
Abstract
Background:
Concurrent care enables seriously ill pediatric Medicaid and Children's Health Insurance Program (CHIP) beneficiaries to continue curative treatments along with the supportive services usually associated with hospice care. Although a few studies have examined pediatric concurrent care, none has explored the economics of this care delivery approach for medically complex children.
Objective:
The purpose of this study was to identify the cost components relevant for an economic analysis of pediatric concurrent hospice care and demonstrate the use of the cost components in an economic case illustration.
Methods:
A scoping review of the hospice cost literature was conducted to identify article focused on hospice costs that were published in the journal literature from 2000 to 2019. A preliminary economic analysis was also conducted using a cost-minimization approach with data from a large mid-Atlantic pediatric hospice provider. We compared costs between concurrent versus standard hospice care for children.
Results:
Fifteen hospice cost articles were identified and no article on concurrent care costs. Most articles in the scoping review focused on hospice personnel costs, followed by supplies/equipment, and other. Personnel and costs were higher for standard hospice children compared with concurrent care, whereas concurrent care children had higher supplies/equipment costs.
Conclusions:
Identifying cost components are critical to economic analysis of pediatric concurrent care. These findings provide preliminary evidence about the difference in costs between concurrent and standard hospice care for children.
Background
Concurrent Care for Children was enacted in 2010 with the passage of the Patient Protection and Affordable Care Act (ACA, Section 2302). Concurrent care enables seriously ill pediatric Medicaid and Children's Health Insurance Program (CHIP) beneficiaries to continue curative treatments along with the supportive services usually associated with hospice care. 1 Concurrent care was a response to a growing consensus in the end-of-life community that hospice eligibility requirements were critical barriers to end-of-life care, especially for seriously ill children. 2 Before concurrent care, hospice eligibility for children followed adult hospice standards and required that children have a life expectancy of approximately six months or less as certified by a hospice medical director and an attending physician or nurse practitioner. Hospice certification required that children discontinue all life-prolonging or curative care (i.e., chemotherapy, dialysis, bone marrow transplant, antiretroviral regimens, radiation, transfusions, and transplant rejection medication) upon hospice enrollment. These two eligibility rules, in particular forgoing curative attempts, forced many families to make very difficult choices between attempts to treat a child's disease or managing comfort and quality of life during treatment of advanced disease. Concurrent care allows many families to continue curative treatments and therapies, whereas their child enrolls in hospice care with a six months to live prognosis.
Upon the passage of the ACA, hospices received minimal guidance from the Centers for Medicare and Medicaid Services (CMS) on the implementation of concurrent care. 3 CMS and many state Medicaid offices issued no regulations or guidelines, nor were hospice per diems modified to account for the significant changes in services provided. 4 Although a few studies have examined pediatric concurrent care, 5 none have explored the economics of this care delivery approach for medically complex children. Consequently, it remains unclear what the hospice cost components for concurrent care are and how they might be applied in an economic analysis. From a hospice perspective, costs are the expenses a hospice incurs in the provision of care to a patient. 6 Costs are often categorized as direct or indirect costs. Direct costs are connected to a specific patient and include fixed and variable hospice costs (e.g., labor, materials), whereas indirect costs encompass costs that are necessary for providing care but may not be directly related to a specific individual patient (e.g., triage, care coordination, business overhead, administration).
Understanding the cost components of pediatric concurrent hospice care is important and policy relevant. Improving our knowledge of cost components is a critical first step in gathering baseline information about costs of concurrent care. This information will assist in developing a financial framework of pediatric concurrent hospice care that includes costs and revenues, and ultimately a comprehensive economic model that incorporates both treatment and hospice services. Information on cost components is also timely given the current policy environment. For example, some state Medicaid plans began requiring all hospices that provide pediatric concurrent care to perform daily visits with pediatric patients and to be the care coordinators for all services without any change in payment. 7 Understanding cost components will enable pediatric end-of-life researchers to evaluate the economic impact of concurrent care, including state-level adaptations.
This article has two main purposes. First, we identified the cost components relevant for an economic analysis of pediatric concurrent hospice care. Using pediatric and adult hospice economic literature and reports, the range of financial costs related to pediatric concurrent hospice care were identified. Second, we demonstrated the use of the cost components in an economic case illustration. We used a cost-minimization analysis (CMA) that compared the cost strategy of pediatric concurrent hospice care versus pediatric standard hospice care.
Methods
This study used a multiple methods design, which included a literature review of hospice cost components and a real-world, hospice case illustration that demonstrated the application of the cost components.
