
Abstract
Background:
More medical residents and fellows outside of palliative care (PC) will need to be trained in primary PC (PPC) to meet an increasing patient need.
Objective:
To systematically review surveys of program leadership in postgraduate medical training programs and their respective PPC curricula.
Methods:
This review included all studies of program leadership surveyed about their PPC curricula in U.S. graduate medical education programs, published in English, and listed on MEDLINE, CINAHL, and EMBASE through January 2020.
Results:
Data were extracted from eight studies that met the selection criteria out of 221 reviewed texts. PC domains of communication, symptom management, and end-of-life care were taught in all medical specialties most commonly through didactics and PC rotations. Program leadership supported expanding PPC curriculum, with lack of time being the most common barrier. There were differences by specialty in which trainees were exposed to PPC education, with most programs not using a formal curriculum.
Conclusions:
Generally, there are positive attitudes about PPC education, but there remain significant numbers of trainees with no exposure, and heterogeneity in the content and delivery of PPC education across specialties. PPC Education in U.S. Residencies and Fellowships: A Systematic Review of Program Leadership Perspectives.
Introduction
Models of care predict that the number of graduating palliative care (PC) fellows would need to double by 2030 to meet the demand for specialty PC clinical services. 1 To meet this need, nonpalliative providers have been increasingly providing PC services for their patients, known as primary PC (PPC).2–5 PPC improves patient access to PC services and strengthens long-term patient/provider relationships. 6 Education in PPC has been shown to develop trainee confidence, knowledge, and clinical skills, 7 and therefore, improving PPC education for trainees should increase access to PPC.
To promote the inclusion of PPC within and across graduate medical education (GME) programs, it is necessary to assess the current practices and opinions of stakeholders involved in curricular development. A prior systematic review has evaluated the perspectives of trainees regarding the PPC education needed. 8 To our knowledge, no prior studies have evaluated the perspectives of program leadership in a systematic manner.
To better understand the landscape of PPC education in U.S. graduate medical residencies and fellowships, we conducted a systematic review of studies that have surveyed program leadership on their PPC educational curricula. Our primary study question was based on program leadership perspectives: what are the PPC educational interventions in U.S. GME programs? Our secondary question was based on program leadership perspectives: how do these programs differ from each other regarding education content, delivery, and attitudes of PPC education?
Methods
Data sources and searches
Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines were followed in the planning and execution of this study. 9 The study was exempt by the institutional review board. This search was conducted by a professional medical research librarian using MEDLINE, CINAHL, and EMBASE databases from inception through January 17, 2020. Key MeSH terms were as follows: palliative, hospice, end-of-life care, comfort care, terminal care, death, internship, residency, residents, fellows, fellowship, education, knowledge, clinical competence, program evaluation, survey, and opinion.
Study selection
Two authors (K.P., A.K.M.) split search results to screen for duplicate entries and studies not written in English, which were removed. Titles of abstracts were screened for studies not conducted in the United States, after which abstracts were screened for full-text review if they met inclusion criteria. If either author was unsure about inclusion based on abstract review, a full-text review was performed. Consensus was reached by discussion between both authors if discrepancies arose at any stage of review.
Studies included in this review were published in peer-reviewed journals and written in English. Studies needed to evaluate postgraduate medical training programs in the United States and could be in any medical specialty except hospice and palliative medicine (HPM). Studies needed to include evaluation responses by program directors (PDs) or assistant/associate program directors (aPDs/APDs). Studies had to describe the curriculum's education content, delivery methods, and evaluation instruments to be included in this review.
Studies were excluded if they were not in English, of postgraduate medical training programs outside the United States, review articles, or meta-analyses. Studies that did not specify between interdisciplinary trainees, respondent type, medical specialties, or graduate level of medical trainees were excluded. Studies that did not specifically report evaluations of curricula by PDs/APDs/aPDs were also excluded. If studies included respondents other than program leadership, those data were not included in this review.
