
Abstract
Background:
Little is known about how patients with incurable cancer and caregivers differ in their prognostic awareness, and the relationship between caregiver prognostic awareness and their psychological distress.
Objective:
To investigate prognostic awareness in caregivers of patients with incurable cancer and prognostic discordance in patient–caregiver dyads and its association with psychological distress.
Design:
This is a cross-sectional study.
Setting/Subjects:
In total, subjects were 390 caregivers of adults with incurable lung, gastrointestinal, and brain cancers at a cancer center in the northeastern United States.
Measurements:
The Prognosis and Treatment Perceptions Questionnaire was used to assess prognostic awareness and Hospital Anxiety and Depression Scale to assess psychological distress.
Results:
In total, 39.7% (n = 147/370) and 17.3% (n = 64/370) caregivers reported clinically significant anxiety and depression symptoms. And 53.7% of caregivers reported the patients' cancer as “curable” and 44.1% reported the cancer was “not terminal.” Caregivers' report of curability was not associated with their anxiety (odds ratio [OR] = 0.99, p = 0.93) or depression (OR = 1.05, p = 0.32) symptoms. Among 42.5% (124/292) and 26.0% (76/292) of dyads (n = 292), both patients and their caregivers agreed in their perception of the cancer as curable and incurable, respectively. In 19.9% of dyads (n = 58), patients reported their cancer as curable, while their caregivers reported it as incurable. In 11.6% of dyads (n = 34), patients reported the cancer as incurable while caregivers reported it as curable.
Conclusions:
More than half of caregivers have misperceptions about the patients' likelihood of cure, and one-third of patient–caregiver dyads have discordant perceptions. Supportive care interventions may facilitate conversations and enhance prognostic understanding in patients with incurable cancer and their caregivers.
Introduction
Caregivers (i.e., family or friends) play a critical role in caring for patients with incurable cancer,1–9 especially as patients' needs intensify and they have diminished capacity to manage their own care and activities of daily living. 10 Many caregivers participate in medical decision making11–16 and act as decision partners, 17 particularly 13 when patients lose the ability to make their own medical decisions as their illness progresses.14,18 In the context of incurable cancer, patients must face numerous health care decisions,19,20 underscoring the important role of caregivers in the decision-making process.
Although caregivers are frequently called upon to help with patients' decision making, 21 little is known about their prognostic awareness. 22 When caregivers have an accurate understanding about prognosis, they are better positioned to help patients cope with their prognosis, participate in conversations related to goals of care, advocate for patients' best interests, anticipate the outcome of terminal illness, and make informed decisions.13,20,23–28 However, limited data have focused on caregivers' understanding of the patients' disease status. Two studies29,30 have found that caregivers are often overly optimistic about the likelihood of cure compared with the oncologists. In addition, data are also limited in identifying salient factors associated with accurate prognostic awareness in caregivers.6,31–33 Interestingly, multiple studies have shown an association between patient's accurate prognostic understanding with increased psychological distress and lower quality of life in patients with solid tumors,25,34–41 yet data exploring the relationship between caregivers' prognostic understanding and their psychological distress are lacking.6,29,42
Caregivers participate in medical decision making, thus highlighting the importance of examining whether patients and caregivers differ in their perceptions about prognosis. Existing literature has shown that patients with incurable cancer often overly overestimate their prognosis.41,43,44 Prior studies have mostly examined either patient–clinician13,45–48 or caregiver–oncologist dyads13,29,49 with limited focus on patient–caregiver dyads.11,50–53 Prior studies also lacked representation of diverse cancer types and were mostly conducted in the inpatient setting. 54 Therefore, it is important to compare prognostic awareness between patients with incurable cancer and their caregivers and its association with caregiver psychological distress in a cohort of patients with diverse cancer types.
In this study, we sought to (1) describe prognostic awareness in caregivers of patients with incurable cancer, (2) examine factors associated with caregiver prognostic awareness, with a specific interest in examining whether psychological distress is associated with caregiver prognostic awareness, and (3) investigate prognostic discordance in patient–caregiver dyads and its association with psychological distress.