Scoping review
We conducted a scoping review of the hospice cost literature to identify articles focused on hospice costs that were published in the journal literature from 2000 to 2019.8,9 During this period, pediatric palliative and hospice care defined itself as distinct from adult hospice, programs proliferated rapidly, the stage was set for the passage of concurrent care policy in 2010 as part of the ACA, and pediatric hospice and palliative care became a recognized medical subspecialty. 2 To be included in the review, articles were needed to focus on adult and pediatric hospice costs with information on cost components. Peer-reviewed journal articles were included if they were hospice studies, conducted in the United States, and were written in English. Articles were excluded if they focused broadly on end-of-life or palliative care-only costs because of the different cost structures potentially present in these care delivery models. Case reports, nonresearch quality improvement reports, opinions, and guidelines were excluded. Duplicate citations were also excluded.
The literature search was conducted in August 2019, in the following databases: Medline, CINAHL, and Web of Science. These databases were searched to retrieve articles about hospice costs using the terms hospice+ concurrent care+ costs+ expenses+ economic+ financial in the title, abstract, or keywords. We also conducted a hand search of reference lists to identify any articles not captured through the database search. We used a modified cost framework from Lindley et al. and clinical hospice experience with pediatric concurrent care to extract hospice cost components for pediatric concurrent care. 10 The major cost categories used in this review were relevant to pediatric care and included hospice personnel, supplies and equipment, and other costs. For each study reviewed, information on the cost component, definition, and measurement of the cost components was captured and extracted.
Case illustration
We conducted a preliminary economic analysis using CMA. CMA comprises the least costly alternatives between two care health options. It is used widely in health care economics to compare costs of care delivery types, drugs, and therapeutic modalities. Cost minimization compares the costs of end-of-life delivery A versus end-of-life delivery B, and evaluates which cost strategy offers reduced costs. 11 This method of cost evaluation is used when outcomes are assumed to be roughly equivalent. Among the various cost analysis methods (e.g., cost consequences, cost effectiveness, cost utility, and cost benefit) CMA is appropriate for initial and preliminary cost analysis.
In our illustration, we compared the cost strategy of pediatric concurrent care to pediatric standard hospice care strategy. We analyzed the 2018 de-identified financial data from a large community-based hospice organization in the mid-Atlantic region with a trained pediatric staff that provided concurrent and standard hospice care throughout a large geographic region. We generated descriptive statistics (i.e., means and standard deviations) for the cost components. Cost measures were created using the actual costs incurred by the child divided by the number of days enrolled in hospice care. Cost measures are presented as the average cost per days enrolled. Concurrent care and standard hospice care were mutually exclusive. All costs were in 2019 U.S. dollars. Comparisons of the strategies were conducted using a Mann–Whitney U test of means. Because of the small sample sizes of the comparison groups and the non-normal distribution of our demonstration cost data, p-values were not reported. This study was approved by University of Tennessee, Institutional Review Board.
Results
Cost components
The initial search strategy resulted in a total of 93 adult and pediatric citations from electronic databases and hand searches of the reference lists (Fig. 1). Thirty citations were removed because they were duplicates. Based on screening the titles and abstracts, 25 citations were removed because they did not meet one or more of the screening criteria, leaving 38 for full-text screening. Following the full-text screening process, 23 were removed owing to meeting one or more exclusion criteria. The search of the literature resulted in a final set of 15 articles for the review.
