
Abstract
Background:
Informal caregivers may experience a significant burden while caring for cancer patients. Little is known about how caregiver burden varies across different palliative cancer care settings and the factors influencing it.
Objectives:
We compared the severity of caregiver subjective stress burden (emotional impact) among caregivers of patients seen in the outpatient supportive care center (SCC) with those being cared for in the acute palliative care unit (PCU). Secondary aims were to compare other caregiver burden dimensions, quality of life, and any association of caregiver subjective stress burden to various patient and caregiver factors.
Setting and Design:
Eligible patients and their informal caregivers in the SCC or PCU at a comprehensive cancer center in the USA were approached and enrolled. The Montgomery–Borgatta Caregiver Burden Scale and the Short-form 36 were used to measure burden and quality of life. Multivariate general linear regression was employed to evaluate the effect of covariates on subjective stress burden.
Results:
Ninety-eight dyads in the SCC and 74 dyads in the PCU were enrolled. PCU caregivers reported worse subjective stress burden (p = 0.0029) and mental health (p = 0.0299). Multivariate analysis showed correlations between subjective stress burden and caregivers' objective burden (p = 0.0136), subjective demand burden (p ≤ 0.0001), mental health (p = 0.0074), duration of caregiving (p = 0.0680), education (p = 0.0192) and with patients' anxiety (p = 0.0003) and current/recent cancer treatment (p = 0.0579).
Conclusion:
PCU caregivers demonstrated worse emotional burden and mental health than those in the SCC. More research is needed to tailor interventions for various caregiver burden dimensions.
NCI Clinical Trial Registration Number ID: NCI-2019-01197
Introduction
In the United States, recent statistics estimate that 39.8 million people are caregivers of adults, with 7% (2.8 million people) taking care of adult cancer patients.1,2 Cancer caregivers provide support to important aspects of a patient's health care, including assisting with medical issues, activities of daily living, and other financial and care coordination.3,4
Unfortunately, caregivers can be negatively affected in several dimensions while taking care of their loved ones. 5 During the cancer disease trajectory, they not only frequently suffer from physical and emotional symptoms but also from social and financial problems due to restricted time for leisure activities and work, specifically if cancer progresses and the patient's level of dependency increase.6–8 Furthermore, caregiver burden, a concept defined as “distress that caregivers feel as a result of providing care” is a prevalent problem among them.9,10 As a consequence, the quality of life of cancer caregivers is severely compromised during the cancer journey. 11
Although the negative effects of cancer caregiving are well recognized, little is known about the factors that may influence these. Prior studies have suggested that patient- and caregiver-related factors such as patients' symptoms and functional status as well as caregivers' age and socioeconomic status, for example, modulate the negative impacts suffered by the cancer caregiver.12–14 In addition, few studies indicate that caregiver quality of life possibly varies according to the setting where the dyads are receiving care, with caregivers of advanced cancer patients seen in hospice presenting with worse quality of life compared to those being cared for in outpatient treatment settings.15,16 However, these studies provide only an initial insight into the possible contributors influencing caregiver burden.
A better understanding of how the informal cancer caregiver experience may vary according to the setting of care and which specific life domains are being affected by this multidimensional problem would be helpful to identify needs and to develop interventions that are tailored to them, especially among palliative cancer care populations, in which caregiving adverse impacts are severe. 15 Therefore, our primary aim was to compare the severity of caregiver subjective stress burden (emotional impact) among caregivers of patients seen in the outpatient supportive care center (SCC) to those being cared for in the acute palliative care unit (PCU). Between-group differences in other caregiver burden dimensions and quality of life, as well as any association of caregiver subjective stress burden to various patient and caregiver factors were also examined. We hypothesized that the emotional burden would be worse among PCU caregivers.
Materials and Methods
The Institutional Review Board at The MD Anderson Cancer Center, Houston, Texas, approved this study and all patients and caregivers provided informed consent.
