
Abstract
Background:
Advance care planning (ACP) is recommended for all patients with cystic fibrosis (CF), yet clear implementation guidelines do not exist.
Methods:
The University of North Carolina Adult CF Care Team developed a process to implement semistructured multidisciplinary outpatient ACP meetings as routine care for patients with CF. Premeeting and post-meeting surveys were used to elicit patients' attitudes toward ACP.
Results:
Twenty-seven adults with CF completed a face-to-face ACP meeting, and 13 completed both surveys. Following the multidisciplinary ACP meeting, overall scores for understanding of ACP topics improved by 4.5 points (p = 0.003).
Conclusion:
We successfully implemented sustainable ACP meetings for adults with CF and found increased comfort with ACP and documentation of wishes after ACP meetings. It is important for CF care providers to meet the needs of this patient population by ensuring that ACP is in place before crisis situations.
Introduction
The Cystic Fibrosis Foundation (CFF) and European CF Society recommend multidisciplinary advance care planning (ACP) for all adults with cystic fibrosis (CF).1,2 The 2020 consensus guidelines on management of advanced CF lung disease 3 also emphasized the need for frequent discussions around goals of care as the disease progresses. Formal ACP results in more frequent documentation of treatment preferences and advance directives, which in turn help to guide family members and the treatment team when patients can no longer state their preferences. 4 Acknowledgment and support for the crucial role of caregivers are paramount.3,5
Practices vary widely among institutions, and a meta-analysis of studies of palliative care in CF demonstrated that many people with CF have not engaged in ACP discussions at all, while others wait until the final weeks of their life. 6 A recently published cross-sectional survey suggested that most people with CF would prefer to discuss goals of care while in a stable disease condition and with trusted members of their outpatient team. 7 In addition, Sawicki et al. found that completion of an advance directive was significantly more likely to occur when a clinician asked directly about end-of-life wishes. 8 People with CF express a desire to be heard and seen, to understand their personal illness trajectory, and to receive practical resources for managing stress, 9 thus underscoring the need to equip team members for these discussions.9,10 Often these crucial aspects of self-care are overlooked during a busy clinic visit.
The Adult CF Care Team at the University of North Carolina at Chapel Hill (UNC) designed an intervention formalizing ACP meetings. The goals of this resource-limited initiative were to assess the feasibility of a semistructured interdisciplinary meeting in an outpatient clinic setting and to examine how patients' perceptions of end-of-life care changed in response to this intervention.
Methods
The target demographic for the initial implementation was individuals with CF who were 40 years of age or older or who had a forced expiratory volume in one second (FEV1), less than 40% predicted, indicating severe lung disease. While we recognized the importance of ACP for all people with CF, our center is large (>350 adults), so we began with patients at the highest risk of respiratory decompensation. However, any patient expressing interest was eligible to participate. Patients received information about the availability of ACP meetings through newsletter or in person by a CF team member. A resource book created by the QI team was provided before the scheduled meeting; this book (available as Supplementary Data) contained information on end-of-life symptoms, palliative medications, lung transplant consideration, advance directives, and treatment options for medical emergencies, such as CPR. It also included validated tools for end-of-life discussions and outlined a framework for the upcoming ACP discussion.
Interested participants were scheduled for ACP meetings on the same day as their next clinic visit, but in a time slot specifically reserved for this discussion. This allowed for a separate billable visit that is covered by North Carolina Medicaid and most insurers. 11 ACP meetings were scheduled as either the first or last appointment of the day, allowing the multidisciplinary team to dedicate time without distraction by other clinical responsibilities. Only one meeting was scheduled per clinic day to avoid overburdening the care team. Discussions were scheduled 2–3 months in advance to allow patients to invite family member/caregivers to participate. Participants included the patient and his/her identified support people, as well as the primary pulmonologist/advanced practitioner, nurse, social worker, and other members of the multidisciplinary team as needed. The meetings lasted ∼60 minutes and were moderated by the social worker and guided by each patient's identified topics of interest.
