
Abstract
Objective:
Me & My Wishes involves videos of persons living with dementia talking about their end-of-life (EOL) care preferences. This study aimed to examine the concordance of EOL treatment and psychosocial preferences expressed by assisted living community and nursing home residents in these videos with family and staff knowledge of preferences.
Design:
Randomized wait-list control.
Setting/Subjects:
Assisted living and nursing home residents in the United States, and their family members and caregivers.
Measurements:
Five EOL treatment preferences (cardiopulmonary resuscitation or CPR, breathing machine, tube feeding, life support, and pain treatment) and four near EOL psychosocial preferences (having family at the bedside, engaging in faith practices such as prayer, having a pet at bedside, and engaging in activities such as being read to or listening to music) extracted from residents' videos and captured through family and staff surveys.
Results:
Thirty-six resident videos were shared with family (N = 50) and staff (N = 38) during care plan meetings. Concordance between residents' stated EOL treatment preferences and family and staff knowledge improved, with results showing a treatment effect at time of sharing the video (family: Beta = 0.21, p < 0.001; staff: Beta = 0.35, p < 0.001).
Conclusion:
Our findings indicate that sharing Me & My Wishes videos improved family and staff concordance of EOL psychosocial and treatment preferences for assisted living and nursing home residents living with dementia. Personalized videos conveying resident preferences can help informal and formal caregivers understand the resident as a person and foster concordant care. Clinical Trial Registration Number NCT03861429.
Introduction
More than two million people in the United States reside in long-term care (LTC) settings, such as assisted living communities and nursing homes. 1 More than half of LTC residents are living with Alzheimer's disease or a related dementia and one-third die from it.2,3 Despite the importance of understanding care and end-of-life (EOL) preferences for LTC residents living with dementia, routine approaches for eliciting and documenting such information are underdeveloped.4,5 Some resident preferences and advance directives are collected through standardized assessments at admission, but few LTC settings personalize the approach to ascertain preferences of residents with dementia while they are able to convey them. 6
Ascertaining resident preferences and sharing them with informal (family) or formal (staff) caregivers is important so that care preferences of persons with dementia are honored, even when the caregivers have different opinions of what care should include or entail. 7 Because family, in particular, may serve as proxy decision makers for persons living with dementia, ensuring they understand residents' preferences is vitally important to assure that care is concordant with the residents' wishes. 5
Previous research has shown that persons living with mild-to-moderate dementia can provide information about care preferences in advance care planning conversations.8–13 When wishes are shared and documented before cognition declines, residents feel involved, family caregivers' feel prepared, and providers' decision making may be better informed to provide resident care consistent with those wishes.5,14 Although care preferences can be documented in advance directives, more personalized methods, such as videos, can complement such documentation and also include information about a residents' values and preferences that foster person-centered care. Increased understanding of values and preferences in everyday and EOL care can help inform future decision making, comprehensive care planning, and delivery of concordant care. 15
We previously established the feasibility and acceptability of the Me & My Wishes intervention—a video recording approach for viewing, listening, and discussing daily and EOL care preferences of residents living with dementia. 16 Our protocolized structured Me & My Wishes conversation guide ensures the video interviews elicit more detailed resident preferences for EOL care that are often missing from other assessment processes 17 and which may improve the alignment of care with those preferences. In this Stage II 18 efficacy trial, we examined the concordance of the EOL preferences expressed by residents in their Me & My Wishes videos with family and staff understanding of residents' EOL preferences.
Methods
We employed a randomized wait-list control design to examine the concordance of EOL psychosocial and treatment preferences among LTC residents living with dementia, families, and staff. Assisted living communities and nursing homes were assigned to either an intervention group (resident videos recorded and shared) or a wait-list group (resident videos recorded and shared after all data from the intervention group were collected). The study was approved by the University of Utah Institutional Review Board and registered at ClinicalTrials.gov.
Sample and settings
Utilizing partnerships with the Brown University Center for Long-Term Care Quality & Innovation and American Health Care Association state affiliates, we recruited three licensed assisted living communities and five nursing homes located in the Pacific Northwest of the United States. All sites were for-profit, ranged in size (35–80 beds) and provided 24-hour care, such as activities of daily living. Care in assisted living was more focused on personal care (e.g., assistance with medications) and care in nursing homes provided a greater amount of personal care and other medical services such as rehabilitation. The timing of care plan meetings vary state to state for assisted living communities; however, all sites in our study held resident care plan meetings quarterly, which is typical for nursing homes.
