
Abstract
Objectives:
Determine feasibility, acceptability, and preliminary effects of the Palliative Care Social Worker-led ALIGN (Assessing & Listening to Individual Goals and Needs) intervention in older persons admitted to Skilled Nursing Facility (SNF) and their caregivers.
Design:
A pilot pragmatic randomized stepped wedge design of ALIGN versus usual care in three SNFs.
Setting and Participants:
One hundred and twenty older adults and caregivers (optional) with advanced medical illnesses.
Measures:
Primary outcomes were feasibility and acceptability. We collected exploratory patient-/caregiver-centered outcomes at baseline and three months and conducted a medical record review at six months to assess documentation of Advance Directives (AD). We also collected exploratory health care utilization data, including hospitalizations, mortality, and hospice utilization.
Results:
Of 179 patients approached, 120 enrolled (60 ALIGN patients with 15 caregivers and 60 usual care patients and 21 caregivers). Four intervention patients refused ALIGN visits, 8 patients died or discharged before initial visit, and 48 intervention patients received ALIGN visits, with ∼80% having caregivers participating in visits, regardless of caregiver study enrollment. Quantitative exploratory outcomes were not powered to detect a difference between groups. We found 91% of ALIGN patients had a completed AD in medical record compared to 39.6% of usual care patients (p < 0.001). Qualitative feedback from participants and SNF staff supported high acceptability and satisfaction with ALIGN.
Conclusion and Clinical Implications:
A pragmatic trial of the ALIGN intervention is feasible and preliminary effects suggest ALIGN is effective in increasing AD documentation. Further research is warranted to understand effects on caregivers and health care utilization. The current model for SNF does not address the palliative care needs of patients. ALIGN has potential to be an effective, scalable, acceptable, and reproducible intervention to improve certain palliative care outcomes within subacute settings.
Introduction
Of the nearly 800,000 seniors admitted to Skilled Nursing Facilities for rehabilitation (SNF rehab) annually in the United States, ∼20% will be newly institutionalized, 25%–50% are readmitted back to the hospital within 30 days at a cost of $4.34 billion, and 9% will die in the next year.1–5 Over 10% of Medicare decedents will have been admitted to hospital, SNF rehab, and back to hospital in the year before their deaths, yet goals of care or the possibility of death are often unaddressed.6,7 While the purpose of a short rehabilitation stay may at first glance seem at odds with a palliative approach, this time of transition represents an ideal opportunity to re-examine goals of care for the older adult with multimorbidity. All too often, patients with poor rehabilitation potential are discharged from the acute care hospital to an SNF rehab facility because they are not safe to go home and lack other options. 5 Hence, on closer examination, this population represents an ideal target for palliative care interventions such as symptom management, decreasing caregiver distress, and ensuring that the medical care provided is congruent with patient goals and preferences. Yet due to current Medicare reimbursement models, palliative care has poor penetration in the SNF rehab setting and health professionals working in the SNF rehab setting are rarely trained in palliative care. Additional barriers to SNF rehab staff engaging in palliative-focused discussions include a lack of time and focus on the next care transition.5,8–10 Therefore, there is an immediate and unmet need in the SNF rehab setting for facilitating alignment in patient, caregiver, and provider goals of care and ensuring patient's goals and values align with the medical care possible. 11 Furthermore, these discussions must be effectively communicated across care settings (primary care, SNF rehab, community home health, or hospice) to ensure goals of care are concordant with the treatment being offered and provided.
Palliative care social workers are uniquely positioned to address these unmet needs by addressing the bio-psycho-social-spiritual aspects of illness. The ALIGN (Assessing & Listening to Individual Goals and Needs) intervention was developed and is led by a collective of palliative social workers (The Holding Group) and focuses on identifying patient and caregiver goals and values, facilitating communication between the patient and the care team, and, in collaboration with the patient's primary health care team, providing education about disease trajectory, and developing a patient-centered care plan that accompanies the patient across all future transitions. 12 ALIGN was previously tested in a long-term acute care hospital (LTACH) setting as part of a quality improvement project that demonstrated 15% lower rates of hospital readmissions, 30% greater use of hospice, improved self-reported patient care experience, and 60% higher levels of advance directive completion. 13 We sought to determine the feasibility and acceptability of the ALIGN intervention in the SNF setting by conducting a pragmatic step wedge pilot study. We also sought to explore the preliminary effects of the ALIGN intervention on patient- and caregiver-centered outcomes, as well as health care utilization patterns.
