
Abstract
Background:
The use of formalized criteria (or triggers) for palliative care services (PCSs) has been associated with increased use of PCSs in the intensive care unit (ICU).
Objective:
To explore the utility/validity of frailty as a trigger for providing PCSs.
Design:
This is a prospective cohort study.
Setting/Subjects:
Older adults (age ≥50 years) admitted to ICUs were enrolled.
Measurements:
We measured frailty using the Clinical Frailty Scale. We reviewed electronic health records for the presence/absence of six evidence-based triggers, the use and quality of specialty palliative care (SPC), and markers of primary palliative care (PPC). We used descriptive statistics to describe the differences in PPC, SPC, and six-month mortality by frailty and by the presence/absence of triggers.
Results:
In a study population of 302 older adults, mean (standard deviation) age 67.2 years (10.5), 151 (50%) were frail and 105 (34.8%) had ≥1 trigger for PCSs. Of the 151 (55.6%) frail patients, 84 had no triggers for PCSs, despite a 46.4% six-month mortality in this group. Patients with ≥1 trigger had higher rates of SPC than those without (39.1% vs. 18.3%, p < 0.001); frail patients also had higher SPC than nonfrail patients (32.5% vs. 18.5%, p = 0.006). Patients with ≥1 trigger had higher rates of PPC than those without (66.7% vs. 44.2%, p < 0.001); no statistically significant difference in PPC was found by frailty (56.3% vs. 47.7%, p = 0.134).
Conclusion:
The rates of PCSs and six-month mortality by frailty are consistent with frailty being a valid trigger for PCSs in ICUs; the high prevalence of frailty relative to triggers suggests that ways to increase PCSs would be needed.
Introduction
Older adults admitted to the intensive care unit (ICU) appear to be at higher risk of mortality and morbidity.1,2 Recent studies suggest important heterogeneity in outcomes for critically ill older adults.3–5 How best to provide value-concordant care to the heterogeneous mix of older adults has emerged as one of the 21st century challenges in critical care.6,7
Frailty is an aging-related syndrome characterized by both a diminished physiologic reserve and an increased susceptibility to adverse events after stressors.8,9 Multiple observational cohort studies in older adults with critical illness suggest that frailty is as an important risk-stratification tool in critically ill older adults. Frailty has been associated with increased short-term mortality, increased disability, higher health care utilization, and other adverse outcomes.3,9–11
The use of formalized criteria or triggers for palliative care services (PCSs) has been shown to be associated with increased utilization of palliative care consultation in the ICU setting.12–17 No previous study has explored frailty as a possible trigger for PCSs in older adults admitted to ICU. In a cohort of older adults with critical illness, we aimed to address this gap in knowledge within an integrated model of PCS delivery that includes specialty palliative care (SPC) and primary palliative care (PPC) provided by the primary clinical team. 14 First, we examined the provision of PCSs (both SPC and PPC) by both frailty status and the presence/absence of palliative care triggers. Because six-month mortality has been used to validate the need for PCSs in critically ill populations,5,6 we then compared PCSs and six-month mortality by both frailty status and the presence/absence of palliative care triggers.
Methods
Study design, setting, and study population
We conducted an observational prospective cohort study at two tertiary care hospitals in Bronx, NY, between January 2016 and July 2017, the details of which (including the inclusion/exclusion criteria) have been previously described. 18 The institutional review board of Albert Einstein College of Medicine approved the study.
Defining PPC and SPC
Our primary definition of PPC was the evidence in the chart of any family discussion by a member of the primary clinical team. 19 Other secondary measures of PPC that we collected included the presence of advance directives documented in the notes before ICU transfer: any documentation in the notes of the patient's next of kin before ICU transfer. 19 The primary definition of SPC service was the formal request for palliative care consultation and the palliative care team completing an initial consultation on the patient. We also collected, through chart review, information on the number of visits from SPC and the quality of SPC services provided that included assessment of common symptoms; assessment of the patients and family members psychosocial status; assessment of spiritual concerns; and documentation of the patient's preference for care and advance directives. 19
Frailty exposure variables and other covariates
The research coordinator conducted a baseline interview from the patient or surrogate who focused on demographic characteristics, functional status, and medical comorbidities. Frailty was assessed using the Clinical Frailty Scale, a judgment-based frailty assessment tool that classifies the patient on a scale between 1 and 9: 1 to 3 (fit); 4 (vulnerable); and ≥5 (frail). 20
Triggers for palliative care
During the study, no specific triggers for PCSs were mandated or in general use across the ICUs. Evidence-based triggers for PCSs were extracted from manual chart review and, where appropriate, the electronic health record using Clinical Looking Glass (CLG TM Emerging Health Information Technology, Yonkers, NY): pre-ICU hospital length of stay >10 days; age >80 years with the presence of two or more major comorbidities; history of stage IV malignancy; cardiac arrest; diagnosis of intracerebral hemorrhage requiring mechanical ventilation or global cerebral ischemia; and admitted from a subacute rehabilitation facility or nursing home.15,17
Statistical analysis
Both frailty and triggers were categorized as binary variables: frail versus not frail and presence versus absence of any of the six evidence-based triggers.21–23 We used standard descriptive statistics to describe the demographic characteristics, SPC and PPC by both frailty status and the presence or absence of triggers. Next, we merged frailty identification and the presence/absence of triggers into four mutually exclusive categories and used chi-squared test to describe SPC, PPC, and six-month mortality across the four categories. A p-value <0.05 was considered statistically significant. We used Stata 15 for all data analyses.