Materials and Methods
Study design and procedures
We conducted a cross-sectional secondary analysis of 390 caregivers of adults with incurable lung, gastrointestinal, and brain cancers who were previously enrolled in supportive care studies at the Massachusetts General Hospital (MGH) Cancer Center between May 2011 and November 2018.6,55–58 Caregivers completed questionnaires that asked about their sociodemographic data, perceptions of the patients' prognosis, and caregiver psychological distress. We used the same measures, eligibility criteria with regard to advanced stage cancer, and recruitment processes across three studies and collected them at a minimum of six weeks since the patients' diagnosis of incurable cancer, which allowed us to combine their data for this secondary cross-sectional analysis.
If the caregivers were participating in a supportive care intervention trial, we utilized their baseline data before randomization and intervention delivery. All studies included in this secondary analysis enrolled eligible caregivers who provided informed consent. Our study was approved by the Dana-Farber/Harvard Cancer Center Institutional Review Board.
Study sample
The study included caregivers of adult patients (≥18 years of age) with a new diagnosis of incurable lung, gastrointestinal, and brain cancers and who received care at MGH Cancer Center at the time of enrollment.25,35,59,60 Incurable disease was defined based on treatment intent as documented in the electronic health record and confirmed with the treating oncology clinician. Enrolled patients identified caregivers as relatives or friends who provided them with support and had in person contact with the patient at least twice weekly. 61 Caregivers were eligible if they were ≥18 years old and had the ability to read and respond to questions in English or complete questionnaires with minimal assistance from an interpreter. We excluded patients with significant psychiatric or other comorbid diseases, which the treating clinician believed prohibited informed consent or participation in the study.
Study measures
Sociodemographic and clinical characteristics
Caregivers completed a baseline demographic questionnaire that included age, gender, race, ethnicity, education, marital status, employment, and relationship with the patient. We obtained data on the patients' cancer diagnosis and stage of disease from the electronic medical record.
Prognostic awareness
We administered items from the Prognosis and Treatment Perception Questionnaire to assess patients' and caregivers' baseline prognostic awareness, a measure that has been used in prior studies.25,35,62,63 Specifically, we asked participants to report to what extent they perceive the patients' cancer as curable. Participants rated the likelihood that the cancer was curable on a 7-point scale (ranging from “no chance/0% chance” to “extremely likely/>90% chance”). 25 Consistent with prior research,41,64 we dichotomized responses as incurable (i.e., “no chance” to “unlikely chance”) versus likely to be cured (e.g., “somewhat likely” to “extremely likely”).
We also asked participants to describe the patient's current health status by choosing from the following mutually exclusive options: “relatively healthy,” “relatively healthy and terminally ill,” “seriously ill and not terminally ill,” or “seriously ill and terminally ill.” 35 Consistent with prior research,25,35 we categorized responses as either “terminally ill” or “not terminally ill.”
Similar to a prior study, 6 we considered the response “the patient's cancer was curable” to denote inaccurate prognostic understanding and “the patient's cancer was incurable” as accurate prognostic understanding. Concordant beliefs occurred when both members of the patient–caregiver dyads agreed on perceptions of curability—whether accurate or not. Discordant beliefs occurred when one member of the dyad had a different perception of curability about the patient's cancer than the other member. We categorized dyads as either having a concordant and accurate prognostic understanding if their responses were concordant or they both agreed that the patient's cancer was incurable.
Anxiety and depression symptoms
We measured caregivers' anxiety and depression symptoms using the 14-item Hospital Anxiety and Depression Scale (HADS), a measure with strong psychometric properties in samples of adults with cancer and their caregivers.25,56,65–69 The HADS consists of two subscales assessing anxiety and depressive symptoms in the past week, with subscale scores ranging from 0 (no distress) to 21 (maximum distress).25,62,65
Statistical analysis
We computed descriptive statistics to describe the caregiver characteristics, including means or medians for continuous variables depending on the normality of the data, and proportions for categorical variables. To examine factors associated with accurate caregiver prognostic awareness and acknowledgment of terminal illness, we performed logistic regression models and incorporated variables identified a priori based on prior literature including age, gender, race, education, employment, religion, relationship with patient, anxiety and depression symptoms (continuous variables), and patients' cancer diagnosis. We used McNemar's test to compare perceptions of cure within patient–caregiver dyads. We conducted multivariable linear regression models to assess the independent associations of caregiver prognostic discordance with caregiver distress. A two-sided p-value <0.05 was considered statistically significant and we performed all statistical analyses using STATA version 15.0.