Methods
Sample
Participants were members of an integrated health care system and recruited from 3 community SNFs in the greater metro area. Patients were eligible if they were ≥65 years of age, LACE score >7 (
Study design
This study utilized a stepped wedge design with each SNF rehab enrolling 20 participants in the usual care phase followed by 20 participants in the intervention phase. This design was selected over a randomized controlled trial to address concerns for contamination within the sites. Based on the study design, blinding was not possible. The primary aim of the study was to determine the feasibility of the study design and intervention delivery. Members of the research team (principal investigator [PI], project manager, research coordinator, and palliative care-trained social workers [PCSWs]) met with SNF rehab staff before enrollment started to build rapport and learn facility work flow, schedule, and culture. The research team represented a major referring partner of the participating SNF rehabs, which helped our team gain entrée and engage facility staff. Feasibility assessment included the number of eligible patients, those approached and enrolled. We assessed the number of patients who were able to complete the intervention and reasons if not. Finally, we assessed the proportion of enrolled patients who subsequently completed follow-up patient- and caregiver-centered measures. This study was approved and overseen by the health care system's Institutional Review Board.
Intervention
The ALIGN intervention was developed by The Holding Group, an independent partnership of PCSWs. The intervention is theory driven, utilizing an ecological approach that incorporates family systems theory, considering the interactions of both patient and caregiver.15,16 The intervention is patient/caregiver centered, addresses palliative care and psychosocial issues, and integrates with health care teams. The ALIGN intervention provides psychosocial care that targets communication, goal alignment, and caregiver support. The PCSW makes an initial in-SNF visit with the patient and caregiver completing a comprehensive clinical assessment that guides future intervention visits. All patients are followed from enrollment at SNF admission, through the SNF stay, and for 45 days after SNF discharge. Follow-up visits (approximately two to four visits every two to three weeks depending on needs) are in person and by phone. The number and duration of all contacts are tracked. Intervention overview can be found in Table 1.
Assessing & Listening to Individual Goals and Needs Intervention Components
ALIGN, Assessing & Listening to Individual Goals and Needs; SNF rehab, Skilled Nursing Facilities for rehabilitation.
Patient-centered measures
We used the Functional Assessment Cancer Therapy-General (FACT-G) to assess overall quality of life. 17 This measure includes subscales of physical well-being, social well-being, emotional well-being, and functional well-being. Patients completed a sociodemographic survey, including detailed information on gender, marital status, income, education, and employment. Caregivers completed the Caregiver Reaction Assessment (CRA), a validated measure of both burden and benefit finding associated with caregiving and the Zarit Caregiver Burden survey, measuring caregiver burden.18,19 Both patients and caregivers completed the Advanced Illness Coordinating Care Survey (AICCS), a survey that measures perceived illness understanding and coping support subscale. 20 This subscale measures how effectively professionals communicate with patients/family about their illnesses, prepare them for illness sequelae, and assist them in coping with illness. We conducted chart reviews to assess completion of advance care planning document(s). We also examined health care utilization, including subsequent hospitalizations, mortality, and referrals to hospice programs and length of stay in hospice for participants and for those who met eligibility criteria, but who were not approached for study participation. To assess the acceptability of the intervention, we completed qualitative interviews with a subsample of the intervention phase patients and caregivers using a semistructured interview guide based on a phenomenological approach. 21 The primary focus of the interviews was to understand patients' and caregivers' experience related to perceptions of and meaning assigned to the ALIGN intervention.
