
Abstract
Background:
Addressing unmet palliative care needs in high-risk surgical patients in low- and middle-income countries must include innovative approaches to limitations in personnel and culturally acceptable assessment modalities.
Objectives:
We assessed the utility of a novel seven-item “Step-1” trigger tool in identifying surgical patients who may benefit from palliative care.
Design:
All adult patients (≥18 years) on general surgery, neurosurgery, and orthopedic surgery wards were enrolled over a four-month period.
Setting/Subjects:
This study took place at Moi Teaching and Referral Hospital (MTRH), one of two Kenyan national referral hospitals.
Measurements:
The “Step-1” trigger tool was administered, capturing provider estimates of prognosis, cancer history, social barriers, admission frequency, hospice history, symptom burden, and functional decline/wasting. A cut-point of ≥3 positive factors was selected, indicating a patient may benefit from palliative care.
Results:
A total of 411 patients were included for analysis. Twenty-five percent (n = 102) of patients had scores ≥3. The cut-point of ≥3 was significantly associated with identifying high-risk patients (HRP; χ2 = 32.3, p < 0.01), defined as those who died or were palliatively discharged, with a sensitivity and specificity of 63.9% and 78.9%, respectively. Survey questions with the highest overall impact included: “Would you be not surprised if the patient died within 12 months?,” “Are there uncontrolled symptoms?,” and “Is there functional decline/wasting?”
Conclusions:
This pilot study demonstrates that the “Step-One” trigger tool is a simple and effective method to identify HRP in resource-limited settings. Although this study identified three highly effective questions, the seven-question assessment is flexible and can be adapted to different settings.
Introduction
Of the estimated 40 million people in the world in need of palliative care, 78% live in low- and middle-income countries (LMICs) where palliative care services are limited.1–5 Few African countries have palliative care integrated into their national health policies, despite multidimensional physical, social, and spiritual issues in patients.4,6 In Kenya, as throughout the world, palliative care has experienced marked expansion, with an 82% increase in available palliative care centers in Kenya from 2005 to 2016. 7 However, this expansion has mainly occurred in oncology, leaving largely unmet needs in other high-risk patient (HRP) populations. 6 One such important population consists of people coping with surgical illness, where the burden of pain, functional limitations, and morbidity are daunting. Postoperative mortality rates in LMIC settings have been reported to be ninefold higher than that in high-income settings, and expansion of surgical care in LMICs is estimated to prevent 1.4 million deaths and 77.2 million disability-adjusted life-years per year globally.8–10
Despite this clear-cut need, palliative care in this population is typically not initiated until operative options are exhausted and death is imminent. In LMIC settings, increased morbidity and mortality is seen in surgical patients despite the fact that patients are younger and frequently present with treatable conditions.11,12 The prognostic uncertainty associated with surgical disease in the context of limited resources, coupled with inadequate numbers of trained palliative care staff, overwhelms the capacity of providers to identify high-risk patients and provide palliative care services.
A screening assessment or “trigger tool” could address this situation but there are little data on such assessments in LMIC. In 2011, a consensus report by the Center to Advance Palliative Care (CAPC) discussed a survey checklist designed for use upon hospital admission to aid general health providers caring for seriously ill patients in identifying unmet palliative care needs. 13 Although the assessment tool was not designed for use in LMIC, we hypothesize its efficiency and ease of use has potential utility in resource-limited settings. This study was performed to evaluate the use of this trigger tool in surgical patients at a large referral hospital in western Kenya.
Materials and Methods
Setting
This study was performed at the Moi Teaching and Referral Hospital (MTRH), one of two national referral hospitals in Kenya. MTRH, located in Eldoret, serves an estimated patient population of 24 million, with a catchment area covering western Kenya, eastern Uganda, and southern South Sudan. As a referral hospital, MTRH receives complex and difficult-to-manage patients from hospitals across this catchment area. The surgical wards, including general surgery, neurosurgery, and orthopedic surgery, admit an average of 300, 100, and 150 admissions per month, respectively. Nursing to patient ratios may reach 18:1 per cube, with one charge nurse managing the overall ward.
The palliative care team at MTRH consists of two clinical officers (mid-level nonphysician clinicians) and one social worker. 14 This team is responsible for addressing the palliative care needs of all patients in the hospital, although most referrals for palliative care originate from oncology and internal medicine. The team has had extensive training from the Kenya Hospice and Palliative Care Association (KHPCA) and palliative care colleagues from North America. Most of the consultations requested of the palliative care team involve communication of “bad news,” pain management, and facilitating conversations with families. The team also coordinates transfers to a privately owned, 26-bed hospice center called Kimbilio Hospice, which has two locations in the Eldoret region.