Results
Sample characteristics
Table 1 depicts sample characteristics. The study included 390 caregivers of patients with a diagnosis of incurable lung (n = 203, 52.1%), gastrointestinal (n = 126, 32.3%), or brain (n = 61, 15.6%) cancer. The median age for caregivers was 59 years old [range 19–86], and the majority was white (n = 363, 93.1%) and female (n = 263, 67.4%). Caregivers most commonly identified themselves as partners or spouses of the patient (n = 270, 69.2%). Over half (n = 214, 54.9%) of the caregivers reported their employment as currently working part- or full-time and 46.7% (n = 182) had at least a college degree. Among caregivers who reported data on psychological distress, 39.7% (147/370) reported clinically significant anxiety symptoms and 17.3% (64/370) reported clinically significant depression symptoms.
Baseline Characteristics of Caregivers of Adults with Incurable Cancer (n = 390)
Rates and correlates of caregiver prognostic awareness
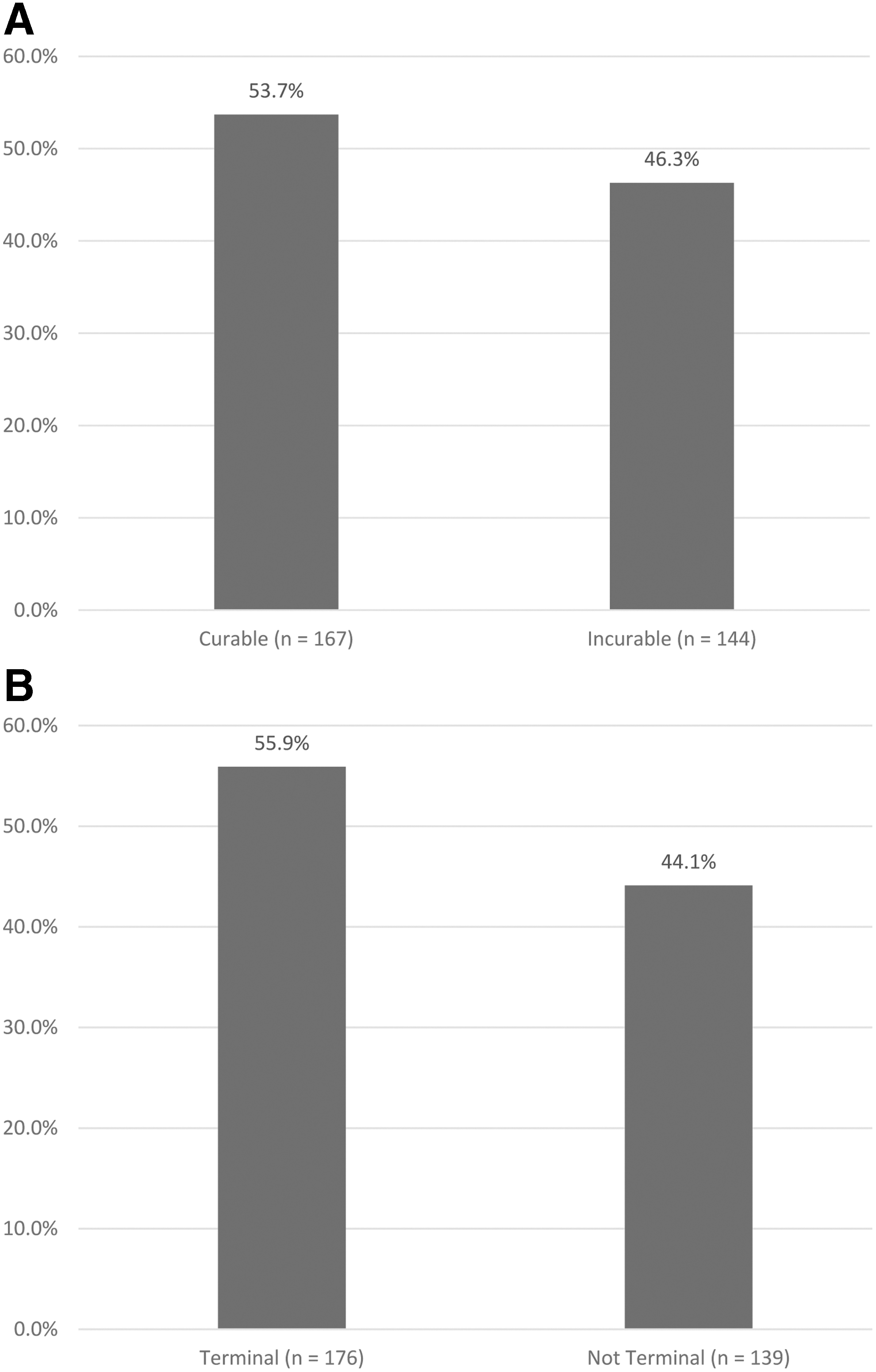
Over half of the caregivers (53.7%, 167/311) reported that the patients' cancer was curable (Fig. 1A) and 44.1% (139/315) reported the patients' cancer was “not terminal” (Fig. 1B). Table 2 presents a cross-tabulation of perceptions of curability and acknowledgment of terminal illness. We examined associations between caregiver factors and their report of curability (Table 3). White caregivers were more likely to perceive the patient's cancer as incurable (odds ratio [OR] = 3.69, p = 0.03) compared with nonwhite caregivers. We found no significant associations between the caregivers' report of curability and their age, gender, education, employment, religion, relationship with patient, and patient's cancer diagnosis. Caregivers' report of curability was not associated with their anxiety (OR = 0.99, p = 0.93) or depression symptoms (OR = 1.05, p = 0.32) (Table 3). We then examined associations between caregiver factors and their acknowledgment of terminal illness (Table 4). Older caregiver age (OR = 1.03, p = 0.048), female caregivers (OR = 0.52, p = 0.019), white caregivers (OR = 3.06, p = 0.038), those who are children of patients compared with partners (OR = 2.95, p = 0.03), and caregivers of patients with gastrointestinal cancer compared with lung cancer were more likely to acknowledge the patient's cancer as terminal. Caregivers' acknowledgment of terminal illness was not associated with their anxiety (OR = 1.02, p = 0.52) or depression symptoms (OR = 1.04, p = 0.44).
Caregivers' Perception of Curability and Acknowledgment of Terminal Illness
Caregiver Factors Associated with Perceptions of Curability in Caregivers of Patients with Incurable Cancer (n = 275)
p < 0.05 is considered statistically significant.
CI, confidence interval; OR, odds ratio; SE, standard error.
Caregiver Factors Associated with Acknowledgment of Terminal Illness in Caregivers of Patients with Incurable Cancer (n = 277)
p < 0.05 is considered statistically significant.
Prognostic discordance in patient–caregiver dyads and psychological distress
We found significant discordance in report of curability in patient–caregiver dyads (p = 0.016), with >30% of the dyads (92/292, 31.5%) reporting discordant perceptions of prognosis (Fig. 2). Specifically, in 19.9% (58/292) of dyads, patients reported their cancer as curable while their caregivers reported the cancer was incurable. Among 11.6% (34/292) of dyads, patients reported the cancer as incurable while their caregivers reported the cancer as curable. Finally, among 42.5% (124/292) and 26.0% (76/292) of dyads, both patients and their caregivers agreed in their perception of the cancer as curable and incurable, respectively.