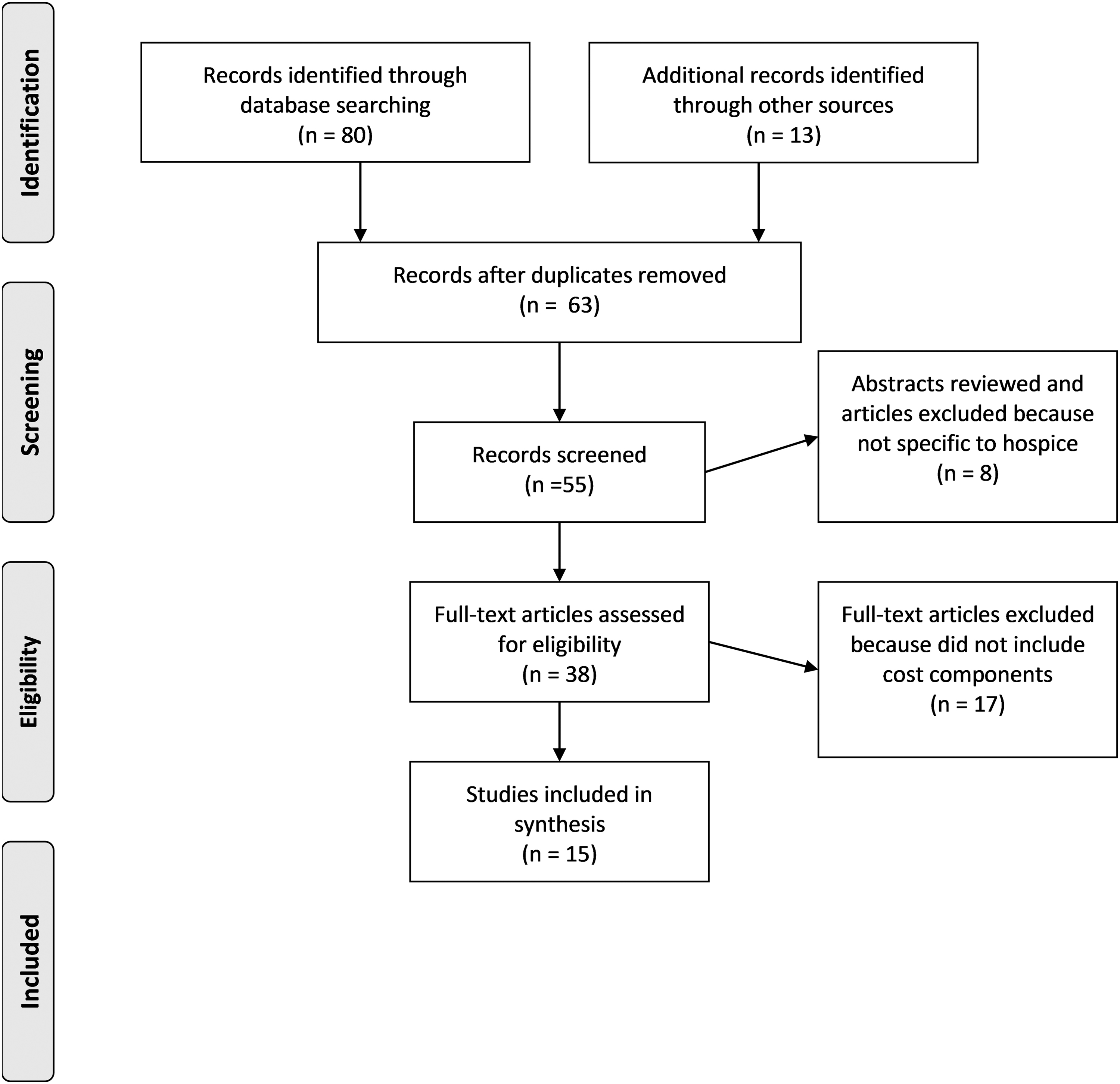
PRISMA flow chart.
Table 1 presents a summary of the cost components classifications and cost information from the literature. The articles ranged in date from 2004 to 2017. There were seven hospice personnel cost articles identified.12–18 The most common type of hospice cost studies included personnel costs for nurses: registered nurses (RNs), licensed practical nurses (LPNs), and advanced practice registered nurses (APRNs),12–16 whereas no studies were identified that included spiritual care costs. No studies were identified that provided information on concurrent care personnel costs.
Cost Components of Pediatric Concurrent Hospice Care
APRN, advanced practice registered nurse; DME, durable medical equipment; LPN, licensed practical nurse; RN, registered nurse.
Nine studies included hospice supply and equipment costs.12,18–25 The most common cost in this category was medications with nine studies providing information.12,18–25 Several studies offered information on the different types of medications included in hospice cost calculations. For example, Speer et al. identified cost of 16 discarded medications commonly used in hospice care, 21 whereas Romo and Gifford identified 19 medications in their cost analysis of a musical intervention for hospice patients. 12 Other researchers included drugs, biological and infusion therapy in the definition of medications. 25 It was not common for these studies to offer detail on the specific supplies and equipment. These costs were generally combined together and presented as overall supplies or equipment costs. 18 No studies were identified that provided information on concurrent care supplies and equipment costs.
