
Abstract
Thanks to the efforts of many individuals and organizations, the field of Hospice and Palliative Medicine (HPM) has undergone unprecedented growth over the last two decades. To meet the needs of seriously ill patients and families in inpatient, outpatient community setting in the future, the field of HPM must develop innovative strategies to expand the specialist workforce pipeline. With 148 programs participating in the National Residency Matching Program and 285 matched applicants in 2019, the specialty of HPM can barely replace those who are retiring or leaving the field. We call for a renewed and coordinated effort to increase the applicant pool for HPM fellowship positions, as well as greater access to specialist HPM training through expanded traditional fellowship programs and innovative specialist training pathways. Without such an expansion, our specialty will struggle to serve those patients and families who need us most.
To meet the growing need for Hospice and Palliative Medicine (HPM) physician specialists across health care settings, coordinated and focused efforts are needed to increase the applicant pool for fellowship positions, and to expand access to traditional and nontraditional paths for specialist training.
The field of HPM has experienced unprecedented growth and success over the past 20 years. Early awareness of palliative care grew out of the Project on Death in America, as well as the Robert Wood Johnson Foundation's Promoting Excellence in End-of-Life Care program. A robust body of research built on these early efforts demonstrated the value of palliative care in improving quality of life, 1 improving quality of medical care, 2 and in reducing costs. 3 These efforts have been crucial in advocating for additional resources for inpatient and community-based palliative care programs. Success of these efforts is evidenced by the growth in the presence of inpatient palliative care programs from 15% of hospitals in 2001 to 67% of hospitals in 2016. 4
Extraordinary educational outreach has led to shifting attitudes and increased understanding of the value of specialist palliative care, as well as recognition of the importance of developing palliative care skills in all health care providers. Numerous programs, including the Education on Palliative and End-of-Life Care (EPEC) Project launched by the American Medical Association with funding from the Robert Wood Johnson Foundation, EPEC-Oncology created at Northwestern University with support from the National Cancer Institute and the American Society of Clinical Oncology (ASCO), “Fast Facts” from the Medical College of Wisconsin, VitalTalk, and the Serious Illness Care Program, were developed to build primary palliative care skills among all providers in the medical system, and have generated a number of spin-off programs that have reached thousands of clinicians. In recognition of the unique expertise needed to provide hospice and palliative medical care, 10 of 24 American Board of Medical Specialties (ABMS) specialty boards recognized HPM as a medical subspecialty in 2006.
The result of these efforts has led to the historic expansion of HPM capacity in the United States. Advocacy to advance the mission of palliative care continues led by the Center to Advance Palliative Care (CAPC), the American Academy of Hospice and Palliative Medicine (AAHPM), the Hospice and Palliative Nurses Association (HPNA), the National Hospice and Palliative Care Organization (NHPCO), ASCO, and palliative care specialists and enthusiasts in many other subspecialty societies.
As we look to the dawn of the next decade, the field of HPM faces new and unique challenges and opportunities in expanding access to palliative care services to all seriously ill patients and their families. Chief among these is ensuring a robust and sustainable specialty HPM workforce to meet the growing demand for palliative care services in community, hospital, and hospice settings. Despite remarkable growth, few hospital-based palliative care programs meet the Joint Commission's national staffing recommendations. Consult requests at many institutions are growing so quickly 5 that many teams are driven to institute strategies to manage unsustainable consult volumes, including capping the number of new patients that can be seen daily. 6 While hospice censuses are growing more slowly, the number of available HPM or Hospice Medical Director (HMD) board-certified physicians still does not meet the demand of hospice programs and patients.7,8 Access to outpatient and community-based palliative care services remains limited. 9 Training in primary palliative care, 10 while necessary for the provision of high-quality care for all seriously ill patients, requires a supply of HPM specialists to lead these initiatives and deliver education.
