
Abstract
Objective:
The article that follows is purposed at demonstrating how IT opioid plus bupivacaine achieves sustained acceptable pain relief while simultaneously rapidly reducing oral morphine equivalents (OME).
Background:
Cancer patients represent a population with significant morbidity, pain, and limited life expectancy. It is, therefore, vital to achieve satisfactory analgesia quickly and safely. To date, there is limited data in the literature that discusses efficacy of combined intrathecal (IT) medication therapy in reducing systemic opioids in the oncological population.
Methods:
This was a retrospective analysis that reviewed cancer pain patients from day of IT pump implantation through the six-month postoperative time point. A cohort of 50 oncological patients who had intrathecal drug delivery systems (IDDSs) implanted at Memorial Sloan Kettering Cancer Center between 2017 and 2019 were studied. Median OMEs were the primary modality of analysis for this review. Mean visual analogue scale scores were secondarily reviewed.
Results:
Median OMEs decreased from 503 preoperative to 105 at six months postoperative time point. Median time to discharge was 6.5 days. Unfortunately, due to malignant mortality, 27 patients did not make it to the 6-month postoperative time point.
Discussion:
IDDSs with opioid plus bupivacaine represent a safe and efficient route toward expeditious pain relief and decreased OMEs in the cancer pain population.
Introduction
In the WHO's pain relief ladder, originally designed for cancer-related pain, opioids represent the latter steps. 1 Opioids consistently provide reliable global analgesia, are easily administered, and often cheaper than alternatives.1–3 The utility of opioids is limited by their myriad side effects: gut motility slowing, pruritis, nausea, emesis, urinary retention, edema, hyperalgesia, bradycardia, sedation, sexual dysfunction, tolerance, and respiratory depression.2,4,5
Nevertheless, opioids' work and the three-step WHO ladder are effective in 80–90% of patients.1,2 In a refractory minority (2%–15%), analgesia yielded by oral (PO) opioids is either insufficient or the side effects intolerable.6,7 For these patients, intrathecal (IT) medications, through IT drug delivery systems (IDDSs), represent an attractive option in line with a proposed fourth step.7–9 IDDSs work because the proximity of the catheter tip to a central nervous receptor site provides direct longer lasting analgesia and slowed systemic absorption.5,10 As it relates to oncology, IDDSs have been shown to decrease pain and improve survival. 11
Morphine is the only opioid that is FDA approved for IT administration. 12 Other FDA-approved IT drugs include ziconotide for analgesia and baclofen purposed for spasticity. 12 Frequent off-label IT medications include hydromorphone, fentanyl, bupivacaine, and clonidine. 12
Although intrathecally administered morphine is a more receptor-targeted option than its oral counterpart, systemic absorption with dose-dependent adverse effects remains a concern. 13 For this reason, IT morphine is often combined with local anesthetic bupivacaine for superior relief. Bupivacaine is a lipophilic sodium channel blocker that preferentially blocks pain conducting fibers; however, at higher dosages, it may inhibit fibers pertaining to touch and motor function. 14 Notorious IT bupivacaine adverse effects include urinary incontinence, numbness, weakness, respiratory depression, and sympathectomy-induced hypotension.15,16
By combining morphine with bupivacaine, physicians are able to deliver analgesia with decreased dose of each, thereby limiting adverse effects.17–20 A 1996 survey demonstrated that 20% of IDDSs contained bupivacaine, whereas a 2000 study showed that 70% of pain physicians (which implanted IDDSs) had experience using morphine plus bupivacaine.21–24 For many, the addition of IT bupivacaine can significantly improve pain scores, activity, and life quality. 25 The 2012 Polyanalgesic Consensus Conference recommended IT morphine plus bupivacaine as first line for neuropathic pain and second line for nociceptive pain. 16
In the cancer population, it is vital to achieve pain relief carefully and swiftly. This is particularly true given the functional status required for continued chemotherapeutics and increased mortality. There is literature that discusses efficacy of combined IT medication in reducing systemic opioids in the oncological population. Our article is purposed at demonstrating how IT morphine plus bupivacaine achieves sustained satisfactory relief while rapidly reducing oral morphine equivalents (OMEs).