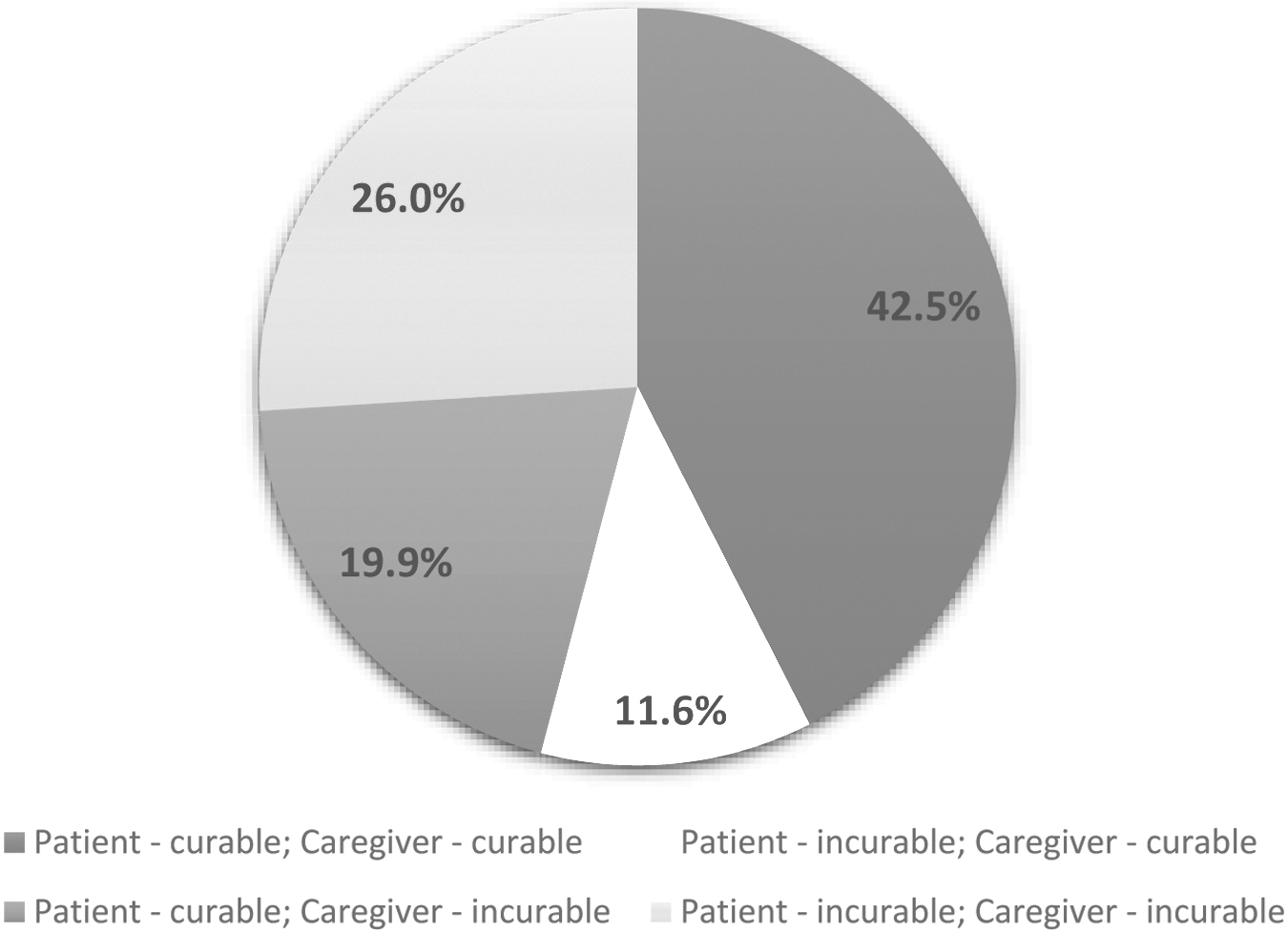
Caregivers' and patients' perceptions of curability within dyads (n = 292).