Ethical considerations
We obtained informed consent for all patients who participated in the Step-2 assessment. In cases where patients were unable to consent themselves, family members consented as surrogate responders. Patients who were enrolled in the Step-1 trigger tool assessment alone were not consented, as this part of the study only involved patient file review and assessments of the patients' palliative care needs from the perspective of hospital nurses. This study was approved by the Indiana University Institutional Review Board (IRB) and the Moi University/MTRH Institutional Research and Ethics Committee in Eldoret, Kenya.
Design
In this two-part pilot study, all adult patients (≥18 years) in three surgical wards—general surgery, neurosurgery, and orthopedic surgery—from January 20, 2019 to May 6, 2019, were enrolled. A total of 465 patients were enrolled. We manually extracted demographic information from patient files of all enrolled patients. Other data collected included diagnosis, medical history, previous palliative care consults, time from admission to surgery, and the procedure performed. These patients were then evaluated by the Step
This novel Step-1 trigger tool was developed by a multidisciplinary group of North American and Kenyan palliative care physicians, surgeons, nurse practitioners, nurse educators, and students. This tool was adapted from a previously reported palliative care assessment checklist reported by the CAPC. 13 We hypothesized that a frugal trigger tool would permit identification of high-risk surgical patients who might benefit from palliative care intervention. We also hypothesized that this trigger tool can be used by nonpalliative care specialists, allowing expansion of the workforce able to provide palliative care support.
The original CAPC instrument on which the Step-1 trigger tool was based was reviewed by palliative care specialists with experience in our study setting and several items were removed as they were deemed to be not applicable in our study setting. These included items related to complex care requirements, long-term care facilities, home oxygen use, or tracking out of hospital events such as cardiac arrest. A question regarding advanced care planning was removed as such planning is largely absent in our setting.
We administered the abbreviated seven-item assessment (Step-1 trigger tool) to a nurse familiar with the patient. Although surgeons were involved in the design, implementation, and guidance of this project, we saw considerable benefit in collaborating with the surgical nursing staff, as they are the critical personnel most closely involved in patient assessment and care. Furthermore, utilizing nursing evaluation fostered a more “real-life” situation than utilizing a study coordinator alone. In settings with more resources, the Step-1 trigger tool could be performed by other personnel, lessening the burden on frontline providers. The trigger tool could also be easily integrated into existing electronic medical records.
Most frequently, the charge nurse(s) of the general, orthopedic, and neurosurgical ward completed the Step-1 trigger tool, totaling eight nurse respondents. In rare instances where the charge nurse was unfamiliar with the patient, the individual nurse providing direct care to the patient was approached instead. The Step-1 trigger tool was organized in a yes/no format, covering issues including prognosis (“the surprise question”), cancer history, social barriers, admission frequency, hospice history, symptom burden, and functional decline/wasting (Table 1).
Step-1 Trigger Tool
For patients with score of ≥3 on Step-1 trigger tool, additional data were collected (Step-2) including functional status assessment using the Eastern Cooperative Oncology Group (ECOG) performance status scale, and an in-depth interview utilizing the Africa Palliative care Outcome Scale (POS) (Table 2). 15 Step-2 interviews were conducted by trained research assistants fluent in Swahili, Kalenjin, or Luo, the most commonly spoken dialects within the catchment area. Interviews were completed either with the patient or with a family surrogate if the patient was incapacitated. Written informed consent in the appropriate language was obtained before Step-2 interviews. The results and analysis of the Step-2 assessment will be reported separately.
Africa Palliative Care Outcome Scale Items
We tracked the status of all participants for up to 30 days after interview. At that time point we recorded the status of the patient as still hospitalized, discharged, transferred to another hospital, discharged to hospice, or with palliative care follow-up, left against medical advice, or died. We characterized patients as being “high-risk (HRP)” if they died or were discharged to hospice or palliative care within the 30-day follow-up period. A flowchart displaying steps of this project is given in Figure 1. Data collection took place from January 20, 2019 to May 6, 2019.