Data collection
Research team members collected baseline measures from all patients and participating caregivers following consent. Study personnel surveyed patients two months after enrollment to complete the patient- and caregiver-centered measures. Chart review was conducted by study PI (S.M.F.) and Co-I (E.J.) to assess for the presence of advance care planning documentation within the electronic health record. Health care utilization data were administratively extracted by a statistician (C.R.). Qualitative interviews were conducted by study team members and recorded and then transcribed verbatim. To be eligible for the qualitative interviews, patients must have received and completed the intervention with The Holding Group and completed the follow-up quantitative survey. Qualitative interviews were completed with a convenience sample of seven patients and caregivers. Six interviews were conducted (one caregiver and patient were interviewed together). Study team also met with SNF rehab staff as a group at the completion of the intervention phase to informally debrief the implementation of the intervention within the facility. Written notes were taken at these sessions.
Analysis
Survey data were collected through REDCap and patient health care utilization data were obtained from the health care system's Virtual Data Warehouse. Data were analyzed using SAS, v.9.4 from the SAS Institute, Cary, NC. Analyses consisted of descriptive statistics and t tests for continuous level data, testing for differences in outcomes of interest between the Align, usual care groups, and the not approached group for utilization outcomes.
All qualitative interviews were, on average, one-hour long, transcribed verbatim. Data were organized and reviewed using a basic content analysis approach by coding responses and then identifying themes by two members of the research team. 22 Information gathered in memos and notes were also considered. Codes were reviewed and organized into themes by two members of the research team. The primary focus of the analysis was to understand patients' and caregivers' perception of the ALIGN intervention.
Results
Feasibility outcomes