In the adjusted analyses, there was no association between patient–caregiver discordance in perception of cure and caregivers' anxiety (B = 0.33, p = 0.54) or depression (B = −0.07, p = 0.86) symptoms. We found significant discordance in report of terminality in patient–caregiver dyads (p < 0.001), with 35.7% of dyads (105/294) reporting discordant beliefs of terminality (Fig. 3). Specifically, in 24.8% (73/294) of dyads, patients reported their cancer as nonterminal while their caregivers reported the cancer was terminal. Among 10.9% (32/294) of dyads, patients reported the cancer as terminal while their caregivers reported the cancer as nonterminal. Finally, among 30.6% (90/294) and 33.7% (99/294) of dyads, both patients and their caregivers agreed in their perception of the cancer as terminal and nonterminal, respectively. In the adjusted analyses, there was no association between patient–caregiver discordance in acknowledgment of terminal illness and caregivers' anxiety (B = 0.04, p = 0.95) or depression (B = 0.04, p = 0.92) symptoms.
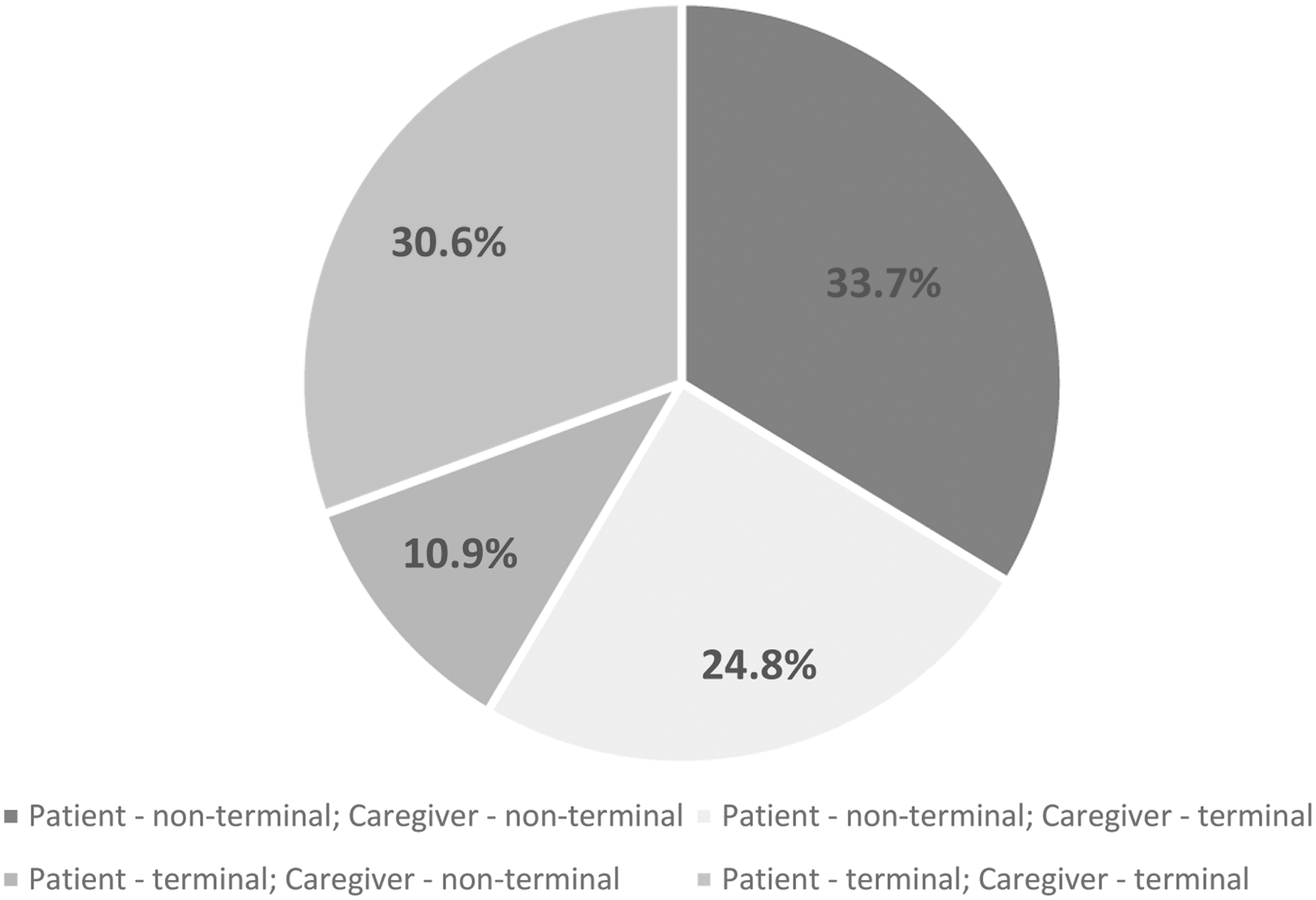
Caregivers' and patients' perceptions of terminality within dyads (n = 294).