Eligible patients and their primary caregivers in their first visit to the SCC and on day one of PCU admission were screened and asked to participate. Patients were included if they had a diagnosis of advanced cancer (defined as locally advanced, recurrent, refractory, or metastatic) and a caregiver identified by the patient or self-identified as their primary informal (nonpaid) caregiver. A primary caregiver was defined as the one person most responsible for providing care to the patient on a daily basis. Both the patient and their caregiver needed to be able to read and speak English. PCU caregivers were also required to be present during the patient's stay. Patients with no caregivers or only a formal (paid) caregiver and those with cognitive impairment, as well as participants (patient or caregiver) who refused to participate were excluded.
In this cancer center, the names supportive and palliative care are used interchangeably and consulting services understand that both are of the same team. An interdisciplinary team experienced in palliative care, including physicians, nurses, clinical pharmacists, clinical psychologists and counselors, social workers, and a chaplain staff both the PCU and SCC in this cancer center. The PCU also has a dedicated case manager who is experienced in transitioning patients to hospice care. Being in a cancer center, only cancer patients are seen. Family conferences are organized in both areas as well as virtual home outreach counseling for patients and caregivers. One of the key differences in the PCU is that patients and caregivers are exposed throughout their stay to the interdisciplinary team compared to time-limited visits in the SCC. They can access this care multiple times throughout the day.
Data collection
The following patient data were collected: patient demographics, including age, gender, ethnicity, religion, marital status, level of education, and employment status; co-morbidities using the Charlson comorbidity index; cancer diagnosis, stage, and current and previous cancer treatments; prognostic score as assessed by the Palliative Prognostic Index (PPI); and symptom distress scores using the Edmonton Symptom Assessment System (ESAS) at the day of first SCC consultation or the day of PCU admission. ESAS scores were collected by proxy if the patient was unable to complete them.
The following caregiver data were collected: demographics, including age, gender, ethnicity, religion, relationship to the patient, marital status, education, employment status, and duration of care since cancer diagnosis; co-morbidities as assessed by the Charlson comorbidity index; caregiver burden (the Montgomery–Borgatta Caregiver Burden Scale), quality of life (the Short-form 36), strength of religious faith and engagement (Santa Clara Strength of Religious Faith, Brief version), and trust in medical profession (Trust in the Medical Profession Questionnaire). Caregivers enrolled at the SCC could answer the surveys by phone after the patient's first consultation (± three days).
Assessment tools
The following assessment tools were used to conduct the study. The primary objective of comparing subjective stress burden between the two caregivers groups and the secondary objectives of examining differences in other caregiver burden dimensions were assessed using the Montgomery–Borgatta Caregiver Burden Scale, a 14-item tool developed to evaluate three main concepts of the caregiver burden by using three subscales: the objective burden, subjective demand, and subjective stress burden subscales.10,17 Objective burden measures the extent of disruptions or changes in various aspects of the caregivers' life and household. Subjective demand burden evaluates the extent to which the caregiver feels the responsibilities are overly demanding, while subjective stress burden quantifies the emotional impact of the caregiving experience on the caregiver, including their attitude and emotional reactions. 18 This instrument has been used to evaluate caregiver burden in both cancer and noncancer populations.18,19
Other secondary objectives were assessed using a variety of instruments. The Short-form 36 Health Survey (SF36) is a validated instrument used to evaluate different aspects of quality of life. It is composed of eight subscales (physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health) and two summary measures (physical and mental health).20–22
The ESAS is a widely used validated instrument that measures 10 common symptoms (pain, fatigue, nausea, depression, anxiety, drowsiness, shortness of breath, appetite, sleep, and feeling of well-being) presented by cancer patients.23,24 We used the ESAS-SF, which is a 12-item version that included 2 nonvalidated items (financial distress and spiritual pain) and has been used in advanced cancer patients. 25
The Santa Clara Strength of Religious Faith Questionnaire is a self-reported tool used to assess strength of religious faith and engagement. In this study, we used the brief five-item version. 26 Trust in the Medical Profession Questionnaire is a five-item instrument used to measure trust in medical profession. It has been proven valid and reliable for this purpose in previous studies. Higher scores (5–25 range) indicate higher trust. 27
The PPI is an objective assessment tool employed to assist clinicians in predicting life expectancy of advanced cancer patients 28 and the Charlson comorbidity index is a widely used tool to measure the severity of comorbid disease in cancer and noncancer populations.29,30
Statistical analysis
To achieve the primary outcome, we planned to enroll a total of 200 evaluable caregivers (100 dyads/center) accounting for an incomplete rate of 10%. This sample provided 80% power to detect an effect size of 0.4 on the severity of subjective stress burden using a two-sample t-test with a two-sided significance level of 0.05.