The current shortage and impending workforce crisis for our field has been well documented. The growth in physician fellowship positions and applicants, although substantial, appears to have reached a plateau in the neighborhood of 150 and 350, respectively (Fig. 1). Now that fellowship is required for recognition as an HPM specialist, the field must aim higher. Much higher. In the next decade, a comprehensive and coordinated effort to expand the HPM specialty training pipeline is needed. Efforts are also needed to increase advanced training opportunities for nurse practitioners, physician assistants, pharmacists, and other health care providers interested in entering specialty HPM practice. Increased training for clinicians from varied disciplines is vital to addressing workforce shortages and ensuring that all patients with serious illness have access to hospice and palliative care services, particularly in geographic areas with few HPM physician specialists.
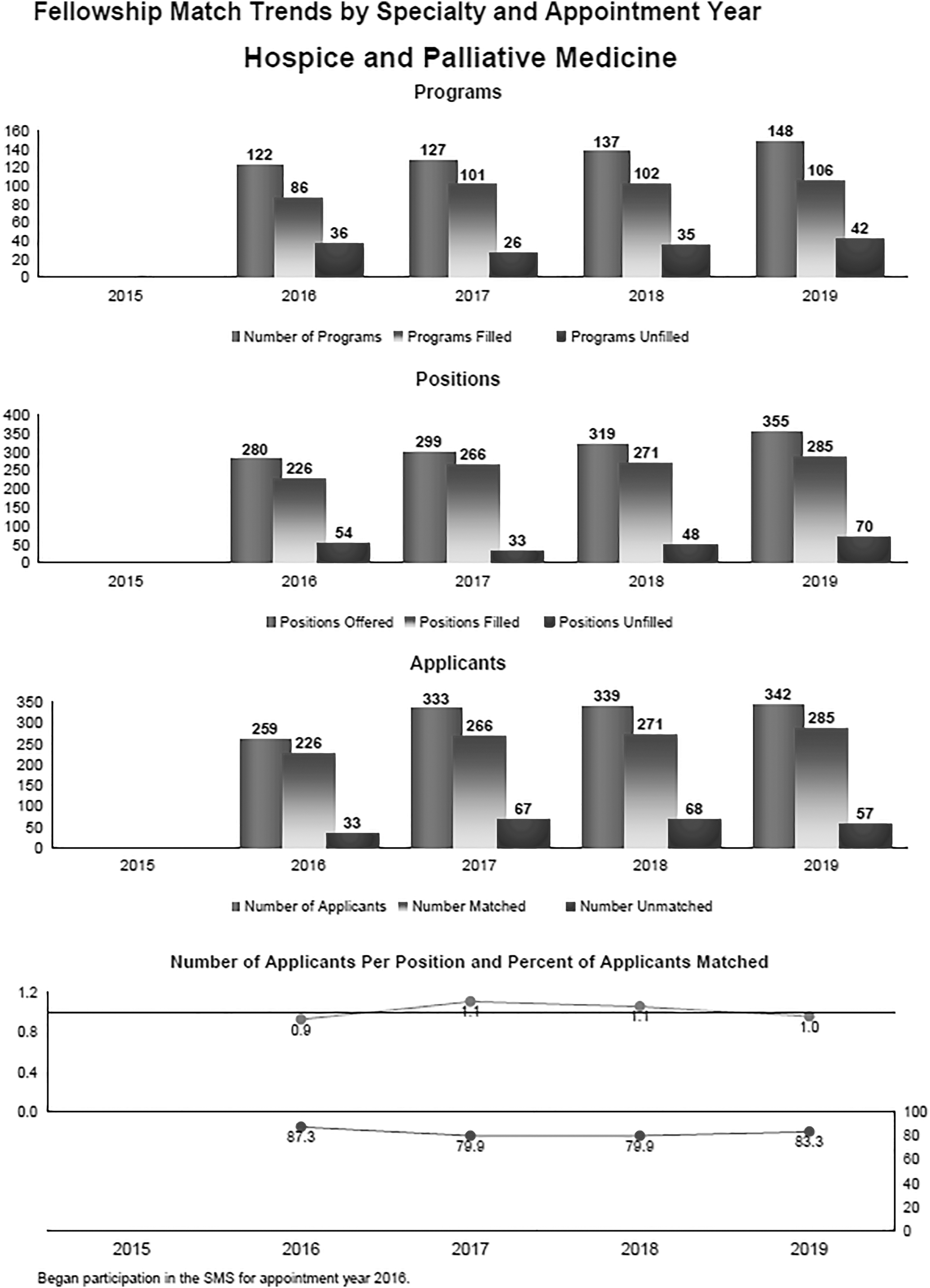
Fellowship match trends by appointment year—Hospice and Palliative Medicine.