Three studies in the review offered information on other hospice cost components.14,16,19 Cost information on triage or the 24/7 phone support for patients and families along with care coordination was nonexistent. Triage may be a cost factor more common among pediatric hospice providers than adults because parents often call the hospice staff regarding concerns about signs and symptoms at end of life for their child, and a triage resource allows them to get timely assistance. In addition, concurrent care for children requires a level of care coordination not typically offered in adult hospice care. Hospice providers are now providing care coordination regarding medical services, medications, and therapies between hospice and the treatment teams. One study, Gardiner et al. discussed inpatient costs for hospice patient in their evaluation of cost components for palliative care for adults. 19 Finally, two researchers identified administrative costs as a critical factor in the cost structure of providing hospice care.12,16
Case illustration
Our case illustration utilized an economic analysis approach (i.e., cost minimization) that compared the cost strategies of pediatric concurrent and standard hospice care. For this case illustration, we used financial data from a large pediatric hospice provider. De-identified data were from 44 children younger than 19 years enrolled in hospice care in 2018. The average age of the children was six years. Approximately one-third of children had Medicaid insurance and a cancer diagnosis. The average length of stay in hospice was 125 days (median = 82 days). More than 70% of the children received concurrent care from either Medicaid or private insurance.
The comparison of pediatric concurrent versus standard hospice personnel cost components is given in Table 2. Comparing concurrent and standard hospice care labor costs, RN visits, LPN visits, social work visits, spiritual care coordinator visits, and certified nursing assistant visits costs were similar between concurrent and standard hospice care. However, hospice medical director costs were higher for standard hospice care compared with concurrent care ($18.26/day vs. $26.61/day). Total personnel costs were highest for standard hospice care at $79.13/day versus $67.46/day for concurrent care.
Comparison of Personnel Costs between Pediatric Concurrent Hospice versus Standard Hospice Care
SD, standard deviation.
The comparison of hospice supplies and equipment costs between the pediatric concurrent versus standard hospice care are given in Table 3. In the comparison, general supplies were twice as high for concurrent care ($4.66/day vs. 2.36/day), whereas medications were similar between the groups. The cost of durable medical equipment was almost five times higher for concurrent care versus standard hospice. Total supplies and equipment costs were highest for concurrent hospice care ($50.00/day vs. $22.09/day).
Comparison of Hospice Supplies and Equipment Costs between Pediatric Concurrent Hospice versus Standard Hospice Care
Table 4 provides the comparison of other hospice costs. Although triage costs were similar between pediatric concurrent and standard hospice care, care coordination ($7.80/day vs. $12.86/day) and inpatient care ($0.14/day vs. $76.48/day) costs were significantly higher for standard hospice care. Administrative costs were almost double for standard hospice care compared with concurrent care ($37.44/day vs. $63.06/day.). In comparison, the other hospice costs were almost four times higher for standard hospice care versus concurrent hospice care.
Comparison of Other Hospice Costs between Pediatric Concurrent Hospice versus Standard Hospice Care
Discussion
We provided a scoping review of the published literature on hospice cost components important to pediatric concurrent care. Using a concurrent care costing framework, we found that the existing hospice literature primarily focused on personnel and supplies/equipment costs. We believe the current work represents the most comprehensive report using real-world case material to examine the relative cost of concurrent care versus standard hospice care for children.
In general, pediatric care can be labor intensive and costly. The additional costs include the need for specialized training of personnel to care for children, specialized equipment needed for children, more costly therapies chosen for children with advancing disease, that is, total parenteral nutrition, blood transfusions, and intravenous analgesics, which cannot be amortized over a large number of patient days seen in adult hospice medicine. 15 Because the number of pediatric patients cared for by a typical adult hospice organization is small, the relative costs per patient day under care to the organization are expected to be higher. The anticipated higher cost of pediatric care leads some hospice to eschew pediatric care out of the fear that short falls in reimbursement would need to be offset by increased philanthropy and grants. These funds, however, are unpredictable and often difficult to generate. Thus, the findings in this study are important evidence to encourage adult hospices to offer care of children in their communities referred for services under concurrent care guidelines.
