
Abstract
Background:
Methadone is frequently used for the management of complex pain at the end of life by palliative care specialists. It is also used in low doses as an add-on therapy to chronic opioid treatment of cancer-related pain, usually with good effect, and without any reported severe adverse effects. However, there are few reports of switching from ketamine to methadone.
Case:
We report a case of a patient with rectal cancer and intractable pain. Switching from ketamine to methadone to maintain analgesia was successfully carried out without impacting activities of daily living. Established measurement tools, such as numerical rating scale, Douleur Neuropathique, Functional Independence Measure, and Barthel Index, were used.
Conclusion:
Switching from ketamine to methadone may be beneficial in relieving refractory cancer-related neuropathic pain without decreasing functioning.
Introduction
Prevalence of pain in patients with cancer remains high,1,2 and pain has a significant impact on their functioning. Uncontrolled pain is incompatible with satisfactory quality of life and it is well recognized that persistent pain impairs the daily life and social interactions of the patients. 3 Opioids are indicated for moderate to severe cancer-related pain management. These include fentanyl, hydromorphone, oxycodone, morphine, and methadone. 1
Methadone is a synthetic opioid that was developed in 1937 in Germany. It has agonistic action at the μ opioid receptor (receptor involved in supraspinal analgesia) and δ opioid receptor (involved in spinal analgesia). In addition, methadone's
Herein, we report a case of successful management of rectal cancer with intractable cancer pain. This case involved switching from parenteral ketamine to oral methadone as “add on” opioid.
Case Description
The case report was approved by the Institutional Review Board of Seirei Sakura Citizen Hospital.
A 62-year-old man (height 172 cm, weight 53.2 kg) presented with recurrent rectal cancer metastatic to the lung, and had previously undergone laparoscopic low anterior resection. He was admitted to our palliative care unit (PCU) for management of severe cancer-related pain.
On admission to our PCU, he displayed an Eastern Cooperative Oncology Group (ECOG) performance status of 1, and there was no dysfunction of the liver or kidney. His pain was continuous, sharp, and perineal. Pain was also present in the hip due to local recurrence, and his pain intensity score was 6–8/10 (10-point numerical rating scale [NRS]). He had been prescribed serval analgesics (acetaminophen 2400 mg PO, loxoprofen 240 mg PO, morphine 160 mg per day IV, tapentadol 50 mg PO, pregabalin 450 mg PO, duroxetine 20 mg PO, and ketamine 50 mg per day IV) for pain management, but the pain remained unrelieved and prevented him from assuming a sitting position. After admission, an intrathecal phenol block was administered for managing his perineal pain. Consequently, the perineal pain disappeared and he could be in a sitting position. Owing to this improvement in his condition, some analgesics were gradually reduced and some were discontinued (tapentadol, pregabalin, and duloxetine were discontinued, whereas loxoprofen was reduced). Rehabilitation was then initiated to improve or maintain his activities of daily living (ADL).
Over the next month, his buttock pain worsened because of pain recurrence. The pain intensity score was 6–8/10 using the same rating scale as used previously. Morphine and ketamine were uptitrated frequently to achieve adequate pain control (morphine 2112 mg per day IV, ketamine 156 mg per day IV); however, their combined analgesic effect was inadequate. The pain remained continuous and sharp, with a shooting pain below the right S1 area. The patient also had persistent numbness, allodynia, and hypoesthesia. Sensation of pinprick, cold, and touch were measured; all of them had decreased (loss of cold sensation score 5/10 [NRS], pinprick score 5/10 [NRS], and touch score 5/10 [NRS]). We also administered the Douleur Neuropathique 4 (DN4), 7 and was found to be 6/10; therefore, the pain was diagnosed as neuropathic pain.
We consulted the Department of Radiation Oncology and the patient received radiation to the sacrum (60 Gy/30Fr). The radiation caused a reduction in the severity of his pain but was associated with somnolence because of the high doses of analgesics administered. Therefore, we decreased analgesics step-by-step; first, morphine was reduced by 20%–30% every two days and discontinued after two weeks (Fig. 1). We changed morphine 30 mg per day IV to the sustained-release oxycodone 40 mg PO BID (Fig. 1). After opioid switching, we also decreased ketamine, but his pain increased several hours after the ketamine reduction and did not improve with supplemental or rescue doses of oxycodone 5 mg as needed. He also noted that the numbness, allodynia, and hypoesthesia also increased. Therefore, we determined that this pain syndrome was likely worsening neuropathic pain. We considered increasing ketamine again, but the patient declined this line of treatment due to need for intravenous administration of ketamine (oral administered ketamine is not possible in Japan). We also considered using other analgesics for the control of neuropathic pain. However, the patient was disinclined from using adjuvant analgesics (e.g., gabapentinoids and duloxetine) due to side effects and lack of analgesic benefits in the past. Since then, he had a negative impression about these classes of medications for pain. As an alternative, we suggested using methadone given its NMDA antagonism, which he was amenable to.