As for growth in the physician workforce, current fellowship levels remain inadequate. The AAHPM reported 6400 active physicians in full- or part-time practice of specialty HPM in 2016. These providers could be estimated to represent 6000 full-time equivalents (FTE) HPM physician specialists, given that a proportion of these individuals are engaged in part-time HPM practice, and 6.5% are involved in education, administration, or research much or most of the time. The American Association of Medical Colleges physician workforce report 11 offers guidance in estimating workforce attrition. A 5% annual attrition rate due to retirement and departure from full-time practice would represent a loss of 300 physicians annually. Current HPM fellowships have the capacity to produce 330 graduates annually, resulting in net growth of 30 providers per year for the workforce. Using these rough estimates, and assuming that all fellowships fill to capacity and all graduates enter full-time HPM specialty practice, we could expect a workforce capacity of 6300 FTE HPM specialist providers in 10 years—an estimated gain of only 300 FTE from current levels.
Extensive modeling work by the George Washington University Health Workforce Institute established a recommendation for 600 annual fellowship graduates to both meet the needs of an aging population and replace physicians who exit HPM specialty practice. 8 A recent study by Kamal et al. predicted a workforce valley in the coming years due to increased attrition as a result of burnout. 12 This study established a recommendation to grow HPM fellowships to 575 positions annually to replenish and grow the HPM specialist physician workforce. However, even these targets may be too conservative to adequately meet the needs of the HPM workforce, including needed growth in outpatient and community-based palliative care programs.
As the field seeks to grow, barriers clearly exist to increasing the supply (fellowship positions) and demand (fellowship applicants) needed to expand the HPM specialty pipeline. Some of these barriers are known, while others are yet to be clearly defined.
Funding is a significant challenge to expanding the supply of HPM fellowship programs and positions. Many fellowship directors and program chiefs already struggle to maintain funding for existing fellowship positions, let alone expand the number of funded positions in a program. Most teaching hospitals have already exceeded their Medicare Resident Limits, which determine allocation of state and federal dollars to hospitals to support graduate medical education and these residency “caps” have not been increased since 1996. 13 Ongoing financial challenges for teaching hospitals limit willingness and resources for institutional funding for new or expanded programs, particularly as Medicare funding covers only half of the costs for each fellowship position. Additional funding is needed to support HPM educators in creating and administering fellowship training programs.
If additional fellowship positions are created, it is critical to ensure a robust pool of candidates to populate training programs. In 2019, many HPM fellowships remained below capacity, as only 285 of 355 positions were filled in the National Residency Match Program. 14 Unfortunately, medical students and residents often lack the exposure to palliative care that might inspire them to explore a career in HPM. While many medical schools report their students are taught palliative care, curricular time is at a premium, and students may have limited clinical experiences in HPM. Similarly, there are few required HPM rotations in residency training, limiting residents' exposure to HPM at a time when they are making critical decisions about whether to apply for advanced training. Furthermore, as young physicians face mounting debt burden, they may be reluctant to delay practice for a year to complete a specialty fellowship, which may not significantly increase their earning potential. Midcareer physicians wishing to pursue training in specialty HPM have limited opportunities to do so, and often find it unrealistic to step away from professional responsibilities, salaries, and benefits to pursue a 12-month fellowship.