Residents
Residents were eligible for the study if they were living with Alzheimer's or related dementias, able to make themselves understood and be understood by others, resided at the facility for at least two weeks, were ≥65 years of age, and English speaking. Nursing home residents also needed to be LTC residents (defined as anticipated stays of >100 days) and score between 8 and 15 on their most recent Minimum Data Set Brief Inventory of Mental Status. 17 We excluded residents if they were severely cognitively impaired, had limited communication capacity (e.g., aphasia), or unable to complete the consent process. Each site pinpointed a facility champion (e.g., social services director) who identified eligible residents and asked them if they would be interested in talking to a researcher about study participation. A study coordinator completed the consent process with enrolled residents, including a teach-back component (i.e., recapping participation requests in their own words) and signing the consent form.
Family
Family members identified by the consented resident were eligible to participate in the study if they were English speaking, willing and able to watch the resident's video and complete surveys. Family members were eligible to participate regardless of their ability to attend the care plan meeting to view the video.
Staff
Staff members were eligible for study participation if they were identified as a care plan team member, English speaking, and willing to both integrate the resident's video in the care plan meeting and complete surveys. A staff care plan team member, such as a social services director, could be the same person for all residents in a facility, whereas other care team members such as a nurse may differ.
Me & My Wishes intervention
Me & My Wishes videos convey both every day and near EOL preferences. A study coordinator facilitates structured video recorded conversations utilizing the Me & My Wishes conversation guide with residents. The video is structured into four parts: About Me, Preferences for Today, Preferences for Medical Intervention and End-of-Life Care, and Afterthoughts. 19 Conversations cover learning about the resident as a person as well as their preferences for everyday care and activities, medical intervention, and psychosocial preferences near EOL and after death preferences (e.g., desire for funeral). Residents approve their personalized video, which is then shared with the care plan team and resident-identified family members or friends.
At the care plan meeting, a member of the care plan team initiates video viewing and facilitates a conversation with the resident, family, and care team to clarify or reiterate preferences most important to the resident. Findings from our previous study supported the feasibility and acceptability study supported this video recording approach for viewing, listening, and discussing residents' preferences for daily and EOL care, which is important in the LTC context and a facility's ability to integrate into care plan meetings as well as the mandate for person-centered care. 16
Measures
We selected nine potential care preferences to evaluate. Five were EOL treatment preferences (i.e., cardiopulmonary resuscitation or CPR, breathing machine, tube feeding, life support, and pain treatment) and four were near EOL psychosocial preferences (i.e., having family at the bedside, engaging in faith practices such as prayer, having a pet at bedside, or engaging in activities such as being read to or listening to music). We extracted the nine preferences from the resident videos. Family and staff surveys asked whether or not the resident would want each of the nine care preferences. For example, “My relative would want to be fed artificially (through a tube) if he/she can no longer take food and drink normally.” We coded preferences from the videos and surveys as yes, no, don't know, or missing. Concordance occurred when the coded preferences in the resident's video and staff and family member response matched.
Procedures
We followed our standardized procedures for conducting the Me & My Wishes conversation as well as editing and sharing the video.16,19 Working with the facility champion, a study coordinator conducted the video recording and reviewed it with the resident for approval. Resident videos, on average, were 16.32 minutes. A member of the care plan team initiated video viewing and facilitated conversation in the care plan meeting. We administered the family and staff surveys at baseline, second baseline (wait-list group), time of sharing and 90 days post-video viewing. To ensure consistency, one research team member extracted the nine EOL preferences (five treatment and four psychosocial) from the resident videos. We discussed any questions or uncertainties related to extractions in team meetings.