We screened all health care system members admitted to the participating SNF rehabs within the study time frame and identified 469 patients meeting eligibility criteria. Due to limited staffing time and the location of the SNF rehabs, study staff were only able to enroll patients one to two days a week. Therefore, they were only able to approach 179 of the potentially eligible patients for study participation, with 120 agreeing to participate, resulting in a 67% enrollment rate. One person in each group formerly withdrew from the study resulting in a final sample of 118 patients, 59 in each group. Follow-up interviews were difficult in this population with earlier rates of follow-up data capture to be low, improving over time as we implemented additional strategies to successfully complete follow-up, detailed in Figure 1. A total of 21 caregivers enrolled in the usual care phase and 15 caregivers enrolled in the ALIGN intervention phase. The majority of usual care phase caregivers were spouses (73%) versus adult child (20%) where they were more evenly split for ALIGN phase caregivers (43% spouse and 43% adult child). See Figure 1 for the consort diagram.
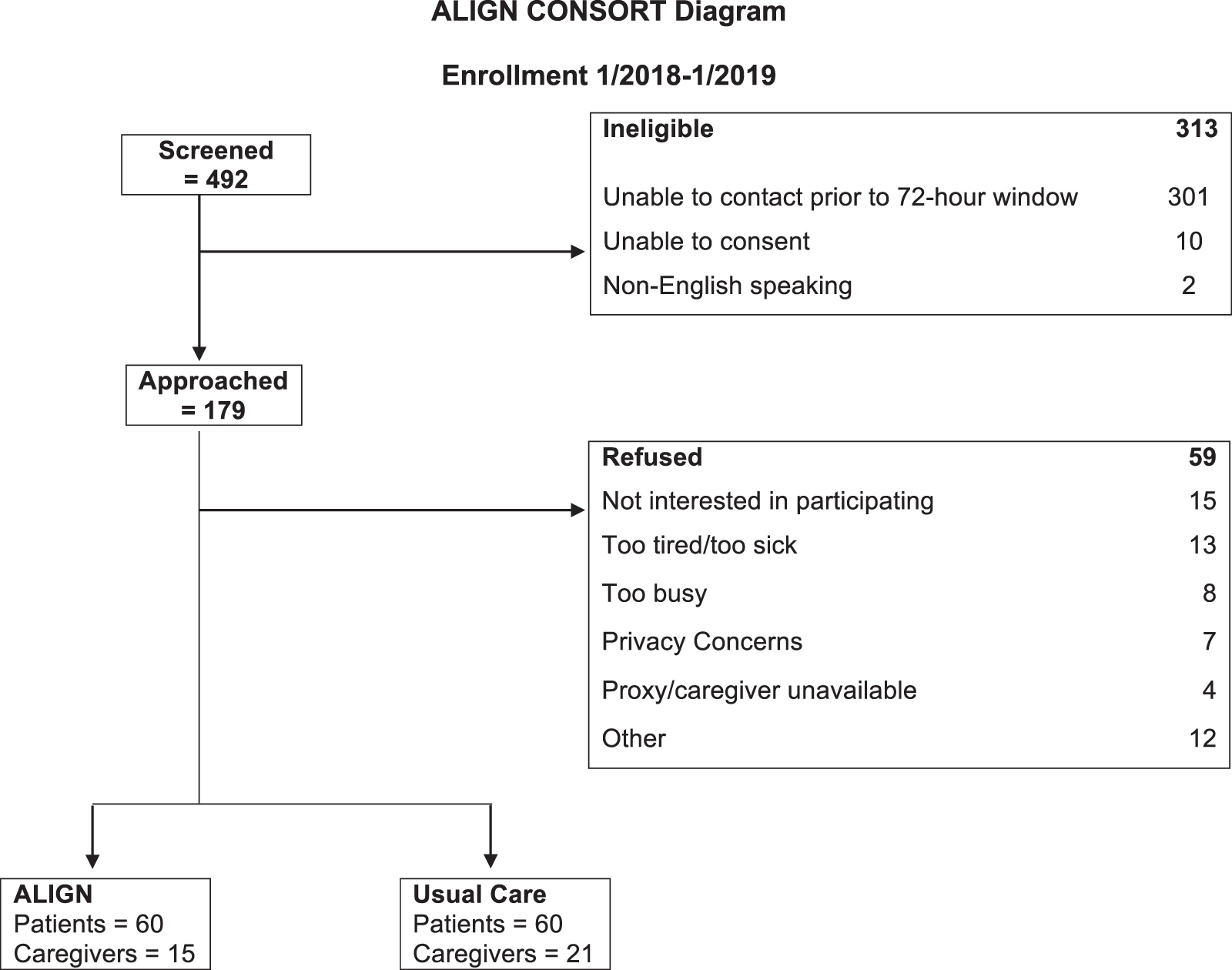
ALIGN Consolidated Standards of Reporting Trials (CONSORT) diagram. ALIGN, Assessing & Listening to Individual Goals and Needs.
Participants
The overall sample consisted of slightly more female patients (61%) with a mean age of 80.3 (±7.8 standard deviation [SD]). The majority of participants were non-Hispanic white, and similar to the group that was never approached. The mean LACE score was 10.8 (±2.8 SD). The majority of participants were either married or widowed and were above the poverty level. Participants were mainly retired and the majority had at least some college. See Table 2 for detailed descriptive statistics of participants who enrolled and those who were not approached.
Description of Enrolled Sample and Not Approached at Baseline, n (%)
SD, standard deviation.
Intervention delivery
Of the 60 patients enrolled in the intervention arm of the study, 48 received the intervention. Four persons refused visits from The Holding Group PCSWs. The other eight patients were either discharged (n = 6) or died (n = 2) before a PCSW was able to approach patients for intervention visits. The average number of face to face visits for the 48 patients who participated in the intervention was 2, and the last visit patients received was after discharge from SNF rehab. As mentioned, in addition to face to face visits, the ALIGN protocol includes periodic phone outreaches to patients and/or caregivers. In over 90% of the patients who received the intervention, their caregivers were involved in these visits and/or their care, although most of these caregivers were not formally enrolled as caregivers in the study.