Data extraction
All studies included in this review for data extraction were split between all authors, and then checked again by author M.S. Studies were assessed for level of training (residency or fellowship), medical specialty, and leadership role of respondents (PD, aPD, or APD).
During our data extraction, we categorized the survey data from each study into content domains and delivery methods. While doing this we referenced categories that had been previously created by Thomas and colleagues and the Accreditation Council for Graduate Medical Education (ACGME).10,11 Content domains included communication (including goals of care or advance care planning), symptom management, end-of-life care (EOLC), psychosocial support, spiritual support, transitions of care/resources (TOC/RE), ethics, and bereavement. Educational delivery method categories included the presence of any PC education, didactics/lectures, small groups, elective or required PC rotations, standardized patients or simulations, self-learning materials, journal clubs, and the presence of a formal curriculum. Simulations and standardized patients were combined into one category as they target similar learning objectives: psychomotor skills/competence, psychomotor behavioral/performance, and affective attitudes. 10 What constituted a formal curriculum was not specified in any study, but ideally included clearly outlined learning goals, objectives, and an explicit approach to evaluation. 10 When a study documented how many programs in that specialty utilized a specific content domain or delivery method, this was recorded.
Attitudes about PPC education were also extracted, including opinions on the importance of PPC and satisfaction with PPC education. Evaluation instruments were categorized based on the framework established by Thomas et al. 10 This included subjective knowledge, objective knowledge, self-assessments (described as attitudes, perceptions, confidence, satisfaction, or comfort), or direct observations.
Quality assessment
The Mixed Methods Appraisal Tool (MMAT), version 2018, was used to assess the quality of studies included in this review. This quality assessment tool is intended to be used for reviews that include studies with mixed methods (qualitative, quantitative, and mixed methods). 12 It was chosen because it has a section specifically for quantitative descriptive studies that fit well with studies we reviewed. Two authors (M.S., A.K.M.) independently assessed the quality of each study using the MMAT, and jointly agreed on any discrepancies.