Data were first summarized using standard descriptive statistics and frequency tabulation. Associations between categorical variables were assessed by cross-tabulation and χ 2 -test. Continuous variables were compared between two groups using the Wilcoxon rank-sum test and multivariate general linear regression was used to evaluate the effect of important covariates on the Subjective Stress Burden. The significant covariates were selected using stepwise selection, using a significance level of 0.10 as the criteria to keep the covariates in the model. All computations were carried out in SAS 9.4 (SAS Institute, Inc., Cary, NC).
Results
Ninety-eight patient and caregiver dyads were enrolled at the SCC and 74 patient and caregiver dyads were enrolled at the PCU. Consort diagrams for SCC and PCU are shown in Figures 1 and 2. The initial goal of 200 total dyads was not reached due to the onset of the COVID-19 pandemic and subsequent restructuring of research and clinical staff and patient appointments. Patients' median age was 62 years and 49% were female. Caregivers' median age was 56 years. Sixty-nine percent were female and 65% were spouses. SCC and PCU patients' and caregivers' characteristics are summarized in Tables 1 and 2, respectively.
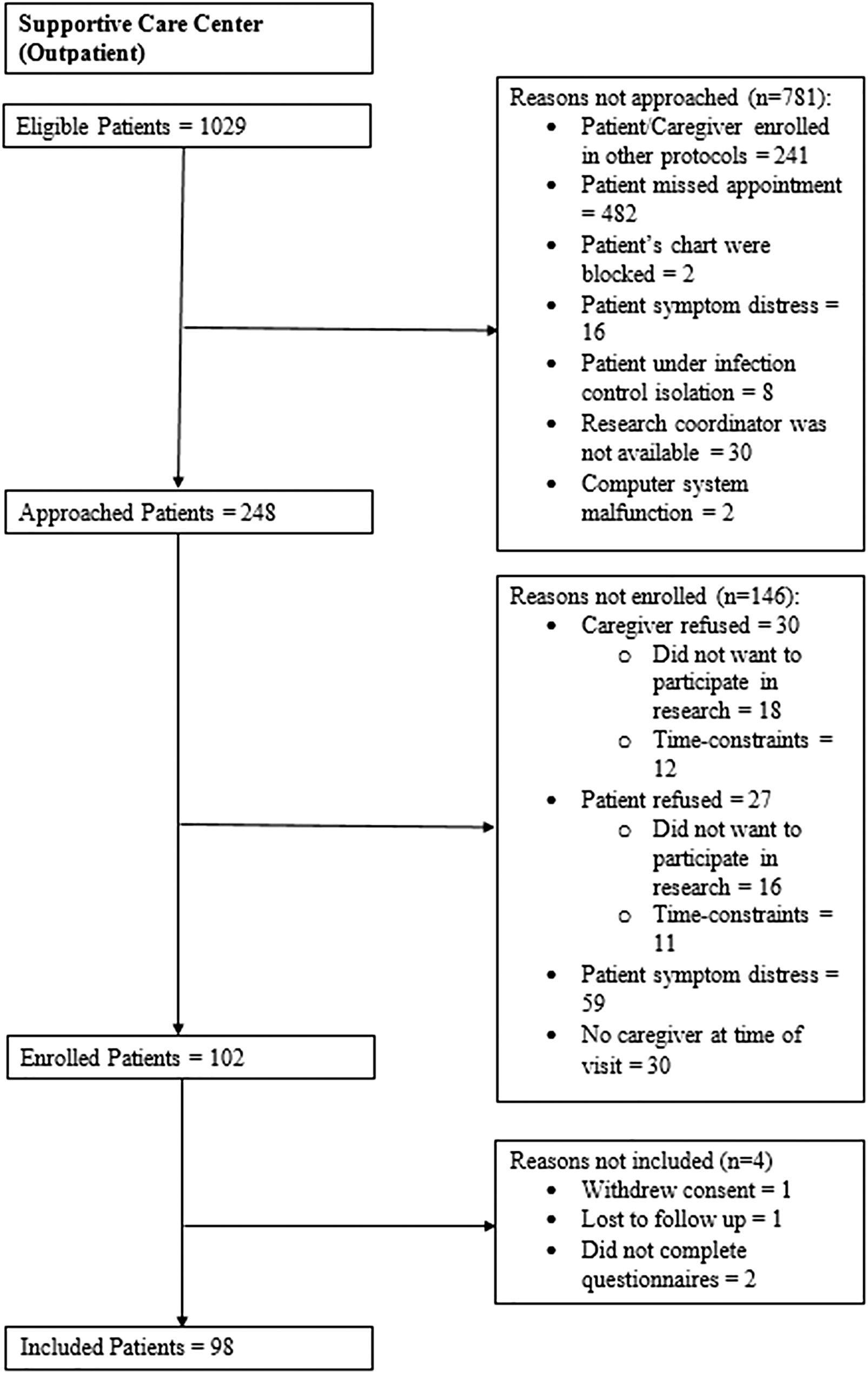
Consort diagram supportive care center.
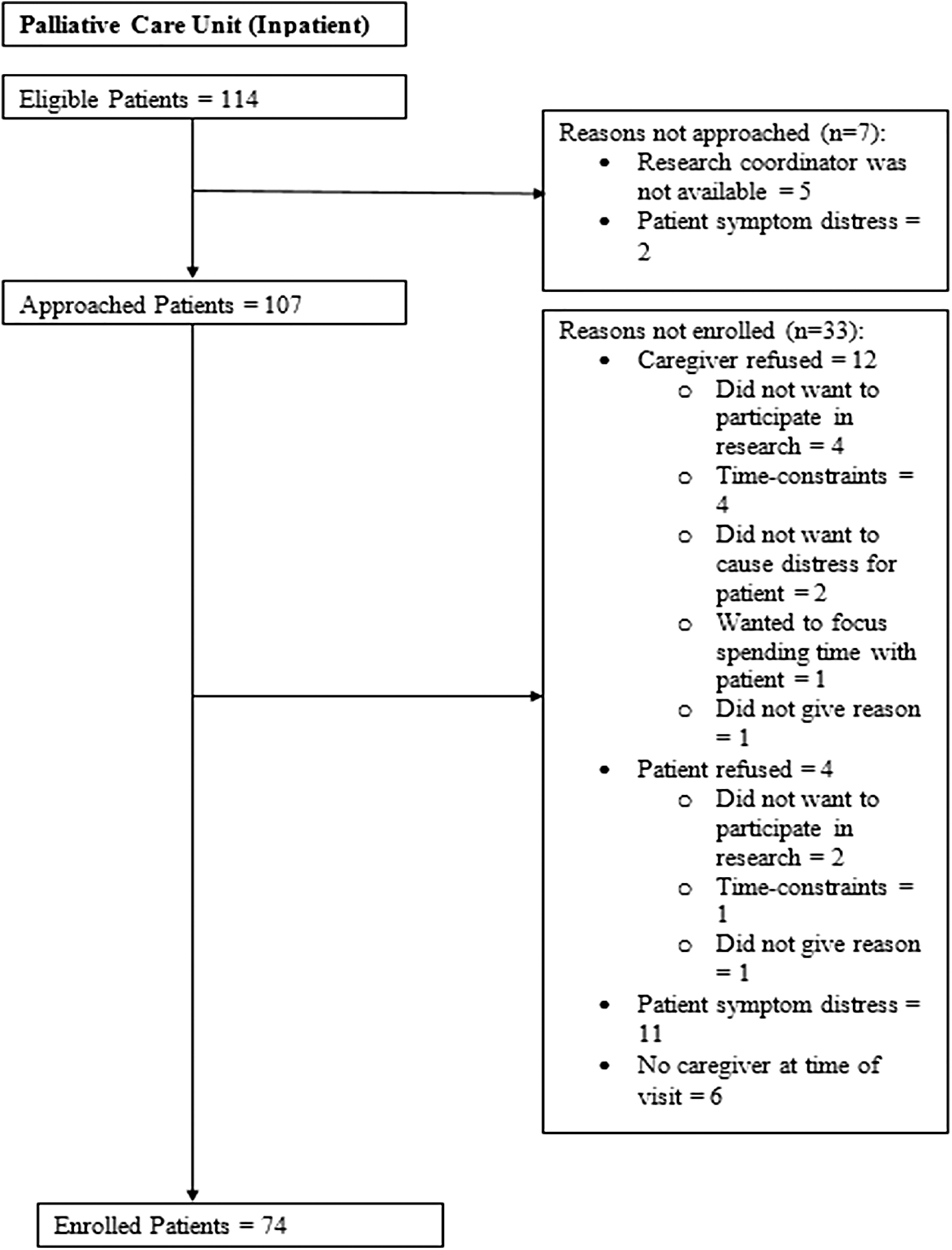
Consort diagram palliative care unit.