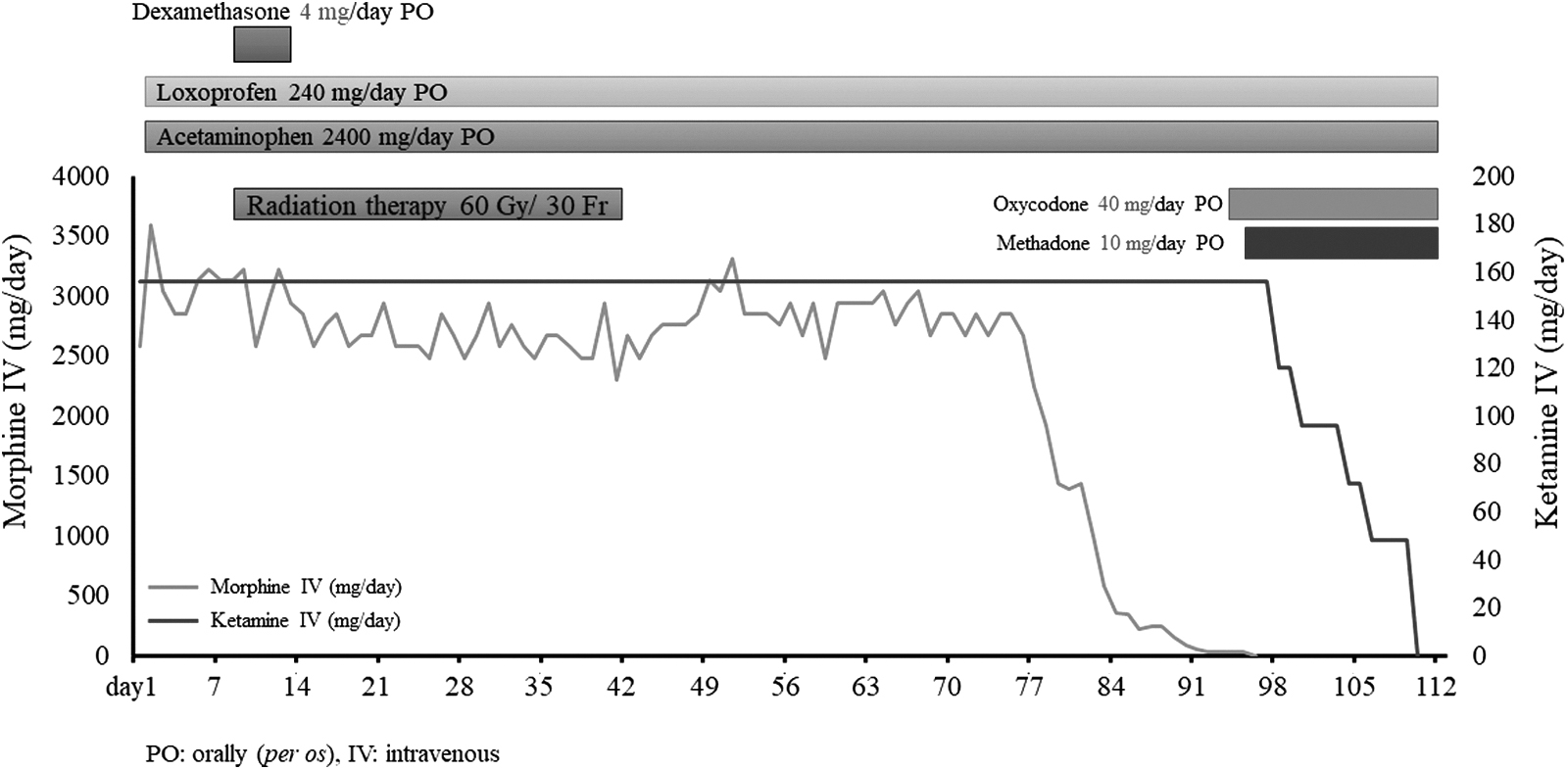
The time course of radiation therapy and analgesic switching. The radiation therapy reduced the pain after fractionated radiation over 30 days of treatment. We decreased analgesics step-by-step and switched from morphine to oxycodone. After this opioid switching, we further switched from ketamine to methadone.