Results
Our search identified a total of 3642 articles, of which 2936 studies remained for screening after removing duplicates and non-English studies (Fig. 1). Two hundred twenty-one full-text studies were assessed, of which 9 studies met all the inclusion criteria.13–21
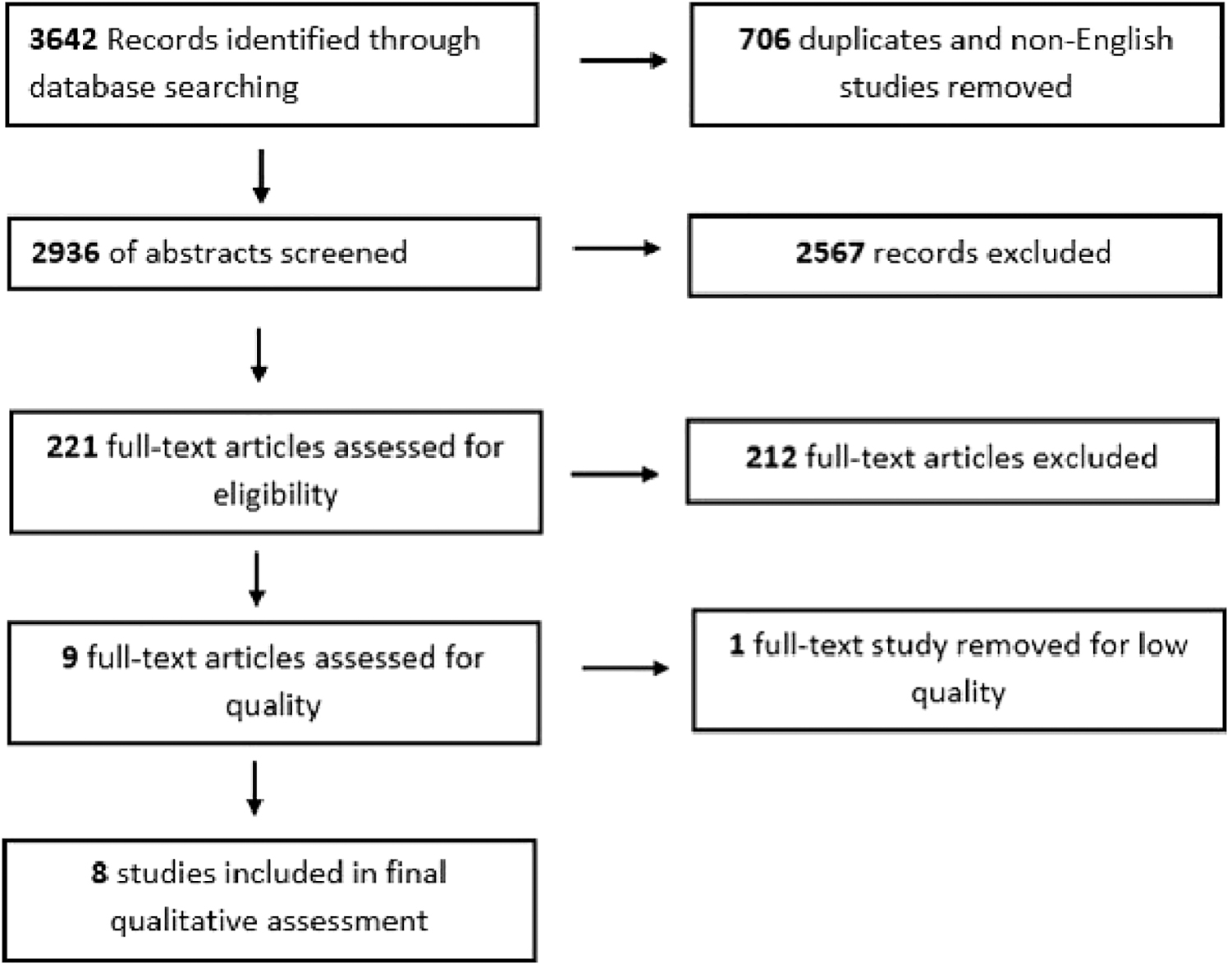
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analysis.
We assessed study quality using the MMAT. One study did not specifically define a research question and was therefore excluded. 21 Seven studies had a risk of nonresponse bias due to low response rate, defined for this review as <70%. A threshold of 70% was chosen as this has been found to minimize nonresponse bias in survey studies.22,23 One study had an increased risk of not being representative of the intended population because it did not report the characteristics of responding programs. Despite these risks of bias, all eight studies were found to be of high enough quality to be included for qualitative analysis based on their total MMAT by two independent reviewers (Table 1).
Mixed Methods Appraisal Tool Quality Assessment
EM, emergency medicine; GYN-ONC, gynecology oncology; HBP/SO, hepato-pancreato-biliary/surgical oncology; IM, internal medicine; NEURO, neurology; NEURO-ONC, neuro-oncology; PCCM, pulmonary and critical care medicine; PED-ONC, pediatric oncology; PEDS, pediatrics; RR, response rate.
All studies surveyed program leadership within different postgraduate U.S. residencies and fellowships. Studies of residency medical specialties included were internal medicine (n = 1), 17 pediatrics (n = 1), 19 neurology (n = 1), 13 and emergency medicine (n = 1). 15 Studies of fellowship medical specialties included were neuro-oncology (n = 1), 14 gynecology oncology (n = 1) 16 , hepatobiliary and pancreatic surgery and surgical oncology (HPB/SO) (n = 1), 18 and pulmonary and critical care medicine (n = 1). 20
Five of the studies exclusively had PD respondents16–20 and three studies included APDs or aPDs.13–15 Survey response rate ranged from 24.8% to 70% (Table 2).13–20
Summary of Program Directors' Surveys
aPD, assistant program director; APD, associate program director; CARD, cardiology; CCM, critical care medicine; GP, general practice; HBP, hepato-pancreato-biliary; NICU: neonatal intensive care; NR, not recorded; ONC, oncology; PD, program director; SO, surgical oncology.