Patients' Characteristics
ESAS, Edmonton Symptom Assessment System; IQR, interquartile range; PCU, palliative care unit; PPI, palliative prognostic index; SCC, supportive care center.
Caregivers' Characteristics
Clinically, patients in the PCU reported worse fatigue (p = 0.006), depression (p = 0.0001), anxiety (p = 0.0003), drowsiness (p = 0.03), loss of appetite (p = 0.009), general well-being (p = 0.007), lack of sleep (p < 0.0001), and spiritual pain (p = 0.003) Also, as expected, they had a poorer prognostic index (p < 0.0001). On the other hand, patients in the SCC reported worse concurrent comorbidities (p < 0.0001). We also found significant differences in patients' employment status (p = 0.03), religion (p = 0.001), primary cancer diagnosis (p = 0.001), and the use of current/recent cancer treatments between the two settings (Table 1).
Table 3 summarizes various caregiver assessment tool scores between SCC and PCU. Caregivers of patients in the PCU reported worse subjective stress burden than those in the SCC (median 16 vs. 14; p = 0.002). We did not find any between-group significant differences in objective or subjective demand burden. Caregivers of PCU patients also had lower SF36 mental health scores (median 190 vs. 226; p = 0.02), but there was no significant difference in physical and general health scores. Caregivers in the SCC reported higher trust in the medical profession (median 19 vs. 17; p = 0.0076). No significant difference was found in their religious faith.
Caregiver Trust, Religious Faith, Quality of Life, and Burden (n = 172)
SF36, Short-form 36 Health Survey.
Significant multivariate analysis results are shown in Table 4. Subjective stress burden was associated with worse caregivers' objective (p = 0.01) and subjective demand burden (<0.0001), a poorer caregiver mental health (p = 0.007), lower caregiver educational level (p = 0.01) as well as with patients' higher level of anxiety (p = 0.0003) and current use of cancer treatment (p = 0.05). We also found a trend toward an association between worse subjective stress burden and shorter caregiver duration of care (p = 0.068).
Multivariate General Linear Regression Model on Subjective Stress Burden
Discussion
In this prospective cross-sectional study, we compared three dimensions of caregiver burden between caregivers of two different palliative cancer care settings: objective burden, subjective stress burden, and subjective demand burden. We found that caregivers of patients in the PCU reported a worse emotional impact in caregiving with higher levels of subjective stress burden than those in the SCC. However, no between-group significant difference was found in objective or subjective demand burden.
As expected and confirmed by our findings, patients in the PCU have worse symptom intensity and a poorer prognosis compared to those at the SCC. These patients are usually not candidates for any further active cancer treatments and have very low functionality. As a result, PCU caregivers are probably experiencing a substantial level of anticipatory grief, which in turn is contributing to the higher intensity of subjective stress burden found among them. Identifying and managing the development of grief of caregivers through a variety of methods, including supportive counseling, spiritual support, and periodic follow-up after the patient's death, are crucial to alleviate the emotional impact on the caregiver. In addition, the difference in the emotional impact may be a reflection of how caregivers process grief and distress at end of life, which makes it more important in early identification and support. Further research is needed to examine how various methods of grief processing at the end of life can affect different dimensions of caregiver burden.