Methods
This was a retrospective analysis of cancer patients with IDDSs implanted at Memorial Sloan Kettering Cancer Center (MSKCC). It was approved through waiver for informed consent by the MSKCC IRB and supported by the MSKCC Support (P30 core) Grant and the department of anesthesiology and critical care.
All patients underwent implantation of Medtronic Synchromed™ II pumps. Live fluoroscopy was used to direct catheter tips toward sites corresponding to patients' pains as determined by MSKCC guidelines (Table 1). Postoperatively, all patients were admitted to the MSKCC hospital for dose titration. Opioid naive patients had their initial IT morphine dosing computed in a 300:1 (PO:IT) ratio, which was adjusted to 100:1 for tolerant patients.6,26,27 Few had IT hydromorphone (not morphine) that was calculated similarly. All pumps also contained 40 mg/mL bupivacaine. Patients were discharged once pain was controlled and cleared from a medical perspective. Outpatient follow-ups were scheduled for one, three, and six months postoperative time points.
Intrathecal Catheter Tip Location Based on Primary Pain Site
Charts of patients with IDDSs implanted between 2017 and 2019 were reviewed. Inclusion criteria were age >18 years, cancer-related pain, and those who received both IT opioid plus bupivacaine at IDDS implantation. Data gathered included oral morphine equivalent (OME), visual analogue scale (VAS) scores, adverse effects, and discharge time (time of IDDS implantation to discharge). OMEs did not include IT doses and were calculated using our internal MSKCC conversion chart.
Results
Between 2017 and 2019, 93 patients had IDDSs implanted at MSKCC, 50 of which contained bupivacaine plus opioid. Median age was 61 years at day of surgery, 56% were female. Gastrointestinal and breast were the most common malignancies.
Mean VAS scores decreased from 6.6 preoperative to 2.7 at discharge. Figure 1 displays the gradual decline in VAS score through six months postoperative time point.
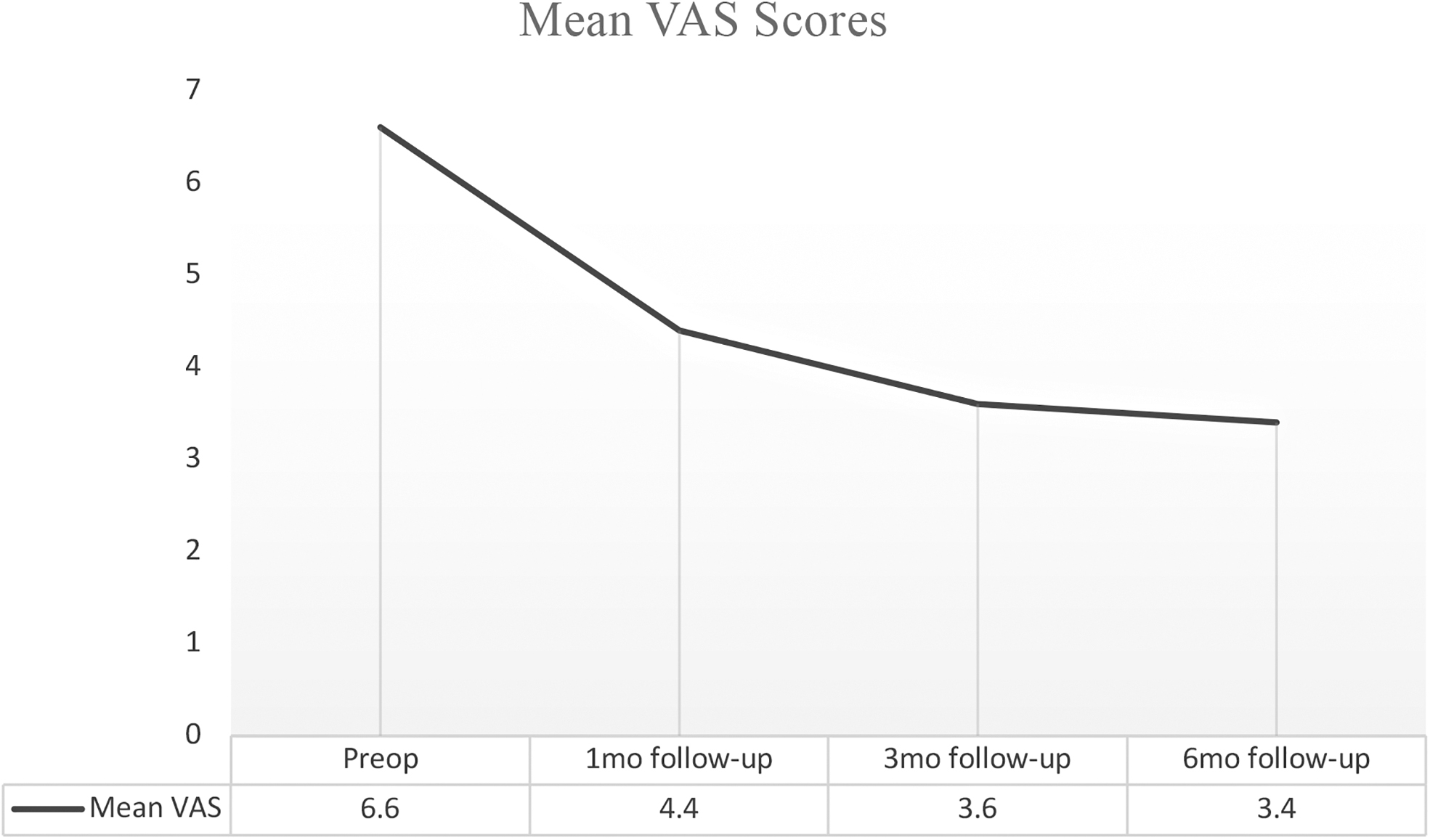
Decline in visual analogue scale pain scores status post-IDDS implantation. IDDS, intrathecal drug delivery system.
Median OMEs declined from 503 preoperative time point to 105 at discharge (Table 2). Figure 2 exhibits the swift decline in OMEs to sustained low 100s through six months postoperative time point.
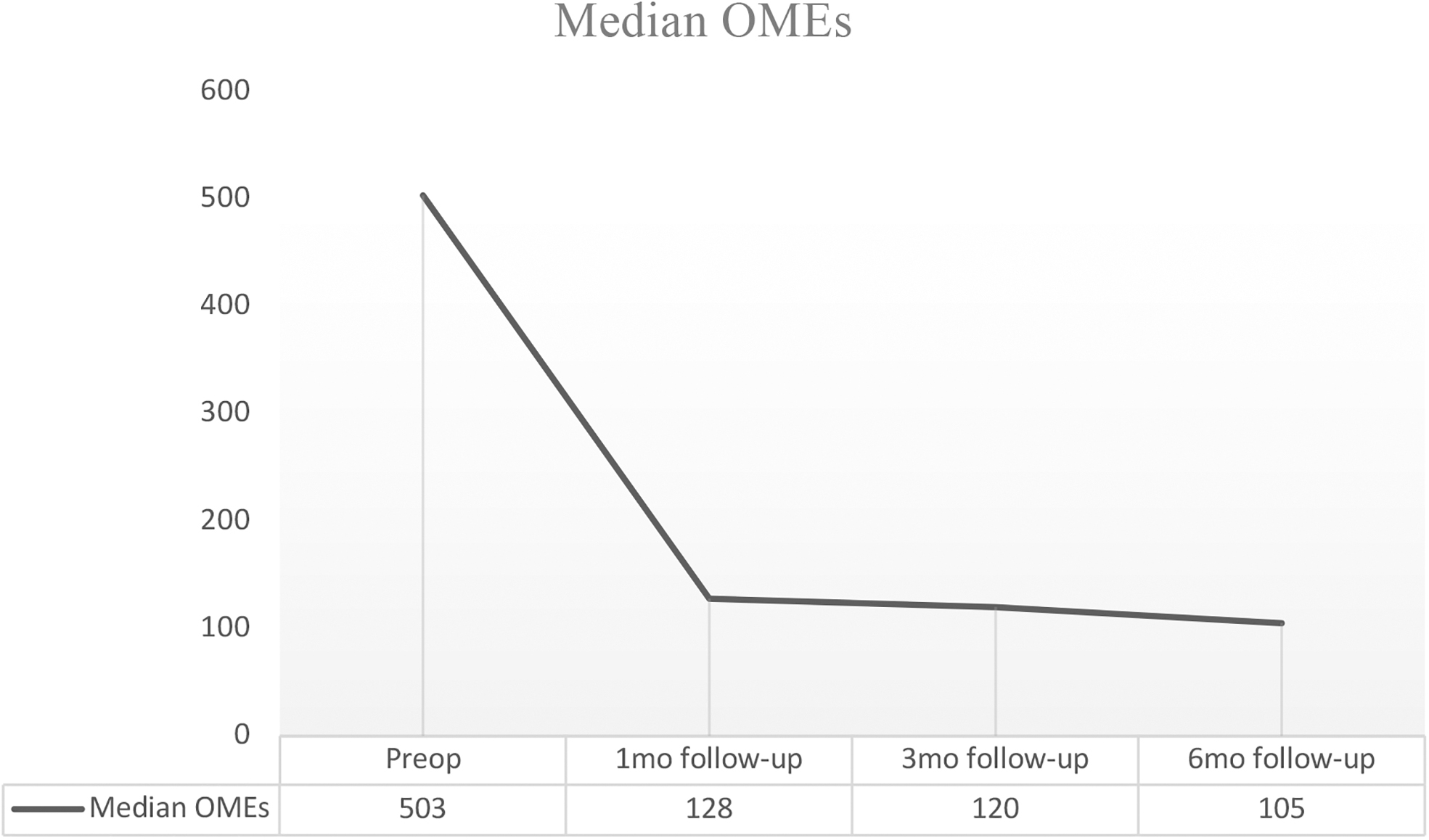
Decline in oral morphine equivalents status post-IDDS implantation.
Oral Morphine Equivalent Reduction after Intrathecal Drug Delivery System Implantation Range of Data
IDDS, intrathecal drug delivery system; OME, oral morphine equivalent.
Average discharge time varied by whether patients were admitted solely for IDDS implantation or whether they were already in-house for another reason. Mean discharge time was 6.0 days for outpatients, which increased to 10.0 days for inpatients. Stratifying patients by inpatients versus outpatients (Table 3 and Fig. 3), we appreciate how outpatients fared better.

Percentage of patients remaining on sustained release (nonintrathecal) opioids.
Comparison of Inpatients with Outpatients
Sustained release opioids include non-IT long-acting/extended-release opioids.
IT, intrathecal.
Twenty-four patients experienced adverse effects after IT pump implantation (Table 4). Throughout our cohort's hospital course and follow-up, many had oncological progression. Table 5 highlights our cohort's mortality.
Adverse Effects after Intrathecal Drug Delivery System Implantation
Deaths before Time Point Follow-Up
Discussion
This review is purposed at exhibiting our institution's experience providing sustained rapid relief through IT synergism of opioid and local anesthetic. To our knowledge, these data have not been widely reviewed despite the importance of hastened pain relief in the oncological population with limited life expectancy.