Attitudes toward PPC education
All evaluations of curricula were in the form of self-assessments by program leadership. Surveys asked program leadership's perspectives on the importance of incorporating PPC in their GME curricula. In programs surveyed, most program leaders (64–87.7%) reported that PPC education was important to teach their trainees.15,17 PDs of neurology residency programs identified 8 of 10 PC domains as “very important” or “important.” 13 PDs of neuro-oncology fellowship programs identified all 10 PC domains as “very important” or “important.” 14
In addition, surveys asked program leadership which PPC domains and delivery methods were most important to include in their curricula. PDs of gynecology oncology fellowship programs ranked opioid rotation, management of depression, management of fatigue, delivering bad news, and discussing prognosis as the five most important topics of PC education for their trainees. 16 PDs of emergency medicine programs ranked all PC domains except advance care planning as being at least “somewhat important” with difficult communication, management of pain, and EOLC ranked highest. 15 Emergency medicine residency PDs thought that bedside teaching, mentoring from HPM faculty, and case-based simulation were their most effective current teaching methods. 15
Satisfaction with their existing PPC curriculum was included in surveys of program leadership. Many PDs supported expanding their PPC curriculum and felt that their current educational methods could be improved. Sixty percent of SO/HPB PDs wanted to improve their current PC education 16 and more than half (50–80%) of pulmonary/critical care PDs 20 thought their education in communication skills, symptom control, community/institutional resources, and withdrawing ventilation was inadequate. All surveyed gynecology oncology fellowship PDs would use additional educational materials if they were available 16 and most pediatric residency PDs believed a formalized curriculum (80%) and a PC rotation (84%) would enhance trainee education. 19 Only 58% of neurology residency PDs were at least “somewhat satisfied” with their program's current PC education compared with 83% of neuro-oncology fellowship PDs.13,14
Content
PDs from all medical specialties reported communication, symptom management, and EOLC within their PPC curricula. Ethics and TOC/RE care were also reported by PDs in most specialties (n = 5). Spiritual support was reported by some PDs in half of the specialties, with a minority of specialties including bereavement and psychosocial support (n = 2). Only three studies (gynecology oncology, internal medicine, and HBP/SO) specified the percentage of PDs within their specialty that included these educational domains (Table 3).16–18
Education Content
B, bereavement; CC, care coordination; Comm, communication; EOLC, end of life care; NR, not reported; PS, psychosocial support; SM, symptom management; SS, spiritual support; X, reported in some programs, but rate not reported.
Delivery
The number of programs offering some form of PPC education varied based on the specialty. In every specialty, some surveyed PDs reported curricula including didactics and PPC rotations. When specified, PPC rotations were typically elective with required rotations offered between 3% and 28% of the time.13,14,16,19 Other methods of education delivery were reported by PDs in some specialties, including self-learning (n = 5), standardized patients/simulation (n = 5), small groups (n = 3), and journal clubs (n = 2).
PDs from gynecology oncology, pulmonary critical care, and pediatrics reported on having a formal curriculum; this was found in a minority of programs, ranging from 14% to 45% (Table 4).16,19,20
Education Delivery
CARD, cardiology; CCM, critical care medicine; GP, general practice; HBP, hepato-pancreato-biliary; NICU, neonatal intensive care; NR, not reported; ONC, oncology; SO, surgical oncology; X, present, but data on frequency not obtained.
Barriers
Studies of two residency programs13,15 and three fellowship programs14,18,20 asked PDs to identify existing barriers to including PC in their curricula. Three of five studies reported time limitations as the main barrier.13,14,20 Additional barriers included faculty availability (n = 2),13,14 faculty expertise (n = 2),13,15 lack of faculty or fellow interest (n = 1), 15 fellow discomfort with death and dying, and difficulty with curricular changes (n = 1). 18
Discussion
This systematic review examined the existing PPC educational priorities and opportunities for graduate medical trainees in the United States according to the GME program leadership. While prior systematic reviews of PPC have focused on trainees' educational needs and curricular impact, none has evaluated curricula from the program leadership's perspective. 8 In our review, we found that PPC is widely incorporated in residency and fellowship programs, and while current leadership believe PPC education is important, they are not satisfied with their current curricula. Overall, we found PPC education to be heterogeneous in content and delivery. In the studies we reviewed, program leadership did not directly evaluate the impact of their curricula.
