
Abstract

Dear Editor:
Some patients with malodorous wounds cannot receive sufficient palliative care regarding odor due to their systemic condition. The currently recommended topical therapy for wound odor control is the antibiotic metronidazole or an activated charcoal dressing.1,2 However, the optimal dose or dressings to ensure efficacy and cost-effectiveness are unclear. 3
Recently, rice bran, one of the most abundant and valuable by-products produced during the rice milling process, is gaining interest for its potential health benefits. Rice bran has effective microorganisms, which has been demonstrated to reduce odor in vitro. 4 This clinical study evaluated the antiodor effects and safety of rice bran sheets in the management of malodorous wounds.
This was an open label pilot study with a pre–post design; assessments were made before and after an intervention, without a control group. This study was conducted in accordance with the ethical principles described in the Declaration of Helsinki (UMIN-Clinical Trials Registry: UMIN000031276) and approved by the ethics committee of Shimane University (Approval No. 2822). All participants provided written informed consent before the study. Patients were assessed at two time points: on entry into the study just before the application of rice bran sheets and at day 7 after the application. Rice bran sheets were applied over the gauze after the dressing change once daily.
The effects of rice bran sheets were judged by measurements with a six-stage odor intensity display, nine-stage pleasure/displeasure display, and the odor measuring device. Wound odor was rated both by patients and physicians on a 6-point scale (0 = no odor, 1 = slight odor, 2 = moderate odor, 3 = strong odor, 4 = very strong odor, and 5 = overpowering odor). A hedonic scale of odor from 4 to −4 (4 = highly like, 3 = like very much, 2 = like moderately, 1 = like slightly, 0 = neither like nor dislike, −1 = dislike slightly, −2 = dislike moderately, −3 = dislike very much, and −4 = greatly dislike) was also used. A handheld odor meter (OMX-ADM; Shinyei Technology Co., Ltd., Kobe, Japan) was used to display a numeric odor strength level. Changes in the odor intensity, and hedonic and strength levels were assessed for significance using the paired Wilcoxon signed-rank test.
Fifteen patients were recruited for this study. The mean age of the participants was 64.9 ± 2.5 (mean ± standard error) years (range 48–78 years). Wound etiologies were arterial leg ulcer (five), diabetic ulcer (three), skin cancer (three), burn ulcer (two), and others (two). A total of 12 species were isolated from the 15 wounds. The most common bacterial species was Staphylococcus aureus (12), followed by Proteus mirabilis (4), Pseudomonas aeruginosa (4), Escherichia coli (4) and others (8). Side effects, including rice bran allergy, were not observed in all patients during the study. The patients' and physicians' subjective assessment of odor intensity improved significantly (p = 0.003). The patients' and physicians' subjective assessment of odor hedonics also improved significantly (p = 0.002, p < 0.001). Furthermore, the results of odor meter analysis (odor strength level) improved significantly (p < 0.001) (Fig. 1).
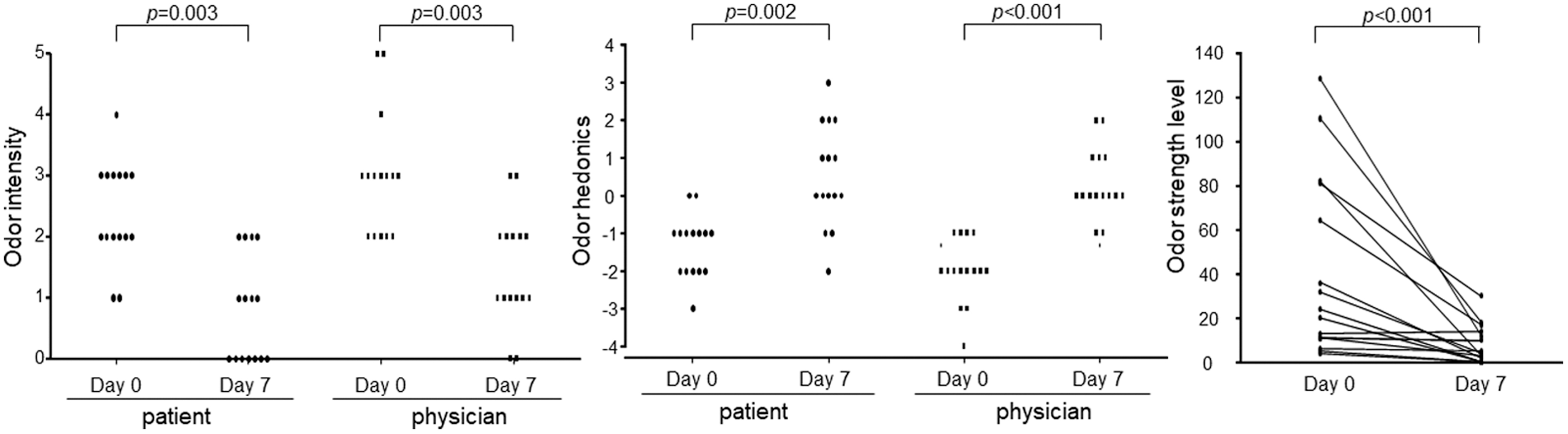
Improvement of both patients' and physicians' assessments of odor intensity (left) and hedonics (center), and improvement of odor strength level measured using the odor-sensing device (right) by the application of rice bran sheets.
Preliminary data suggest that rice bran is safe and effective to use in patients with malodorous wounds. Further research, including basic studies, on these cost-effective natural substances for odorous wounds are needed, especially in palliative care.
Footnotes
Funding Information
This study was supported in part by Shiraishi Biomass Co., Ltd.