Analysis
Analyses were conducted using SPSS Version 24.0 (SPSS, Armonk, NY) using an intent to treat approach. Multilevel linear regressions (generalized estimating equations [GEE] with an autoregressive (1) working correlation matrix) were fitted to assess concordance of preferences between the resident videos and staff and family surveys at three (intervention group) or four (wait-list control group) time points. The models account for the repeated measures (three or four time points), correlated, data structure per person. Because this study used a wait-list control design, data include the initial baseline data for both groups and second baseline data for the wait-list group. An additive model was conducted with contrast coding for each time point, treatment, and follow-up effects.
This allowed us to compare the groups by the different times they received the video, with Time 1 (Baseline) as the reference category. For example, a participant in the immediate group at time of video sharing would receive contrast coding: Time 2 (1), Time 3 (0), Time 4 (0), Treatment (1), and Follow-up (0). Whereas a participant in the wait-list (control) group at time of video sharing would receive contrast coding: Time 2 (0), Time 3 (1), Time 4 (0), Treatment (1), and Follow-up (0). We stratified our analysis by the three different types of participants—residents, family members, and staff members. In addition, the nine resident EOL preferences were descriptively analyzed for concordance against family and staff surveys.
Results
Figure 1 illustrates the flow of enrollment and Table 1 shows participant characteristics. We enrolled 50 residents; our attrition rate was 28%. The 36 residents who completed the intervention on average were 78.4 (standard deviation [SD] = 9.4) years of age and were more likely to be female, widowed, non-Hispanic, and white. Almost half (47.2%) had some college and 27.8% had graduated college or had postgraduate education. Family members (N = 50) on average were 60.7 (SD = 11.5) years of age. Most were female, married/partnered, non-Hispanic, and white. Nearly half of the family caregivers were adult children followed by siblings and the category “Other.” Staff (N = 38) were mainly female, non-Hispanic, and white. Sixty-four percent of staff in this sample had a college education and 13.2% reported having a postgraduate or professional education.
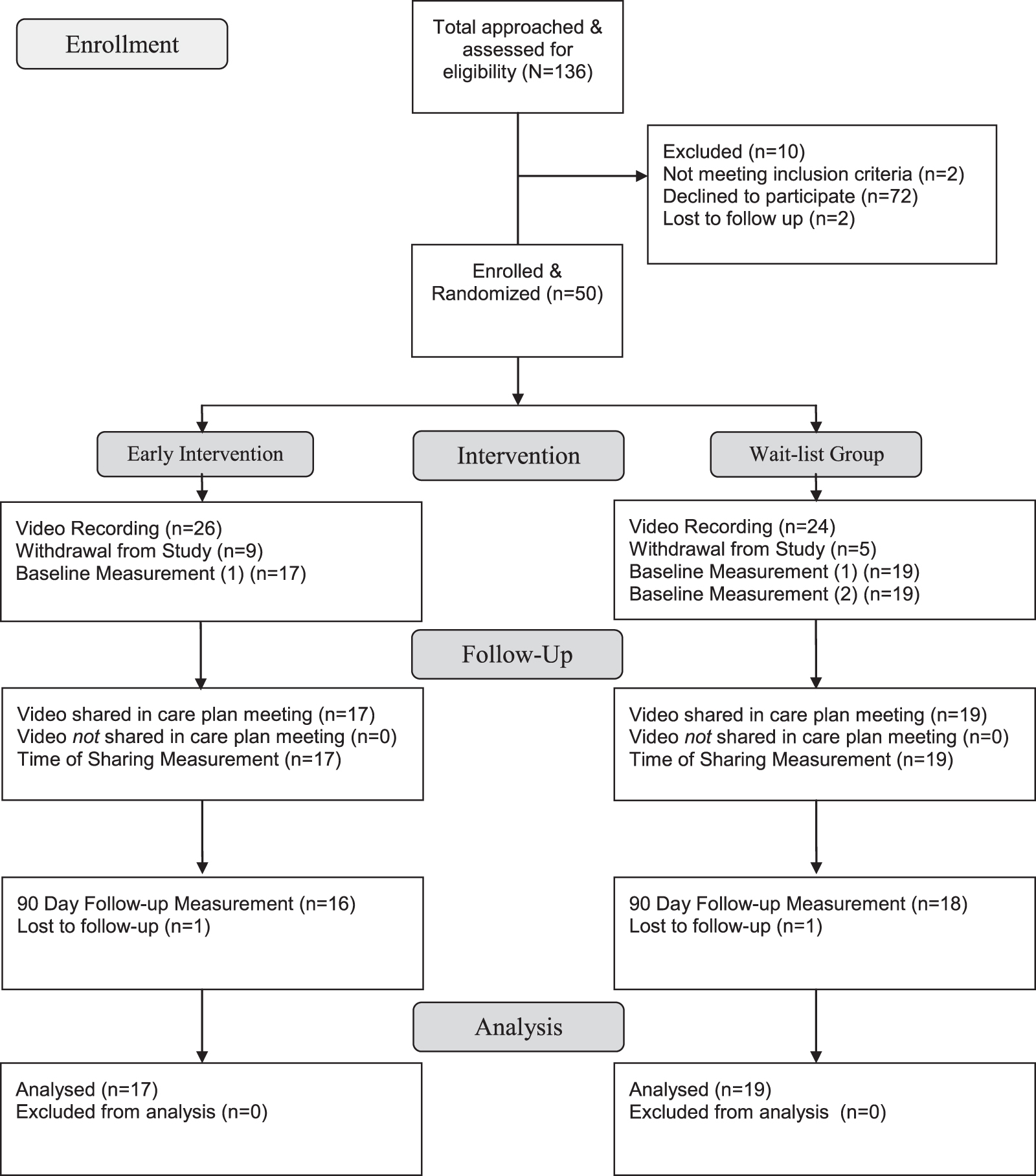
Me & My Wishes resident enrollment flow.
Demographics
SD, standard deviation.
Concordance of EOL preferences