PDs across specialties responded that they believe in the importance of PC education for their trainees but reported dissatisfaction with their current curricula. Many PDs also expressed a desire to expand their current curricula. This belief in the importance of and a desire to expand PPC education highlights the motivation to incorporate more PPC into existing and new curricula. This reflects the outcomes of prior studies demonstrating specialists requesting more PPC education and the inclusion of PC exposure into ACGME guidelines in multiple specialties.16,18–20,24
Lack of specific national PPC education guidelines may account for this dissatisfaction. In our findings, the PPC curricula varied by content and delivery. The PC domains included most commonly were symptom management, EOLC, and communication. Prior studies reflect the need for knowledge and skills in these areas by practicing clinicians.25,26 O'Connor et al. found these to be the most common reasons for specialty PC consultations. 27 While variation in clinical PC needs exists across medical specialties, our findings suggest common educational needs as identified by program leadership. The development of future curricula should consider the inclusion of these specific PC domains. On a national level, this information allows for specialties to identify gaps in education that might need more attention. For example, we found that bereavement, spiritual support, and psychosocial support were not commonly taught and would be useful areas of curricular growth. Bereavement training can help improve satisfaction of care for families and prevent physician burnout after patients die, and spiritual care training improves trainee communication surrounding spirituality.28,29
Most program leadership included in this review reported that they were not using a formal curriculum for their PC.16,19,20 In an ideal setting, the teaching content in a formal curriculum stems from clear learning goals and objectives. 10 When available, specialty specific competencies can serve as a framework for developing these learning goals and objectives. Because training needs are different depending on the specialty, having specialty specific competencies is important for generating pertinent curricula. Currently, emergency medicine, internal medicine, and family medicine are the only specialties with published PPC educational competencies for their trainees.30,31 Without having more specialty specific competencies, trainees may continue to have gaps in their PPC education and formal curricula would likely vary between programs. Identifying barriers to improving PC education within specialties is another critical step before expanding PPC curricula. Of the programs surveyed, most identified lack of time or faculty availability as the main barriers to including more PC education. Environmental barriers including inadequate time are commonly referenced barriers in medical education. 32 This may be especially challenging in PC education where role-playing and teaching communication can be especially time intensive. Program leadership will need to continue to demonstrate beneficial outcomes of their curricula to motivate other programs to create space within their teaching time for more PC education.
This review has several limitations. Most of the studies used different surveys, meaning that differences in results between programs may not be fully representative of differences between curricula. For example, many studies did not include questions about spiritual or psychosocial domains, meaning that a higher, or lower, proportion of programs may have included this in their education than is reported. This heterogeneity limited our ability to perform a complete data analysis across studies. Furthermore, there was a low response rate for many of the surveys, leaving room for nonresponse bias. Finally, none of the studies was able to assess outcomes of their curricula, which is needed to better understand the effects of implementing PC curricula in different specialties. This will help programs determine whether the most common PPC delivery methods are effective (didactics/lecture, rotation), or if we need to focus more on less commonly used delivery methods including simulations and standardized patients.
Conclusion
Program leadership across GME specialties report PPC to be an important part of their curricula; however, variations in content and delivery exist. This variability may lead to a lack of satisfaction with existing educational interventions. Future studies of program leaders should assess the impact of different curricula on clinical outcomes to better understand which delivery methods are most effective. In addition, developing more specialty-specific PPC guidelines would help with the development of more consistent and higher quality curricula.
Footnotes
Funding Information
No funding was received for this review.
Author Disclosure Statement
No competing financial interests exist.