Results
Table 1 compares the evidence of PPC and SPC in the study population by frailty status in the study population of 302 older adults [mean (standard deviation) age 67.2 years (10.5) in which frailty was quite prevalent (n = 151, 50%)].
Patient Characteristics within the Study Population Stratified by Prehospital Frailty Status
APACHE, acute physiology and chronic health evaluation; ICU, intensive care unit; IQR, interquartile range; SD, standard deviation.
Table 2 describes markers of PPC and SPC by frailty status. We found evidence of a family meeting documented by the primary clinical team (our primary measure of PPC) in 157 of 302 (52%) patients; we found no difference in PPC by frailty (56.3% vs. 47.7%, p = 0.134). Frail patients were more likely to have a next of kin documented in a clinical note before ICU transfer (67.6% in frail patients vs. 52.0% in nonfrail patients, p = 0.006). SPC was called in 77 (25.5%) patients, completed in 75 (24.8%) patients within a median (interquartile range [IQR]) of 12 (6–19) days from the ICU admission date. Frail patients were more likely to have SPC (31.8% in frail patients vs. 17.9% in nonfrail patients, p = 0.005), although there was no difference by frailty in the time from ICU admission to SPC (Table 2).
Markers of Primary or Specialty Palliative Care Services by Prehospital Frailty Status
This was our primary measure or PPC. See text for more details.
PPC, primary palliative care; SPC, specialty palliative care.
Table 3 describes the evidence of PPC and SPC by the presence or absence of palliative care triggers. Patients with any triggers appeared more likely to have evidence of our PPC measure [70/105 (66.7%) in those with triggers vs. 87/197 (44.2%) in those without a trigger, p < 0.001]. SPC consultation was also more likely to be completed in those patients with a trigger (37.1% vs. 18.3%, p < 0.001) and was completed earlier in the hospital course [median (IQR) days from ICU admission to SPC 9 (5–16) in those with triggers vs. 17.5 (8–25) in those without, p = 0.004].
Evidence of Primary or Specialty Palliative Care Services Based on the Presence or Absence of Evidence-Based Palliative Care Triggers
This was our primary measure of PPC.
Figure 1 shows the rate of SPC, PPC, and six-month mortality across four categories of patients: patients without triggers and without frailty (n = 113), patients with ≥1 trigger and no frailty (n = 38), patients without triggers but identified as frail (n = 84), and patients with ≥1 trigger and also identified as frail (n = 67). Patients identified as frail without any of the evidence-based triggers had a six-month mortality similar to that of patients with triggers but appeared to have lower rates of SPC and PPC.
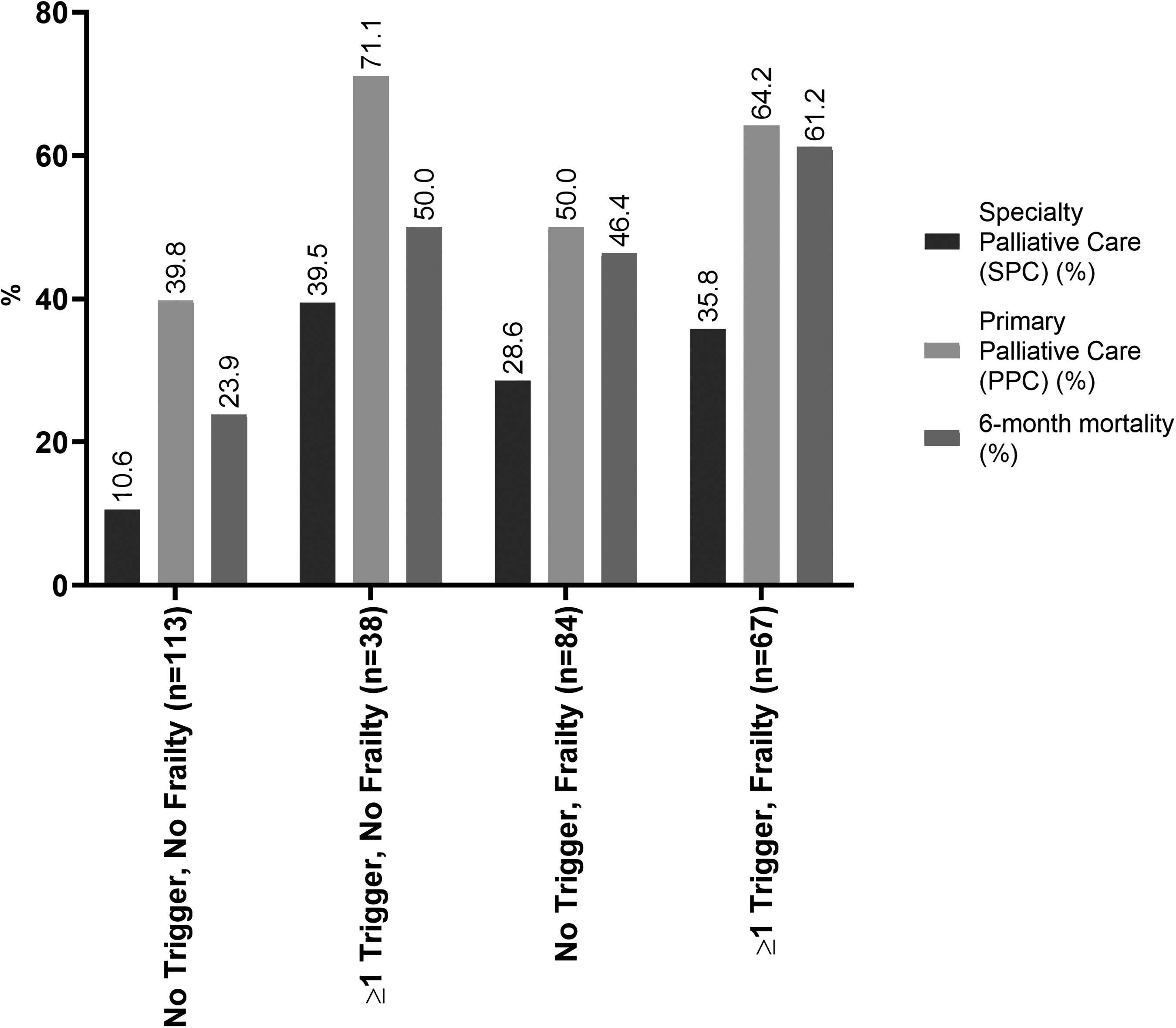
The rate of specialty palliative care, primary palliative care, and six-month mortality across four categories of patients: patients without triggers and without frailty, patients with ≥1 trigger and no frailty, patients without triggers but identified as frail, patients with ≥1 trigger and also identified as frail.