We evaluated the impact of our Me and My Wishes Video intervention on family and staff concordance with resident's EOL preferences (EOL treatments and psychosocial preferences). Table 2 shows parameter estimates for all GEE models. For EOL treatment preferences, there was a treatment effect (time of sharing the video) (Beta = 0.21, p < 0.001) within family members. Thus, concordance between resident's stated preferences for EOL care and family members' knowledge of the preferences increased at treatment. Calculated values (Estimated Marginal Mean) for time of treatment in the early intervention group was 57.7% (standard error [SE] = 4.1%) and 66.1% (SE = 5.3%) in the wait-list group as compared with the overall baseline rate of 43.4% (SE = 4.2%).
Concordance with End-of-Life Psychosocial and Treatment Preferences: Fixed Effects from General Estimating Equations
Effect coding (1, 0; presence or absence) was used for each fixed effect. Time 1 (baseline) is the reference category. Example, goal of care documentation for a participant in the immediate group at time of video sharing would receive effect coding: Time 2 (1), Time 3 (0), Time 4 (0), Treatment (1), and Follow-up (0). Whereas a participant in the wait-list group at time of video sharing would receive effect coding: Time 2 (0), Time 3 (1), Time 4 (0), Treatment (1), and Follow-up (0).
EOL, end-of-life.
The concordance rate dropped back to baseline rates at follow-up, as indicated by a nonsignificant follow-up parameter (Beta = 0.07, p = 0.360). We also found a treatment effect at time of sharing the video for staff (Beta = 0.35, p < 0.001). Calculated values for the early intervention group was 63.5% (SE = 3.5%) and for the wait-list group, 54.6% (SE = 4.7%) versus a baseline rate of 28.9% (SE = 3.7%). Staff concordance remained higher than baseline at follow-up (Beta = 0.40, p < 0.001); calculated values for the early intervention group was 59.6% (SE = 5.3%) and the wait-list group was 45.8% (SE = 4.8%).
For EOL psychosocial preferences, there was a trend of treatment effect (time of sharing the video), Beta = 0.09, p = 0.081 within the family group. For staff, there was a treatment effect, Beta = 0.29, p = 0.001, showing increased concordance rates. The calculated value for the early intervention group was 76.3% (SE = 2.8%) and the estimated marginal mean for the delayed intervention group was 89.5% (SE = 3.7%) versus a baseline rate of 44.4% (SE = 4.7%). The treatment effect for increased concordance on EOL psychosocial preferences did not hold and returned to baseline rates at follow-up, Beta = 0.08, p = 0.497.
