funds Marguerite-Marie Delacroix and Haute Ecole Léonard de Vinci.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.