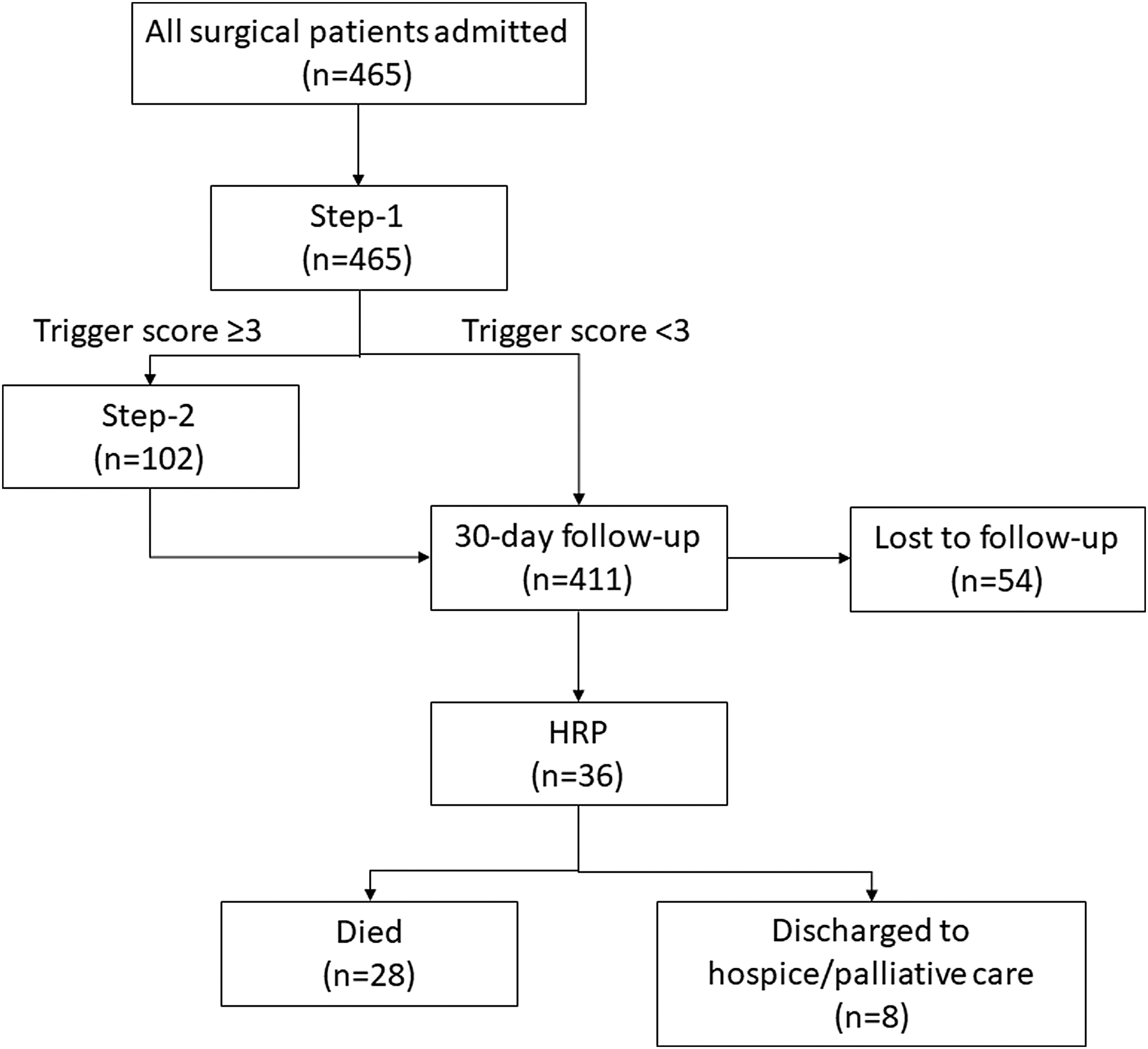
Flowchart of patients through study admission and interventions. The Step-1 Trigger tool was administered for all admitted patients. Those with a trigger tool score of ≥3 were consented for Step-2 interviews with patients or surrogates. Following the Step-2 interviews, patients, along with patients who had scores <3, were followed for 30 days or upon hospital discharge or death. HRP were defined as those who died or were discharged to hospice or palliative care during the follow-up period. Fifty-four patients were lost to follow-up because of lost files. HRP, high-risk patient.