We also examined the concordance by type of EOL treatment and psychosocial preferences. Tables 3 and 4 show the preference concordance rates between residents, family, and staff over time. Pain treatment had the highest concordance between the resident's video and family and staff surveys; life support had the least concordance. Having family at the bedside had the highest concordance between groups when comparing with the resident videos at all time points; having a pet at the bedside was the least concordant.
Percentage Concordance of End-of-Life Treatment Preference between Resident Videos and Family and Staff Surveys over Time
CPR, cardiopulmonary resuscitation.
Psychosocial Preference Congruence Rates between Resident Videos, Family, and Staff Surveys over Time
Activities (e.g., reading, playing music, and watching television).
A considerable proportion of the discordant responses between resident preferences and family and staff knowledge occurred when family or staff answered, “I don't know.” For example, before sharing the video, family replies of “I don't know” accounted for about half of the discordant responses, including 46.3% of EOL treatment responses and 52.2% of psychosocial preference responses. At the time of sharing, family replies of “I don't know” accounted for 15.2% and 25.6% of discordant responses related to EOL treatment and psychosocial preferences, respectively; at 90 days follow-up they accounted for 15.3% and 27% of discordant replies to EOL treatment and psychosocial preferences.
We observed a similar pattern with staff. Before sharing the video, staff replies of “I don't know” accounted for 61.9% and 77.9% of discordant responses of EOL treatment and psychosocial preferences, respectively; at time of sharing, they accounted for 12.8% and 17.7% of discordant responses in EOL treatment and psychosocial preferences, respectively. However, at follow-up, “I don't know” responses increased and accounted for 22.2% EOL treatment and 51.9% of psychosocial discordant responses.
Discussion
We found the Me & My Wishes intervention of sharing resident videos of care preferences in care plan meetings efficacious in improving family and staff concordance of understanding the EOL psychosocial and treatment preferences for assisted living community and nursing home residents living with dementia. Our findings align with previous research, including ours, that has shown that persons living with mild-to-moderate dementia are able to express their preferences for everyday and EOL care, and that advance care planning conversations have value.9–13,20 In addition, older adults living with mild-to-moderate dementia can respond to questions about values and preferences related to quality of life, and treatment preferences such as a breathing tube, and can identify a surrogate decision maker.10,13
In our descriptive analysis, we found discordance in all areas with the highest discordance related to the preference of receiving life support or having a pet at the bedside. Family and staff response of “I don't know” to a preference before video sharing accounted for nearly half of the discordance in treatment preferences for family and more than half of the discordance in treatment preferences for staff. The percentage of “I don't know” responses by family and staff for EOL and psychosocial preferences were less frequent at time of sharing and follow-up, suggesting family and staff caregivers were more informed about residents' preferences after viewing their videos. However, concordance, especially for family members, was not maintained at follow-up and possibly demonstrates that family know some preferences but not others. 21
Staff discordance may be explained in part if staff members completed study surveys without accessing the medical record. We recognize that many staff appropriately look in the medical record to identify the residents' preferences—a good practice as staff care for many residents simultaneously and are not expected to remember all the nuances of their preferences. Me & My Wishes provides residents an opportunity to convey their preferences, although sometimes their responses are ambiguous. Prompting further conversation with the resident to clarify any discrepancies and documenting the conversation in the resident's chart would be a best practice when the resident, care team, or family members report “I don't know” about EOL preferences.
Our findings demonstrate that Me & My Wishes can improve concordance and highlight the need for continued conversations among residents living with dementia, their family, and staff caregivers. 16 Reviewing care plans with residents quarterly is already a part of regulation, but may not always happen consistently or include the nuances of psychosocial preferences near EOL. To ensure person-centered care is delivered in concordance with the preferences of residents with dementia, their preferences must be routinely assessed and documented to identify changing needs.20,22 Me & My Wishes videos are designed for ongoing conversation. The four modules do not need to be viewed at one time; one could be viewed during each quarterly care plan meeting. In the event of a significant change, staff could review the most relevant module. Using Me & My Wishes videos routinely could facilitate conversation among residents, family, and staff and identify changing preferences.