Figure 1 shows a quick decline in OMEs after IDDS implantation. We acknowledge the bump in mean three-month follow-up OMEs. In our cancer population, patients are frequently admitted for numerous reasons (disease progression, complications, and treatments) and thereby may have increased narcotic requirements. We also appreciate plateauing in median OMEs at one to six months postoperative time point. Although perhaps ideal to have patients progress to zero OMEs, most prefer to have some systemic OMEs available. This familiar crutch is comforting and at lower doses benign to our terminally ill population. In addition, because IDDS catheters deliver only localized opioid, pains at other body sites necessitate coverage.
A goal at MSKCC has been to wean patients off their non-IT OMEs in a stepwise manner (Fig. 4). Preoperatively to discharge, we were successful in cutting systemic OMEs in half in 84% of our patients (Table 3). By introducing an IT catheter corresponding to patients' most painful sites, we find it reasonable to reduce systemic opioids by ≥50%. From discharge to six months postoperative time point, we aim to eliminate (non-IT) sustained release OMEs. Thirty percent of patients remained on sustained release OMEs by six months. Outpatients often fared better because inpatients are often with acute pathophysiologies and increased pain at primary and secondary sites. Admittedly, not all patients follow our stepwise model. As everything in medicine, guidelines are offered, an individualized approach is always of utmost importance.

Percentage of patients on sustained release (nonintrathecal) opioids at each time point.
First, our data demonstrate that rapid sustained relief is possible with IT opioid–bupivacaine. This is significant in the oncological population wherein time is of utmost importance. Table 5 emphasizes how 54% did not reach six-month follow-up due to mortality. At MSKCC, we typically receive IDDS referrals when patients are nearing end of life. However, we believe that IDDSs should be considered earlier given benefits in pain relief, quality of life and long-term cost effectiveness. 28 In terminally ill patients, a pain-free few weeks or months may be very comforting. Thus, barring contraindications, IT opioid–bupivacaine should be considered.
Second, our data emphasize a swift, substantial, and lasting decline in OMEs after IDDSs are implanted and IT infusions are started with the opioid–bupivacaine combination. Median OMEs dropped 79% in six months after implantation. This implies that IT opioid is an adequate substitute for oral opioids.
Lastly, we highlight the substitution of OMEs with IT morphine–bupivacaine. This is important because although IT morphine has reduced plasma absorption compared with oral, the absorption rate is not zero. 26 That is not to say that IT bupivacaine does not have adverse effects, we know it does.15,16 However, by linking the two for continuous infusion, patients achieve relief at lower respective doses of each.
Table 4 documents our side effects post-IDDS implantation, which may have been due to morphine, bupivacaine, the procedure itself, or other (malignancy, therapeutics, and surgeries). Numbness, urinary retention, and weakness often occurred together and resolved upon decreasing bupivacaine. Adverse effects were likely unrelated to IT opioid because of its localized and minute dosing.
We acknowledge our limitations. This was a review of patients with malignant pain and, therefore, may be less generalizable. We report a sizeable dropout, but this re-emphasizes that in the terminally ill, an aggressive approach is crucial. Owing to complex pathophysiology of our population, discharge delays were rarely after postoperative time points. Although we focused on opioids and bupivacaine in isolation, we admit that this does no take into account nonopioid adjuvants.
Conclusions
IDDSs with morphine–bupivacaine represent a safe and efficient means to expeditiously reduce OMEs in the cancer pain population. Future studies should focus on the abilities of IT morphine–bupivacaine in isolation, devoid of or controlled for adjuvant pain medications.
Footnotes
Funding Information
This study was supported by Memorial Sloan Kettering Cancer Center Support Grant (P30 core grant) and the Department of Anesthesiology and Critical Care.
Author Disclosure Statement
A.G. is consultant for Medtronic, Flowonix, AIS, SPR, and Nalu.