Discussion
In our study population of older adults admitted to ICU, frailty was identified in 50% of the population whereas evidence-based triggers for PCSs were present in ∼35% of the population. Both frailty and the presence of triggers were associated with higher SPC utilization. Although the time from ICU admission to SPC was not different by frailty status, ≥1 trigger was associated with earlier SPC consultation. In addition, patients with triggers were more likely to have PPC than those patients without triggers, whereas no such difference was noted when we compared PPC by frailty.
That we found higher rates of palliative care triggers than previous retrospective studies may be attributable to the fact that we enrolled adults ≥50 years who were sicker patients than some of the previous studies.16,17 The utilization rates of SPC in our cohort is consistent with previous studies that have suggested that clinicians still misperceive palliative care to only be relevant near the end of life. 24 The high prevalence of frailty in our study coupled with innovative approaches to increase the use of both SPC and PPC in the care of critically ill older adults. 25
Although one previous study explored clinicians' attitudes about palliative care triggers and found that clinicians favored triggers that included pre-existing characteristics of the patients, 24 more research would be needed to explore how the various stakeholders would view the use of frailty assessment as a screening criterion for PCSs in the ICU. In addition, more research would be needed to explore the communication and symptom challenges that are relevant to frail older adults during and after critical illness. 26
This is a single-center study with a small sample. We did rely on medical record abstraction for our measures of PPC and SPC. Although our approach has been used in previous studies, it has not been previously validated. We may have underestimated the quality of PPC since our measure depended on note documentation of communication interventions and did not include other aspects of PPC such as pain and symptom management. 19
Prehospital frailty in critically ill older adults may be a valid trigger for PCSs during critical illness. Future research should focus on testing strategies to increase PPC and SPC services in older adults during critical illness.
Footnotes
Funding Information
National Institute of Aging R03 AG05092 (AAH). National Heart, Lung, and Blood Institutes K01 HL140279 (AAH), U01 HL122998 (MNG), U01 HL143453 (NNG). National Center for Advancing Translational Sciences Institutional Career Development Core KL2TR002558 through the Einstein-Montefiore Institute for Clinical and Translational Mentored Clinical/Translational Research Career Development Award (EC).
Author Disclosure Statement
No competing financial interests exist.