Barriers to conversations include the assumption that caregivers know the resident or the resident assumes their caregivers know them, 23 but our findings suggest that knowing may not be enough as preferences are nuanced. It is possible that residents' decisions of EOL treatment preferences were influenced by acceptable characteristics of the treatments such as if they were temporary, would relieve suffering, ensure a positive outcome, or enabled a return to baseline health. 7 Organizational barriers such as the structure of the care plan meeting (e.g., time allotted for each meeting) and team members focused on completing the checkboxes (or current care needs) may influence participants' ability to engage in meaningful conversation. Furthermore, care teams may lack communication skills to engage residents and families in ongoing conversations about preferences. 5
Improved understanding of the nuances that accompany preferences potentially improves family and staff knowledge of preferences, which increases the likelihood of providing care and that supports both resident preferences and family caregivers who are concerned about decision making. 24 Although many residents with dementia may already attend their care plan meeting, our findings suggest that sharing their video during the meeting provides an opportunity to ask residents about their preferences or to clarify preferences, for example when residents convey limitations or misunderstanding about treatments.
Concordance may further improve if parts of the video are shown routinely to spark conversation about preferences. Participation in the care plan meeting may be particularly important for staff and family caregivers who may not have had informal or interspersed remarks within casual conversations with residents over time. The coronavirus disease 2019 (COVID-19) pandemic has increased the use of, and comfort with, telehealth, including use by family members to participate in care discussions. Therefore, we hope that family participation in attending care plan meetings where the Me & My Wishes videos are shared and discussed will increase and improve care concordance.
Limitations and Future Research
The results from this analysis should be interpreted in light of the limitations. Randomization occurred at site level and despite randomizing in blocks our sites differed. For example, each site has their own culture and buy-in, which may influence interpretation of preferences.5,15 The small sample size, the majority of participants being of one racial group (white), and one geographic region limits generalizability. Despite a small sample size, we did detect statistical significance. Because nursing home champions provided a list of eligible residents, rather than researchers conducting a chart review, there may be recruitment bias.
Participant bias may have occurred among all groups. For example, residents and staff who participated in the study may have wanted to engage in conversations. The definition of life support and breathing machine was left open to interpretation by the residents, family, and staff, which may have led to discordance between the groups. We did not examine dialysis or hospitalization and considering these preferences in the future may be helpful.
Future research recommendations include greater representativeness of the study population, examining the documentation surrounding nuanced EOL treatment and psychosocial preferences, and if engaging residents in repeated conversations maintains concordance over time. More specifically, studies will be designed to address lack of concordance (e.g., interviews when staff/family's understanding is not aligned with resident's video; staff training to lead conversations and address “I don't know” responses). Interviews with staff and family may help explain why the understanding or knowledge of preferences was not maintained at follow-up or why conversation was not documented. A larger and/or longer study could also examine actions taken by staff or family compared with their perceived understanding. Finally, establishing a specific place in the medical record to document care conversations would allow information to be queried and compared with regulatory guidelines.
Conclusion
Sharing Me & My Wishes videos in care plan meetings improved family and staff concordance of EOL psychosocial and treatment preferences for assisted living community and nursing home residents living with dementia. These findings build on prior Me & My Wishes research demonstrating that engaging residents in discussion about their preferences promotes person-centered care, can be accomplished by sharing videos during care plan meetings, and is feasible within the established workflow. Because informal caregivers, particularly family, may serve as proxy decision makers for persons living with dementia when they are no longer able to communicate, ensuring they understand residents' preferences is vitally important. As the COVID-19 pandemic heightened the importance of advance care planning, this may be a promising intervention to facilitate conversations and improve goal-concordant care.
Footnotes
Authors' Contributions
Study concept and design by G.L.T. and B.W. Acquisition of data by G.L.T. and R.R.B. Analysis and interpretation of data by G.L.T., B.W., S.N., and R.R.B. Drafting and critical revision of the article for important intellectual content by G.L.T., S.N., R.R.B., and B.W.
Acknowledgments
The authors are appreciative of Ms. Emily Shreefter for collecting much of the data and to the residents, families, and staff for participating in the study. Thank you.
Funding Information
This study was supported by the National Institute on Aging (R21AG058094-01A1). S.N. was supported by the National Institute of Nursing Research of the National Institutes of Health Award under award no. T32NR013456.
Author Disclosure Statement
No competing financial interests exist.