Discussion
In this study, we found that over half of caregivers (53.7%) reported misperceptions about the patients' likelihood of cure with a high proportion (44.1%) also reporting their cancer was nonterminal. Caregiver race was the only variable associated with caregivers' report of curability, whereas other factors including age, gender, and caregivers' depression and anxiety symptoms were not associated with this measure. Prior research has shown that racial and cultural disparities exist in prognostic understanding among patients with cancer, with Hispanic and black patients less likely to acknowledge their terminal prognosis,70,71 less likely to accurately estimate their survival, 72 and report being unaware or prefer not to know their prognosis73–75 compared with whites. Given the unique cultural and racial backgrounds of our patients, there is a pressing need to understand and address racial and cultural disparities in prognostic communication and illness and prognostic understanding in caregivers of patients with cancer.34,72 Notably, a substantial minority of patient–caregiver dyads (31.5%) reported discordant understanding of the likelihood of cure. These findings underscore the need for interventions to improve both patients' and caregivers' prognostic awareness to support patients and families as they face difficult medical decisions. As most care decisions are made within the context of family care and obligation, 76 understanding family member views in a dyadic context is critical in developing communication strategies for harmonious decisions. 33 Recent studies have examined relationships between patient–caregiver concordance and outcomes such as advance care planning and hospice enrollment,33,51,77 and more work in this area is needed.
Although prior studies have primarily focused on highlighting prognostic misperceptions among patients with advanced cancer, 35 our findings demonstrate that these misperceptions are also prevalent among caregivers. In a prior study of 317 patients with advanced cancer and their caregivers in Australia, 52% of caregivers had misperceptions regarding the goal of treatment for the patient. 78 Although over half of caregivers in our study reported the patients' cancer as curable, 55.9% also acknowledged the patients' cancer as terminal. Despite acknowledging the terminal nature of the cancer, caregivers were still hoping for the possibility of a cure, likely highlighting their internal conflict in accepting their loved ones' prognosis. 79 Another possible explanation may be that patients and caregivers do not interpret the terms “curable” and “terminal” in the same way as health professionals.
It remains unclear to what extent caregivers' prognostic awareness and acceptance of the patients' prognosis impact medical decision making. Longitudinal studies are needed to elucidate further caregivers' prognostic awareness and its association with medical decision making, particularly at the end of life. Furthermore, the issue of understanding concordance or discordance between patients and caregivers is relevant for cancer clinicians, especially within families wherein caregivers are highly engaged in care and decision making. 33
Although patients with advanced cancer who accurately perceived their cancer to be incurable reported higher distress in prior studies,25,35–37 we did not identify an association between caregivers' report of the patients' likelihood of cure and their anxiety or depression symptoms. Given the large sample size in this study, these findings are noteworthy and clinically relevant as they suggest that many caregivers may not experience psychological distress to the same extent as patients when accurately understanding the patient's prognosis. Thereby, caregivers may be better positioned to receive prognostic information and engage in early discussions about clarifying prognostic understanding and expectations in the context of incurable cancer without adding unwanted psychological distress.
In our study, only one-fourth (26.0%) of patient–caregiver dyads agreed that the patients' cancer was incurable, further underscoring the extent of prognostic misperceptions among patients with advanced cancer and their caregivers. In fact, approximately one-third of patient–caregiver dyads reported discordant perceptions of the patient's prognosis. Discordance between patients and their caregivers with respect to their understanding of prognosis is critical to address, especially as caregivers are increasingly asked to help make decisions on behalf of the patient at the end of life. Discordance in prognostic awareness may be due to a number of reasons, including the inability to fully process the prognostic information32,80,81 or misinterpretation of the information to be more positively than it was intended.32,82,83 A possible explanation could be that one member of the dyad may face these challenges while the other member may not.