Patient and caregiver centered outcomes
While this study's primary outcome was that of feasibility, we collected patient- and caregiver-centered outcomes to explore effects of the ALIGN intervention in this population. While we were not powered to see any statistically significant difference between the two groups, our findings may help guide and inform future outcomes. Patient-reported outcomes did not suggest that the ALIGN intervention had an impact on quality of life (FACT-G) or patient-perceived communication (AICCES). Advance care planning documentation was significantly different between the ALIGN intervention participants (65.3%) and usual care phase patients (34.7%) at baseline with a p-value = 0.006. At follow-up, 91% of ALIGN intervention participants had advance care planning (ACP) documentation completed in the medical record compared to 39.6% of usual care phase participants with a p-value <0.001. Despite the small numbers, the CRA scale suggested improved burden/benefit and meaning for caregivers in the ALIGN intervention (change in score +4.5 [±5.4]) compared to caregivers of usual phase patients (change in score −1.4 [±5.3]) with a p-value 0.057. Change in caregiver burden (Zarit) and the caregiver AICCES score was not significantly different between the groups (Table 3).
Participant and Caregiver Outcomes
AICCES, Advance Illness Coordinating Care Experience Survey; FACT-G, Functional Assessment Cancer Therapy-General.
Health care utilization
Again, this study was not powered to detect significant differences between the groups. Rehospitalization rates were similar among the ALIGN (18.6%), usual care (20.3%), and not approached groups (22.4%), p-value is not significant. Eleven ALIGN patients died in the follow-up period (18.6%) with seven enrolled in hospice before death for a mean of 40 days (SD ±45.6). In the usual care group, 4 patients died (6.8%) with 3 enrolling in hospice before death for a mean of 22 days (SD ±23.6), and 51 patients died in the not approached cohort (17.6%), with 36 patients enrolling in hospice before death for a mean of 36 days (SD ±50.5). These results were not powered to detect significant differences and the numbers were small (Table 4).
Utilization Outcomes for Patient Participants for the Six Months before Enrollment (Baseline) and the Six Months following Enrollment (Follow-Up)
Qualitative feedback
Study staff debriefed with SNF rehab staff (specifically nurse managers and social services) following intervention phase. Overall, the feedback was very positive. Although one of the SNF rehab SW expressed frustration that the ALIGN intervention team would only see study patients, suggesting the intersection between the community SNF rehab setting and research can itself be complicated by misaligned goals. All the SNF rehab sites participating in the study have agreed to be sites in future trials of the ALIGN intervention. When asked what elements of the intervention the SNF rehab staff were able to incorporate into their own usual practice, responses were consistent. Staff stated that they did not have the time. Exemplars: “No time to even read the chart from the hospital, the job is about safe discharge,” and “None of us have more than 12 minutes to see a patient.”
The research team contacted nine patients and two caregivers. Two patients died before being contacted, two were too confused, and two were too ill to complete the interview. Five patients and two caregivers completed qualitative interviews, providing in-depth perspective on the effects of ALIGN. Results supported acceptability and satisfaction with the intervention, although challenges interviewing such a medically vulnerable population were apparent. Patients and caregivers found the education and “outside help” provided by the ALIGN team valuable. They noted ease of interactions, appreciation of feeling heard, and empowered to make decisions based on their needs (vs. needs of others). “She gave us education [about future planning regarding Parkinson's disease]. Helping us understand the Medicaid Benefit was huge. Everything went really smooth. She made it easier for us.” Another patient stated “I was ignorant of the whole breadth of the social worker profession” before she met the ALIGN team and indicated she appreciated the support to help her with her care goals.