Analysis
A Step-1 trigger tool score was calculated for each patient as the sum of positive responses on the seven-item assessment with equal weighting for all items. The cut-point of ≥3 was selected a priori by palliative care experts in this setting as a “trigger” for defining the need for palliative care services. Patient demographic characteristics were collected (Table 3). A descriptive analysis of enrolled patients included admitting surgical service and 30-day outcomes. We investigated the sensitivity and specificity of the Step-1 trigger tool in identifying HRP by evaluating individual questions, as well as with additional overall score cut-points of ≥4, and ≥5 positive responses. Finally, we performed χ 2 testing using a significance threshold of p ≤ 0.05 to compare each Step-1 trigger tool question with an overall positive Step-1 trigger status.
Patient Demographics
NHIF, National Hospital Insurance Fund.
Results
In total, 465 patients were enrolled in the study, of which 12% (n = 54) were lost to follow-up at 30 days because of lost files and were excluded from analysis. The demographics of the remaining 411 patients are given in Table 1. Of the patients, 50% (n = 205) were on the general surgery service, 22% (n = 92) were on neurosurgery, and 28% (n = 114) were on the orthopedics service. Patients had a median age of 40 years (interquartile range = 29–57) and 69% (n = 282) were men. Cancer and trauma patients made up 22% (n = 89) and 50% (n = 205), respectively, of the study population. Trauma patients were more commonly men and younger, with 38% being ≤30 years of age. In the remaining study cohort, age was more evenly distributed.
The HRP comprised 9% (n = 36) of the total study population, with 28 patients who died, and 8 patients who were discharged to hospice or palliative care. The remaining patients were defined as low risk, with 84% (n = 344) discharged alive, 5% (n = 19) remained in hospital, 2% (n = 8) transferred, and four patients left against medical advice (AMA).
Twenty-five percent of the patients (n = 102) scored ≥3 on the Step-1 trigger tool. Of these 102 participants, 53 had a score of 3, 26 had a score of 4, and 23 patients had a score of 5 or greater. Our initial cut-point of 3 was significantly associated with HRP ( χ 2 = 32.3, p < 0.01) with a sensitivity and specificity of 63.9% and 78.9%, respectively (Table 4). Our elevated cut-points of 4 and 5 were also significantly associated with HRP but resulted in larger shifts in sensitivity and specificity. Table 5 summarizes the positive response rate to each of the seven questions. The individual Step-1 trigger tool questions with the highest positive response rates in patients with an overall positive Step-1 trigger were those related to functional decline/wasting (80%), the “surprise question” (80%), and the pain and symptom question (74%). The only Step-1 trigger question not showing a significant association with a positive Step-1 trigger was the question regarding social barriers (χ 2 = 0.78, p = 0.38).
Step-1 Trigger Tool Cut-Points and High-Risk Patient
HRP, high-risk patient.
Step-1 Trigger Tool Results by Question
Discussion
Our pilot study demonstrates the potential utility and flexibility of a simple screening instrument to identify the need for surgical palliative care services in a resource-limited setting. At our institution, certain Step-1 trigger tool questions proved more applicable than others. Q1, the “surprise” question, and Q7, assessing functional decline/wasting, remained the most frequent positive answers, presenting in >80% of triggered patients. These two questions also showed the strongest sensitivity (63.9% and 77.8%, respectively) in identifying HRP while maintaining high specificity (78.9% and 77.3%, respectively). Difficult to control pain and symptoms (Q6) also showed high sensitivity (69.4%) and specificity (78.4%) for identifying HRP but was not identified in these patients as often as Q1 or Q7. Despite its performance characteristics, we note that “the surprise question” may be difficult to ask and answer owing to strong cultural influences regarding the invocation of death in Kenya.
Although other single questions involving metastatic/advanced cancer or frequent admissions showed high specificity (88.5% and 83.7%, respectively), these queries have limitations. Obviously, the use of the cancer question alone would limit the definition of high risk to oncology patients. The stand-alone utility of the query regarding frequent admissions is limited by the enormous underlying structural vulnerability of the population in Western Kenya. Drivers of frequent admission may include limited community resources for, as well as poor linkage to, post-hospital surgical care. Conversely, admissions may be deferred or not occur owing to distance and financial constraints.
Given that very limited patient financial background data were provided in the charts, the query assessing social barriers was primarily determined by whether a patient was enrolled in the National Hospital Insurance Fund (NHIF), the Kenyan national health insurance program. Enrollment in this fund required a fee of 500 shillings ($5) per month, and membership in NHIF can be viewed as protection against social or familial stresses as it helps to mitigate catastrophic financial costs, which are often associated with surgical care. In addition, the Kenyan medical system frequently requires payment in advance for procedures, supplies, and diagnostic testing. Thus, NHIF plays a significant role in funding care for Kenyans who are enrolled in this benefit, and also promotes timely receipt of appropriate interventions for patients.