On the other hand, PCU dyads are cared for by an interdisciplinary palliative care team of highly trained and experienced specialists in managing severe symptom distress and intense anticipatory grief in both patients and caregivers.31,32 This allows the caregivers to grieve freely and not be restricted by having to manage the day-to-day symptoms and activities of the patient. Therefore, their objective and subjective demand burden are not significantly different from SCC caregivers.
Patients admitted to the PCU are a very small percentage of the patients seen by the palliative care team. Even under the care of the interdisciplinary team, our findings indicate that informal caregivers of PCU patients are in considerable distress. Likely, the level of distress would be more severe in the absence of the resources provided by the PCU setting. Nevertheless, all of the PCU patients in the study were transferred from other units in the hospital. Hence, they were already under the care of the palliative care team during their hospital course or previously in the SCC or prior hospitalizations. These initial encounters with the palliative care team or other inpatient medical teams may have contributed to alleviate their level of objective and subjective demand burden.
Interestingly, caregivers of patients in the SCC reported more trust in the medical profession than those in the PCU. Prior research indicates that a normally worse perception toward the health care team may result when patients' clinical condition or prognostic information is poor. In randomized trials regarding patients' perception of physician compassion after exposure to a more optimistic and less optimistic message, patients generally favored physicians delivering a more optimistic message at the time of the message, even if the eventual patient outcome was not favorable.33,34 Hence, we expect that in situations where there is a difference between clinical scenarios, patients and caregivers would generally have a better perception of the health care professional in the more optimal scenario.
Patients' higher level of anxiety was associated with worse caregiver subjective stress burden. The correlation between patient symptoms, including those of the psychological area, and caregiver emotional suffering has been described by prior research done by our group and others.35,36 In a study to test the feasibility of using the ESAS to assess caregiver symptoms, for example, we found that both anxiety and depression were associated with their corresponding items in the caregiver ESAS. 35 Hence, for clinical practice, the presence of psychological symptoms in patients should prompt an assessment of caregiver emotional health to identify those distressed and provide them with adequate psychosocial interventions.
We also believe that patients' distress is mediating the association between patients' use of current cancer treatment and caregiver emotional burden. The use of chemotherapy in patients with advanced cancer, even for those with good performance status, has been associated with patients' worse physical and psychological distress as perceived by caregivers. 37 Perceiving this distress could emotionally affect the caregivers.
Caregivers with lower education levels reported worse subjective stress burden. Some explanations might justify this finding. Caregivers with higher education levels may develop better skills in formulating solutions and adjusting to different challenges in caregiving. In addition, they may be able to comprehend more easily the health information provided by the health care team or other educational sources, which can facilitate the application of this knowledge to fulfill patients' needs. Furthermore, they may be more financially stable and, hence, able to afford more resources through the caregiving process.
Low income has been frequently associated with worse quality of life, burden, and psychological distress among cancer caregivers.38,39 While it is not feasible to require caregivers to complete higher levels of education, providing basic and easily understandable skills and training in caregiving may allow for a reduction in caregiver burden. Further research is necessary to determine the impact of these measures on caregiver burden.
We also found a trend toward an association between shorter duration of caregiving and worse subjective stress burden. Some cancer patients experience a faster decline in their health condition because of rapidly progressive disease, resulting in a shorter duration of caregiving. Similar concerns have been expressed in other studies relating to informal cancer caregivers.40,41 We hypothesize that the sudden changes in the condition of these patients determine higher levels of caregiver emotional distress; more physical requirements; and a shorter time for grief preparation.
Nevertheless, analyzing only the total duration of caregiving provides a superficial view of the interaction between caregivers' activities and caregiver burden development. 42 Previous studies suggest that the impact of caregiving duration on caregivers may be mixed and other variables such as the type and quantity of the tasks performed may also be concurring to it.43,44 More studies are needed to characterize how caregivers' activities correlate with caregiver burden.