Discussion
In this pragmatic stepped-wedge pilot study, we found the ALIGN intervention was feasible in the SNF rehab setting and was deemed acceptable by staff, patients, and caregivers. The enrollment rate of 67% for patients would support a fully powered clinical trial; however, the rate of caregivers who enrolled in the study was much lower. This was, in part, due to the logistical challenges of locating a caregiver on site to consent on the days when study staff were recruiting. The PCSWs conducting the intervention had much higher rates of success in engaging caregivers of enrolled patients (more than 90% of patients had a caregiver actively working with the PCSWs), supporting the assertion that with adequate staffing, enrollment rates of caregivers would be substantially improved. Furthermore, this pilot study results offer some indication of possible effects of the ALIGN intervention on patient- and caregiver centered-outcomes and health care utilization. We found that the effects on this population of patients may be limited to completing advance care planning documentation, while caregiver outcomes suggested potential improvement in perceived communication and caregiver burden/benefit finding. Advocates for advance care planning argue that documentation of advance care planning increases the likelihood of goal concordant care, although the literature is mixed on this point.23–26 Ideally, furthering the scientific methodology of assessing and measuring goal concordant care would help us better understand the potential benefit of interventions like ALIGN and palliative care interventions in general. 27
The ALIGN intervention was developed in the LTACH setting with demonstrated improvement in perceived communication and health care utilization outcomes, including Do Not Attempt Resuscitation Orders, hospice enrollment before death, and rehospitalization rates. This population also had a high six-month mortality rate at 25%. This is in contrast to this cohort of patients admitted to the SNF rehab setting. We selected a LACE score of >7 attempting to capture a higher risk population. We found the mortality rate in all groups was fairly low, which may justify the need for a higher LACE score or other measure of mortality risk in a future trial. Our findings support future research aimed at improving patient-centered utilization patterns (reduce hospitalizations and longer length of hospice stay).
Increasing attention has been directed toward patients in the post-acute care space due to the high rates of hospital readmission and mortality for this population. In addition, this population is at risk for poor palliative care outcomes with evidence of high symptom rates, including pain, shortness of breath, and fatigue, and poor documentation of preferences.28–30 Volandes et al. conducted a trial of a video intervention in the SNF rehab setting to assist with decision making, finding that the majority of patients receiving the video-based intervention opted for comfort-focused care. 31 Many of the other interventions to improve palliative care outcomes have shown promise, yet have mainly been centered in the long-term care nursing facilities rather than the short-stay rehab nursing facilities.11,32–34 The feedback we received from the SNF rehab staff draws attention to the profound challenges in this transitional care setting. Specifically, facility social work staff are overburdened, often needing to focus on disposition, and simply do not have the time to engage in broader goals of care discussions. 9 Without substantial additional investment in palliative care-trained staff or outside consultants integrating into the SNF rehabs, this unique opportunity to explore goals of care is likely to remain unrealized.
One limitation of this study was the fact that a number of patients in the ALIGN phase of the trial did not actually receive the ALIGN intervention. This was due to patient or caregiver refusal of the program a small number of times. Unfortunately, due to the payment model for the intervention, prior authorization from KP was required and at times, this was delayed, leading to missed intervention delivery, due to shorter average length of SNF rehab stay for KP members. While this can be easily overcome in future clinical trials, this may have implications for more widespread implementation of this intervention model, especially as average Medicare length of stay may decrease due to current reform measures. 22 Another limitation was lower than expected follow-up rate for patient participants. We speculate that this is due to two important factors. First, patients' responses to requests for follow-up were low and thought to be secondary to cognitive impairment and illness-related fatigue. Turnover of study staff further challenged follow-up data collection at the study midpoint that was addressed, resulting in 100% follow-up rates for the final quarter of the study. Finally, the population lacked diversity and the broader generalizability for the ALIGN intervention in minority populations is unknown and remains an important gap to address in future research.
Conclusions and Implications
We found the ALIGN intervention to be feasible and acceptable to caregivers and SNF staff alike. Furthermore, the preliminary exploratory outcomes suggest the intervention may have a benefit for caregiver burden/meaning finding, perceived communication, patient advance care planning, and some patient-centered health care utilization. Next steps are to test the intervention in a larger trial of patient and caregiver dyads, considering adjusting the LACE threshold and eligibility criteria to select for a population at higher risk for mortality.
Footnotes
Acknowledgment
The sponsor had no role in the design, methods, subject recruitment, data collections, analysis, and preparation of article.
Funding Information
This work was supported by a grant from the National Palliative Care Research Center.
Author Disclosure Statement
Authors have no identified conflicts of interest. However, in the spirit of full transparency, the four palliative care social workers who are co-authors on this article have developed and conducted the ALIGN intervention that was tested in this feasibility trial. They have formed an independent LLC (The Holding Group) to allow for billing of their services through a consulting relationship with Kaiser Permanente. However, they have no direct or immediate indirect financial gain with the publication of this article or these results.