Meetings were scheduled in a conference room rather than an examination room to emphasize collaborative discussion rather than a traditional clinic visit. Introductions occurred first, to ensure all family members understood the role of each team member. Unless guided otherwise by the patient, meetings started with a synopsis of the patient's current health status by the CF provider, followed by questions by the patient and family. A key goal of each meeting was to ensure that the surrogate decision maker was selected and to discuss how end-of-life choices could be documented. Otherwise, the meetings did not follow a structured format, allowing the patient time to discuss the topics of highest importance to them as guided by the previously reviewed resource book. An ACP documentation note was subsequently placed in the electronic medical record, and a follow-up phone call was arranged.
A self-administered, IRB approved survey (Table 1) was provided to elicit information about patients' perceptions of end-of-life planning before and after their ACP meeting; however, completion of the survey was not required to schedule an ACP meeting. Surveys were designed by team members with expertise in palliative care, social work, and medical ethics; after review by the entire team, two adults with CF assessed the survey for face validity. Surveys were administered through REDCap 12 and results were analyzed using JMP®, Version 15 (SAS Institute, Inc., Cary, NC) statistical software. Responses were rated on a numerical Likert with 1 representing “strongly disagree” and 5 representing “strongly agree.” One question that was phrased in the negative had the scale reversed for equivalent scoring. This resulted in a scale that ranged from 12 to 60 points, with higher scores indicating a greater comfort level with ACP.
Survey Questions Were Graded on a 5-Point Likert Scale, with a Higher Score Indicating Greater Agreement with the Statement
Mean (SD) participant scores for each survey question are recorded for before and after ACP meeting. The * indicates statistically significant values.
ACP, advance care planning; CF, cystic fibrosis; SD, standard deviation.
Results
Twenty-five patients completed a face-to-face ACP meeting. Thirteen participants completed both premeeting and post-meeting surveys and were thus included in our analysis. With an average age of 34.5 years and FEV1 36.4%
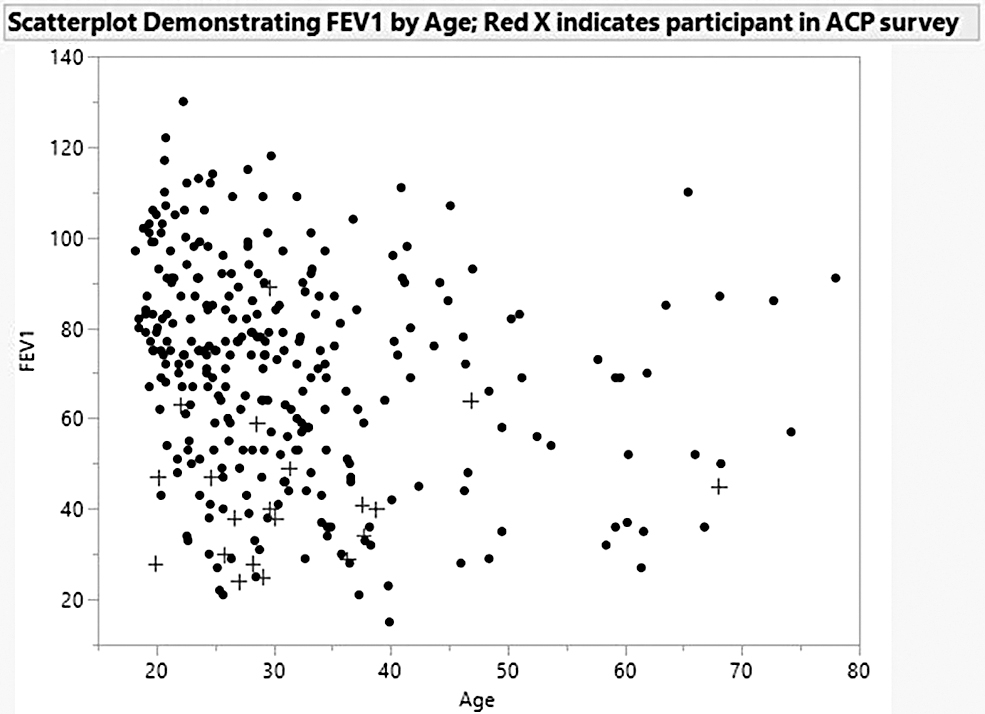
Scatterplot of FEV1 percent predicted by age at UNC Adult CF Program in 2018–2019. Red + mark indicates a participant in this ACP survey showing the generally lower age and FEV1 of those who opted to participate. ACP, advance care planning; CF, cystic fibrosis; FEV1, forced expiratory volume in one second; UNC, University of North Carolina.