However, there is hope. Barriers are already being addressed by large and small HPM-related organizations across multiple fronts. The AAHPM has led the way since they helped advocate to gain accreditation for HPM fellowships in 2006. AAHPM, HPNA, CAPC, NHPCO, and others have proposed the Palliative Care and Hospice Education and Training Act (PCHETA), 15 which was passed with bipartisan support by the House of Representatives and awaits action in the Senate. PCHETA would create new education centers and training programs, and establish incentive awards for physicians, nurses, physician assistants, social workers, and other health professionals to promote entry into our profession. The bill would create the academic infrastructure essential to grow HPM and provide funding for palliative care research to strengthen clinical practice and health care delivery. Nonetheless, PCHETA alone will not solve the workforce shortage.
The HMD Board has begun to address hospice workforce needs. Organizations representing HPM continue to advocate for fair compensation for HPM specialists and fight to preserve existing compensation. Ongoing efforts seek to expand models of reimbursement, which more fairly compensate for this challenging and time-consuming work, and better reflect its impact on patients, families, and systems.
Innovative approaches to expanding access to training for midcareer physicians are underway. Master's degree and certificate programs provide opportunities for midcareer physicians and other interdisciplinary team members to expand their knowledge and skills in palliative care practice. While these programs do not lead to board eligibility, they train palliative care champions who can provide advanced palliative care services to seriously ill patients. 16
This year, the Accreditation Council for Graduate Medical Education (ACGME) and multiple subspecialty boards have approved innovative training programs to expand access to subspecialty training and board eligibility for midcareer physicians. In one case, a time-variable training program leading to board eligibility will allow midcareer physicians to pursue specialty HPM training on a flexible, interrupted schedule while maintaining existing responsibilities, salaries, and benefits. This training program builds on the work that AAHPM has done to develop specialty-specific entrustable professional activities (EPAs), curricular milestones (CMs), and reporting milestones (RMs), and embraces a competency-based advancement approach. A second innovation will pilot coupling an established master's degree program with remote clinical experiences, which may expand access to training for midcareer physicians in areas without established fellowship training programs.
And we can do more by the following:
Advocating locally for more time in undergraduate curricula with careful study of the impact of such efforts on career choice. Working to change Liaison Committee on Medical Education (LCME) standards to require HPM experiences for undergraduates. Expanding required HPM experiences for residents and studying the downstream effect of such experiences. Calling for cap-exempt funded HPM fellowship positions. Supporting partnerships between fellowships and large hospices to fund fellowship positions. Advocating for increased Department of Veterans Affairs support for HPM fellowships. Identifying existing programs whose capacity for fellowship training is not fully exploited, while helping to identify barriers to expansion and addressing those barriers. Building upon the AAHPM Fellowship Directors' Guide to provide additional resources and support to those seeking to establish new fellowship programs. Continuing to partner with other specialty societies such as ASCO and the American College of Cardiology whose interests align with fellowship growth. Continuing to advocate for and support innovative fellowship models in partnership with the ACGME and HPM cosponsoring boards, including the following: ○ Building upon efforts to create EPAs, CMs, and RMs with further development of robust learner assessment strategies, which could advance HPM beyond purely time-based certification pathways. ○ Creating competency-based combined training between HPM and residency and fellowship programs so that trainees do not need to pursue an additional year of fellowship training (e.g., surgery-HPM). ○ Advocating for flexibility from the specialty boards to allow part-time, interrupted, and extended training schedules. ○ Crafting viable funding streams for innovative fellowships without putting accreditation or certification at risk.
While many of these efforts are underway, a cohesive and comprehensive strategy embraced and supported by HPM professional organizations would help ensure success.
The next 10 years present new and exciting opportunities to grow the field of HPM. While the challenges are significant, they are not insurmountable. The experience of HPM growth in a short time should inspire us to tackle new challenges, and to seek innovative solutions to problems faced by our field. We must build on prior successes to visualize a pathway to sustainable growth, and to best serve our patients, their loved ones, our professional societies, and one another. Workforce is not just an issue for our field. Workforce is the central issue that will define our success or failure over the next generation, and the best way to address it is through increasing the number of fellows in training and through expanded and innovative training models.
Funding Information
The authors received no financial support for the authorship and publication of this article.
Footnotes
Author Disclosure Statement
Drs. Dingfield, Jackson, Thomas, Ferris, and Radwany have no COIs to report.