Contrary to what might have been expected, the overall personnel costs were less expensive for children receiving concurrent care than standard hospice care. This stands to reason because children under concurrent care may not be in as late a stage of their disease as children receiving standard hospice care and therefore require less intensive hands-on care. 26 Late-stage disease can be expected to demand greater involvement of personnel to assist in the management of increased symptom burden, counseling, and family support, including 24-hour crisis care when needed. On the contrary, supply and equipment costs were found to be five times higher in the children receiving concurrent care, which reflects the fact that families' have frequently chosen disease-directed therapies and life-prolonging interventions, such as advanced respiratory support devices. Because these therapies are disease directed, the cost should be borne under concurrent care by the primary insurer or Medicaid and does not need to fall under the relatively limited per diem offered by the typical hospice benefit. 27
The cost of inpatient care was interesting, because one would anticipate fewer or shorter hospitalizations in an advanced stage of illness, when death becomes more certain. Yet, this figure may represent a greater reliance on inpatient units to deal with challenging symptom management or end-of-life care, when death at home was not an option or families prefer an inpatient location of death. This item deserves further examination and the details were not contained in the available dataset used in this analysis. The other noteworthy item was the increase in administrative costs associated with concurrent care. It is possible that those costs represent care coordination by nonclinical personnel, but the details are similarly not available in the current dataset, although Table 4 contains a generic care coordination cost. In the future, a prospective trial will serve to provide greater detail regarding administrative costs and the circumstances leading to increased inpatient care. Care coordination remains a critical service provided to children receiving concurrent care, which is inadequately covered by health insurance.
As one of the first studies to use an economic model to examine the costs of pediatric concurrent care, our cost model has administrative and research implications. From an administrative perspective, we discovered that cost information is not easily assessable. Although hospices report financials and various cost information on a regular basis, there are systems challenges to collecting cost data. In many cases, electronic medical records with the information on patient demographics, health, and clinical characteristics do not link readily to the administrative record system. Organizations may need to manually link records that can be cost-prohibitive and time-consuming for smaller hospices. From a research perspective, our cost modeling also suggests that clinical, finance, and health economist research team members are needed to collaborate on identifying costs and interpreting the results. For example, our triage category required a deeper discussion among team members to elicit the components and use of triage. Thus, using the model presented in this article was facilitated by interoperating record systems and a multidisciplinary team.
Our cost findings also have policy implications. One of the critical questions raised by our investigation is the allocation of costs for disease-directed therapy. Hospice eligibility requires a hospice physician or nurse practitioner to certify that a patient has a life expectancy of six months or less if the terminal illness runs its normal course. For the pediatric patient, life expectancy is more difficult to predict and, most importantly, few pediatric patients have a disease process that “runs its normal course.” There is little question that the noble goal of curing disease and extending a young life with good function and developmental potential has fundamentally changed the way we care for pediatric patients and the way children die. Under concurrent care, treatment directed at the primary disease process that led to hospice eligibility is reimbursed by the patient's primary insurance provider, whereas the supportive services provided by hospices, for example, social work, expressive therapies, spiritual support, advanced symptom management, is covered under the hospice per diem. The hospice per diem billed for everyday the child is under concurrent care is ∼$190/day for days 1–60 then and decreases to ∼$150/day for days 61+. 27 Disease-directed therapy, for example, surgery, chemotherapy, intensive care unit care, would be cost prohibitive under a hospice per diem reimbursement structure. Thus, concurrent care in the structure we have analyzed suggests sufficient reimbursement for organizations to take on long-term care of medically complex children, who may remain on the hospice census far longer than six months.
Limitations to this study are important to recognize in planning the next steps and future investigations. Our study represented the experience of a large, metropolitan program in Washington, DC and may not be representative of other metropolitan areas around the country. Although the concurrent legislation was federally mandated, each state was entrusted to implement the program through state Medicaid, which has led to widespread variability across the country in the care children can receive. Future investigation must examine the generalizability of our findings. This study was retrospective and relied upon data that were available in the organization's financial database. This led to the inability to reveal the details underlying the individual costs and likely missed other important costs that were buried in the data, for example, the costs for volunteer and bereavement services, which are important components of hospice care. Future studies must include multiple sites and organizations as well as addressing geographic factors that create disparities in concurrent care services availability, that is, children and families living in sparsely populated areas may not have access to experienced pediatric providers.
Conclusions
Our study represents a unique analysis of real-world financial data demonstrating the costs of concurrent care for children versus standard hospice care. The findings suggest that concurrent care is cost-effective in our region, but it is not clear whether that finding would also be obtained in other regions of the country. The increasing prevalence of children with chronic, complex medical conditions receiving concurrent care or its equivalent in all areas of the country demand that we look closely at the cost factors in their care, so that sustainability and good stewardship of resources can be achieved.
Footnotes
Acknowledgments
The authors thank Theresa Profant for reviewing and editing this article. The authors thank Fletcher Vilt for technical assistance in extracting data and Allison Kuchar for administrative support in patient identification.
Authors' Contributions
The authors all contributed to the conceptualization, development, writing, and review of the article.
Funding Information
No funding was received for this article.
Authors Disclosure Statement
No competing financial interests exist.