Demographics of Survey Respondents
FEV1, forced expiratory volume in one second.
Before the ACP meeting, respondents averaged a score of 45.1 (range 28–53), indicating generally good knowledge about ACP. After the ACP meeting, the average score rose to 49.6 (range 39–55), indicating a statistically significant improvement in the respondents' understanding of ACP topics (p = 0.003 by Wilcoxon Rank Sum test).
Analysis of responses to individual questions revealed more affirmative scores after the ACP meeting. “I have discussed with my loved ones my wishes at end of life” improved from 2.8 ± 1.0 to 3.6 ± 0.9, p = 0.001, and “I have documented or am in the process of documenting my wishes using an advanced directive or other form” improved from 2.8 ± 1.0 to 4.1 ± 1.1, p = 0.005 (Table 1). Overall, scores for most questions improved, suggesting greater knowledge and/or comfort level after having the ACP meeting, although most did not reach statistical significance.
Discussion
While professional organizations recommend early ACP in patients with chronic illnesses, there has been little published on actual implementation in a busy clinical setting. In this study, we report the feasibility of implementing multidisciplinary ACP with CF adults in the outpatient setting, and the positive effects these meetings can have for patients. Our survey showed that after completion of at least one ACP meeting with the outpatient care team, patients were more likely to have discussed their wishes for end of life with their families. This could result in improved written and verbal communication regarding patient preferences and goals of care, which could result in more goal-concordant care for people with CF.
In the interval since we began this work, a European team reported a robust QI project that involved designing a CF-specific ACP tool, resulting in improvement in documentation of end-of-life wishes from 10% at baseline to 85% after the intervention. 13 An enormous benefit of this funded study was the granting of no-cost access to training modules and the CF-ACP to health care professionals on the United Kingdom CF Trust website, encouraging providers to implement their own improvement programs.
Our local initiative shows the feasibility of conducting ACP encounters in a multidisciplinary CF clinic. One limitation of our study was the small sample size. Completing premeeting surveys was not a prerequisite for scheduling an ACP meeting, and only about half of the participants completed both surveys. In addition, surveys were not validated, as they were designed as a local process improvement tool. Finally, our project implementation timeline was halted due to coronavirus disease (COVID)-related changes in outpatient care. However, as we anticipate resuming ACP meetings, the hybrid virtual care model we have adopted might prove more convenient for working families.
Conclusions
In a multidisciplinary care model at a large academic CF center, we successfully implemented sustainable ACP meetings for adults with CF. We found increased comfort with ACP concepts and improved documentation of wishes after ACP meetings, and qualitative feedback from patients has been positive. It is important for health care providers to meet the needs of this patient population by ensuring that ACP is in place for patients before crisis situations.
Footnotes
Authors' Contributions
Conceptualization: E.A.S., M.L.B., B.W.J., S.H.D., and J.L.G.; data acquisition: E.A.S., M.L.B., B.W.J., and J.L.G.; data analysis/interpretation: S.H.T., E.A.S., M.L.B., B.W.J., E.P.D., S.H.D., and J.L.G.; drafting the work: S.H.T. and J.L.G.; and critical revisions: S.H.T., E.A.S., M.L.B., B.W.J., E.P.D., S.H.D., and J.L.G. All authors declare that they approve the final version of this article to be published, and accept accountability for all aspects of the work.
Acknowledgments
The authors would like to acknowledge the support of Katie Howe in collecting these data.
Funding Information
J.L.G. reports receiving funding from the Cystic Fibrosis Foundation in association with this work (GORALS19Y5).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.