Other variables associated with subjective stress burden were objective and subjective demand burden as well as SF36 mental health. The association between objective and subjective burden found in our study was weak; pointing in the same direction of other studies that show, although correlated, the association of both types of burden is not strong.45,46 This indicates that different contributors influence the two burden types. Further research should develop specific interventions to relieve each of these burden dimensions.
On the other hand, subjective demand burden was moderately associated with subjective stress burden, which suggests that a negative patient/caregiver relationship increases caregiver emotional burden. Others have found a similar correlation. 47 For example, in a study evaluating the frequency and predictors of depression among spouse caregivers of advanced cancer patients, Braun et al. found that relational variables, such as marital satisfaction and the type of attachment behavior, had an important contribution to depression. 48 Additional studies are needed to better characterize how the type of patient/caregiver relationship can affect the caregiver.
Finally, although mental health was inversely associated with subjective stress burden, lower scores in the SF36 represent worse health status, while higher scores in Montgomery–Borgatta burden scale represent a more intense burden. Therefore, this finding is expected as both subscales are measuring similar dimensions of suffering.
The results of this study demonstrate that caregiver burden may present in various degrees regardless of patient care setting. In addition, caregiver burden may be reduced with the support of health care teams by essentially assuming certain caregiver roles, particularly health-related activities, which in turn reduces caregiver tasks and allows caregivers the opportunity to grieve and spend time with their loved ones. 3
However, for caregivers taking care of patients outside of the hospital, the health care team support is not readily available. Therefore, it is important to strengthen the social structures of health care system responsible to provide caregiver support and training programs to provide caregivers with the skills and knowledge to care for patients outside formal health care settings. 49 This would allow primary caregivers of advanced disease patients' to have the knowledge to address patient symptoms and other issues and receive help with certain caregiver tasks or at the very least, a temporary respite to relieve their burden.
Although prior studies testing various caregiver interventions, such as psychoeducational interventions and skills training, have demonstrated mixed results, benefits have been shown in reducing burden and improving quality of life, coping skills, and self-efficacy.49–51 Moreover, incorporating technological advances into caregiver support is encouraging to see how they can improve caregiver stress.40,50 However, further research is needed to determine optimal timing, intensity, and mode of delivery of these interventions, as well as applicability to a more diverse cultural and ethnic caregiver population.50,51
This study has some limitations. We were not able to enroll the 200 patient-caregiver dyads initially planned due to the onset of the COVID-19 pandemic. Although we accrued 85% of the target goal, reaching 100% may have potentially offered further significant adjustments and insights to the results. Also, patients with cognitive impairment were not included. Hence, we did not capture the impact of cognitive disturbances on caregiver burden. Including these patients, however, would likely disproportionately affect the PCU dyads as patients at end of life are commonly affected by neuropsychiatric syndromes such as delirium, a condition well known to be associated with caregiver distress. 52 In addition, all of the PCU patients in the study were transferred from other units in the hospital where the patients and caregivers have already received care and support from other medical and nursing teams. We were not able to examine patients who were admitted directly to the PCU from the outpatient setting, which may affect the level of objective and subjective demand burden.
For future studies, in line with this study's results, it would be interesting to compare caregiver burden and distress in the outpatient center, inpatient hospital units, and the hospice population, including both inpatient and home hospice care. More importantly, after identification of caregiver distress and burden is made, more studies are needed to evaluate the targeted application and the corresponding impact of existing interventions to alleviate caregiver suffering.
Conclusion
Caregivers caring for patients in the inpatient PCU reported more emotional impact than those in the outpatient area. However, this difference did not extend into the demands and responsibilities felt by the caregivers. There may be additional factors that impact caregivers who are caring for patients at the end of life, including grief, grief reaction, and intensity of interventions to manage these. Further research testing tailored interventions to alleviate specific caregiver burden dimensions is needed in both inpatient and outpatient palliative cancer care settings. Precedent settings of care may also affect how caregivers are coping in their current situation. Finally, more studies investigating caregiver burden in hospice care compared to acute medical care settings are necessary to tailor interventions in reducing caregiver burden as they transition care settings.
Footnotes
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.