In our study, no association with the questions regarding social barriers and patient outcomes was noted (χ 2 = 0.78, p = 0.38), despite our assumption that lower socioeconomic status would be associated with worse outcomes. This counterintuitive result may be explained by the interplay of several contrasting factors. Younger, healthier patients, including those most vulnerable to trauma-related surgical disease, are less inclined to purchase health insurance, creating a favorable bias in the outcomes of the uninsured. Another potential confounder is the setting of our study. A public referral hospital where the large catchment area's most difficult cases are sent regardless of patient socioeconomic background could bias patient outcomes based on the social or financial barriers question. Finally, the query regarding hospice utilization was not positive for any patients in the cohort. Limited availability of hospice beds is certainly a factor in this result, but acceptance of hospice services by our patients and providers, as well as logistical constraints of admitting patients to hospice hours away from their home communities, play equally important roles.
Whereas questions regarding predicted survival, uncontrolled pain, and symptoms and functional decline/wasting proved to be the most effective questions of the Step-1 trigger tool in our setting, we acknowledge the possibility that in different settings, other questions may be equally or more effective. This speaks to the limitations of our study.
Variations in patient data collected, relationships with local hospice centers, or the presence of an established and accessible health system could alter the optimal configuration of this seven-item survey. In addition, an important limitation of the study was the 30-day follow-up. As we did not capture possible instances of patients dying in the hospital after the 30-day follow-up period, or patients being discharged alive but dying at home in a short time frame, we may have actually underestimated the proportion of HRPs. An additional study to include an extended and more comprehensive follow-up period would address this question.
In our analysis of varying cut-points for the Step-1 trigger tool, increases to cut-points of 4 and 5 resulted in increased specificity by increments of ∼10%. However, this was outweighed by the substantial drops in sensitivity of >20% with each cut-point increase. The demographics and disease burden of the surgical population in the study institution underscore our belief that an “ideal” palliative care assessment tool should have high sensitivity to ensure that the greatest proportion of HRPs are identified. However, severe constraints in palliative care staffing and resources in this setting require a prudent instrument targeting resources with specificity. Our analysis suggests that the predetermined cut-point of 3 provided the optimal balance of sensitivity and specificity, thus maximizing the number of patients treated while considering the resource and staffing limitations of our setting.
We underscore the potential importance of our findings given the strong evidence regarding the benefits of early palliative care interventions, including improved retention in care, symptom management, patient and caregiver satisfaction, and quality of life.16–18 Unfortunately, surgical patients around the world have been found to be less likely to receive palliative care services compared with nonsurgical patients, despite often suffering from sudden, catastrophic events and unaddressed morbidity and suffering.19,20 Sadly, a high burden of disease was disproportionately found in younger patients in both trauma and oncology cases. Seventy-six percent of trauma patients and 45% of oncology patients were younger than the age of 50. The relatively poor prognosis of younger patients provides perhaps the strongest argument for increasing palliative care interventions in surgical patients. Through our Step-1 trigger tool, we hope to expand palliative care screening capacity to nonspecialized physicians, nurses, and surgeons, with the hope of improving quality of life for vulnerable surgical patients in LMIC settings.
Conclusion
This pilot study identified a vulnerable high-risk population by using a Step-1 trigger tool, modified from a validated consensus-driven assessment.13 The Step-1 trigger tool proved to be a simple, prudent, and effective method to identify patients who would benefit from palliative care. This assessment can be carried out by any member of the provider team with only the basic information available at the time of admission. Our prespecified cut-point of an overall score ≥3 on the Step-1 trigger tool demonstrated the best balance of sensitivity and specificity.
We have outlined the strengths and weaknesses of individual questions within the Step-1 trigger tool. Further investigation into varying combinations of Step-1 trigger tool questions may prove useful in settings with different resource levels. Although the simplicity and flexibility of the Step-1 trigger tool suggest that it can be a useful assessment in resource-limited settings, we strongly advocate that it be viewed as only a first step in evaluating and addressing urgent palliative care needs in surgical patients. For those surgical patients already facing enormous disparities and nearly insurmountable challenges in accessing adequate health care, continued efforts to expand sustainable and culturally appropriate palliative care services remain critical.
Footnotes
Funding Information
Funding support for this study was provided by The Doris Duke International Clinical Research Fellowship.
Author Disclosure Statement
The authors do not have any conflicts of interest to disclose.