In addition, there is little evidence to support whether it is more ideal for members of a dyad to be concordant and inaccurate or discordant in their beliefs about perceptions of curability. We hypothesize that prognostic discordance may lead to conflict within the dyad, whereas concordant yet inaccurate perceptions may result in difficulty making decisions at the end of life. However, further research is needed to fully understand the clinical implications of having dyads with discordant beliefs or dyads with concordant and inaccurate perceptions of curability. In this study, 31.5% of dyads had discordant beliefs about perceptions of curability, and these findings highlight the importance of improving prognostic communication and understanding as well as underscore the need to further explore the potential role of palliative care in these dyadic discussions about prognosis.13,64 Therefore, future interventions that facilitate effective communication between patients, caregivers, and clinicians may help harmonize these discrepancies and ensure an effective decision-making process throughout the cancer illness trajectory.
This study has several important limitations. First, we conducted this study using data collected at a single cancer center. The sample comprised a highly educated caregiver population with limited racial diversity, which may limit the generalizability of our findings to caregivers from other racial and ethnic backgrounds, who live in other geographic areas, and who report lower educational attainment. Second, given the cross-sectional nature of this study, we are unable to determine the directionality, temporality, and sensitivity to change over time between caregiver prognostic awareness and psychological distress. Patients in this sample were only recently diagnosed with incurable cancer; therefore, caregivers' perceptions of the patients' prognosis may change over time. Third, as this is a secondary data analysis, the findings should be considered hypothesis generating and exploratory. Fourth, we did not capture other factors that may impact caregivers' prognostic awareness such as caregivers' mental health history or coping strategies. Lastly, we did not have information to include about the maximum time from diagnosis to explore whether it could have implications for both prognostic understanding and distress.
Discussions of diagnosis, treatment options, and prognosis are an inevitable component of cancer care, and caregivers play a critical role in medical decision making for patients with incurable cancers. However, few caregivers of patients with incurable cancer have a full accurate understanding of the patients' condition. Our study findings highlight the extent of prognostic misperceptions among caregivers of patients with incurable cancer, and future studies are needed to confirm our findings related to the association between patient–caregiver prognostic discordance and caregiver distress.
Furthermore, consistency across measures for prognostic understanding is critically needed and these measures should be studied across racially and ethnically diverse groups. 34 Future research efforts should also identify the optimal timing and approach to deliver prognostic information to caregivers, incorporate qualitative methods such as videoethnographic studies to understand the gaps in patient–caregiver–physician communication, and develop and validate prognostic prediction models and decision aids to help promote a family-centered approach to shared decision making. 34 In addition, our findings underscore the resilience of caregivers in processing prognostic information given that those who have an accurate understanding of the patients' prognosis do not report increased anxiety or depression symptoms. Although our study did not show associations between prognostic understanding and caregiver distress, supportive care interventions for patients with incurable cancer and their caregivers are still needed to facilitate conversations about prognosis, enhance prognostic understanding within dyads, and guide informed treatment decision making.
Footnotes
Acknowledgments
We thank all of the patients and their caregivers for dedicating their time to this research.
Authors' Contributions
Conception and design, acquisition of data, or analysis and interpretation of data; drafting of the article or critical revision of the article for important intellectual content; approval of the article; and accountability for all aspects of the work were carried out by T.F.G., D.F., R.D.N., J.A.G., J.S.T., and A.E.-J.
Funding Information
This study was funded by K24 CA181253/CA/NCI NIH HHS/United States (PI: J.S.T.) R01 NR012735/NR/NINR NIH HHS/United States (PI: J.S.T.) and Leukemia and Lymphoma Society Clinical Scholar Grant (PI: A.E.-J.).
Author Disclosure Statement
J.S.T. receives research funding from NCCN/Pfizer and J.A.G receives research funding from NCCN/Pfizer, royalties from edited volume from Springer (Humana Press), and research funding from Gaido/BCG Digital Ventures, and is a consultant at Concerto Health AI.