We, therefore, started methadone 10 mg PO BID and ketamine was reduced by 20%–25% every two days and discontinued after two weeks. Through this line of treatment, his pain score improved from 6–8/10 to 2–4/10 (NRS), and further neuropathic pain did not appear. Because he experienced improvement in pain, he did not want to titrate it ever. Therefore, we did not titrate methadone. No withdrawal symptoms were noted. Pain intensity was then evaluated again using DN4. The score was 6/10, the remaining pain primarily being neuropathic. However, the patient claimed that his analgesia was good enough; thus, the present analgesic treatment was successful in sustained pain control.
Upon initiating rehabilitation, ADLs were measured by his physical therapists using the Functional Independence Measure (FIM) 8 and the Barthel Index (BI). 9 After radiation, FIM and BI results maintained a high score (FIM 92–98, BI 75), and ADLs of the patient were well maintained.
With this regimen, he did not develop any significant increase in pain.
He died on our PCU due to the progression of his cancer (18 months postdiagnosis).
Discussion
Methadone is a synthetic opioid and is commonly considered as an alternative to other opioids when they lose their efficacy. 10 Methadone, at low doses, has recently become more common in palliative medicine practice. 11 Switching from other strong opioids to methadone as an alternative, based on its μ opioid receptor action, has been reported,5,6 and methadone has shown superiority in a single trial for neuropathic pain in head and neck cancer. 4 However, there are few reports of switching from ketamine to methadone to provide antagonism of the NMDA receptor.5,6
In the case of our patient, the cancer-related pain was reduced by radiation, and hence, we decreased morphine dosage and switched to oral oxycodone. However, after opioid rotation from morphine to oxycodone, we attempted to decrease ketamine, but his pain increased again and he was ultimately transitioned off of ketamine to methadone.
This outcome suggests that methadone's unique properties, for example, NMDA antagonism, may have played a significant role in relieving his neuropathic pain, previously attenuated by ketamine. These findings suggest that, for intractable cancer-related pain where opioids are not completely effective, for example, with some types of neuropathic pain syndromes, we should consider NMDA antagonists. In addition, switching from ketamine to methadone as an “add on” analgesic, especially in settings where oral ketamine is not available, may be beneficial.
The acceptance of methadone has been increasing for palliative care and pain management, especially in the case of advanced stages of cancer and in the case where neuropathic pain is indicated and other opioids are rendered ineffective. 12 Methadone is frequently used for the management of complex pain at the end of life in specialized palliative care in Sweden. 13 It is mainly used in low doses as an add-on therapy to an ongoing regular opioid treatment of cancer-related pain, usually with good effect, and without any reported severe adverse effects. 14 Our present report is in agreement with the literature.13,14
Independence in ADLs is a subjective experience, and self-reporting by the patient is the gold standard for assessment. However, it is sometimes difficult to make an objective evaluation because the expression of patients may be inadequate. In our case, we performed an objective evaluation of ADL using the FIM 8 and the BI 9 by expert physiotherapists. Our FIM and BI showed high scores of 92–98/126 and 75/100, respectively, and these were derived from his adequate pain control.
Limitations of this case report include not considering the possibility that hyperalgesia may develop with abrupt discontinuation of ketamine. Mitchell has reported about generalized hyperalgesia and allodynia following abrupt cessation of subcutaneous ketamine infusion. 15 This case report mentions that possibilities of the number of NMDA receptors would have increased due to prolonged continuous infusion of the receptor antagonist ketamine. In addition, this literature suggests that the release of excitatory peptides and glutamate continues, and the NMDA receptor's change in affinity for magnesium is caused by ketamine.
Conversely, our case differs in that the originally recognized neuropathic pain exacerbation below the S2 region appeared and was not generalized.
In addition, a recent article suggests that duloxetine in combination with methadone may be more effective for neuropathic pain than as single agents. 16 However, our patient was not open to a trial of other adjuvant analgesics.
Conclusions
In this case report, switching from ketamine to methadone may be a beneficial strategy to manage intractable neuropathic cancer pain without decreasing ADL. Further controlled studies are necessary to validate this approach.
Footnotes
Authors' Contributions
Conceptualization, data curation, methodology, investigation, and writing-original draft preparation by S.M. Investigation by T.A., T.K., and H.K. Writing-reviewing and editing by H.Ko. and Y.U.
Funding Information
No funding was received.
Author Disclosure Statement
No competing financial interests exist.