
Abstract
Background:
Medical assistance in dying (MAiD) was legalized in Canada on June 17, 2016, yet many who request MAiD do not complete the assessment process and instead experience a natural death. This analysis of patients who made a formal request for MAiD aims to clarify timelines and factors associated with completion of the MAiD assessment process, and factors associated with completion or noncompletion of MAiD once eligible.
Materials and Methods:
This retrospective cohort study included all patients in Nova Scotia who requested MAiD between January 1, 2018 and December 31, 2018, were deceased at the time of analysis, did not withdraw their request, and were not formally deemed ineligible for the procedure (n = 218). Descriptive statistics, Kaplan–Meier curves, and logistic regression were used in data analysis.
Results:
Of 218 patients, 48 did not complete the MAiD assessment process. Of the 170 patients who completed the assessment process and were deemed eligible for MAiD, 79.4% (n = 135) completed the procedure. Those with an incomplete assessment had a median survival from request to death of 8.0 days (interquartile range [IQR] = 11.5), whereas for those deemed eligible, median survival from request to determination of MAiD eligibility was also 8.0 days (IQR = 16.0).
Interpretation:
Proximity to natural death and poor performance status at the time of MAiD request may drive incomplete MAiD assessments. The majority of patients deemed eligible for MAiD complete the procedure, and as such, patients who did not complete the MAiD assessment process may not have experienced their preferred mode of death.
Introduction
Since the passage of Bill C-14 in 2016 that legalized medical assistance in dying (MAiD), >14,000 Canadians have chosen to end their lives through medically supervised administration of lethal medication at the hands of a physician or nurse practitioner. As per the MAiD legislation before the passage of Bill C-7 on March 17, 2021, the law required that patients be suffering from a grievous and irremediable illness that causes persistent intolerable suffering and will result in a death that is reasonably foreseeable. Patients were required to submit a written request and undergo two independent assessments by a nurse practitioner or physician confirming they met eligibility criteria. Additional safeguards included the requirement of a 10-day reflection period after the request, and reconfirmation of consent at the time of the procedure. 1 Under Bill C-7, patients are now eligible to request MAiD if they suffer from a grievous and irremediable illness, but death is not required to be reasonably foreseeable. In addition, in cases where death is reasonably foreseeable, patients are no longer required to undergo the 10-day reflection period. 2
The percentage of the population dying by MAiD in Canada has increased gradually since 2016, with MAiD accounting for 2% of deaths in Canada in 2019. 3 Many others have made formal requests for MAiD, and have either not met the required legal standard, failed to complete the assessment process, or been approved and subsequently died a natural death after either losing capacity or withdrawing their request for other reasons. 3
The MAiD assessment process can be an arduous one for patients who are very ill and it is common for patients who request MAiD to lose capacity or die a natural death either before the assessment process is completed or after being approved for MAiD. 4
In our recent analysis of outcomes related to MAiD requests in the province of Nova Scotia, >25% of patients included did not complete the MAiD assessment process. 5 Possible underlying reasons for incomplete assessments include withdrawal of the request, loss of decision-making capacity, intervening natural death, or inability to complete the process owing to lack of access.
To date, although data indicate that the numbers of incomplete MAiD assessments are substantial,5,6 we lack a detailed understanding of the factors driving incomplete assessments and how factors such as diagnosis, lag-time between request and assessment, illness complexity, and access to palliative care are related to outcomes.
To better understand these factors, we undertook a secondary analysis of a subgroup from a study of all patients in Nova Scotia who made formal requests for MAiD in the first 2.5 years of legalization. 5 The intention of the analysis was to better understand the timeliness of MAiD assessments, completion of the procedure, and relevant variables associated with an incomplete MAiD assessment.
Materials and Methods
This retrospective cohort study is a secondary analysis from a study of all adult patients who made formal requests for MAiD between June 17, 2016 and December 31, 2018 in Nova Scotia, Canada, and were deceased at the time of analysis (n = 383). 5 The study cohort was identified through the Nova Scotia Health Authority MAiD Care Coordination Office, which maintains the provincial registry of MAiD requests. In this study, we included all those who requested MAiD in 2018 and were either deemed eligible for MAiD or in the process of being assessed for MAiD, at the time of their death. Patients were excluded if they were alive at the time of analysis (June 10, 2020), withdrew their request for MAiD, or were deemed ineligible for MAiD at any point. The institutional research ethics board approved this study. Informed consent was waived for this retrospective study.
Data were extracted from the electronic medical record, with individual health care providers contacted in the case of missing data. The variables collected included age at request, sex, primary care provider, residency in an urban versus rural area (defined by the forward sortation area portion of the postal code), 7 and residency in an area served by a tertiary care center, Charlson comorbidity index (CCI) at the time of request, 8 receipt and date of specialist Palliative Care consultation, underlying condition driving MAiD request, date of MAiD request, date of MAiD assessments, date of death, and mode of death (natural death versus medically assisted).
Specialist palliative care in Nova Scotia is administered provincially through the Nova Scotia Health Authority. Payment sources include a mixture of fee for service, alternative funding plans, and academic funding plans. Team staffing includes 19.9 physician full-time equivalent (FTE), 9.6 social work FTE, and 51.2 community-based nursing FTE. Care is provided in the community, inpatient settings, nursing homes, and in ambulatory care settings. Dedicated staff availability varies through the province, but in general, 24/7 support is available through community nursing and Emergency Health Services with additional training in Palliative Care. Referrals are generated through a variety of physician specialists, including Family Medicine and Medical Oncology. The average number of patients enrolled in the program annually ranges from 3000 to 5000.
The study population was categorized according to MAiD assessment outcome. Patients who were assessed and deemed eligible for MAiD, regardless of mode of death, were assigned to the “MAiD Eligible” cohort. Those who died or lost capacity before the completion of the MAiD assessment process were assigned to the “Incomplete Assessment” cohort. Within the “MAiD Eligible” cohort, patients were further categorized by mode of death (“MAiD Eligible: Natural death” subcohort vs. “MAiD Eligible: MAiD Death” subcohort).
Descriptive statistics were used to describe the population. The distribution of continuous variables was tested with the Shapiro–Wilk test, with normally distributed variables reported as means and standard deviations, and non-normally distributed variables reported as medians and interquartile ranges (IQR). Categorical variables were reported as percentages. Differences between cohorts were analyzed with chi-square tests for categorical variables, analysis of variance for continuous variables with normal distribution, and Wilcoxon rank sum test for continuous variables with non-normal distribution (including survival time). Statistical significance was determined at alpha ≤0.05. Kaplan–Meier curves were created to compare differences in survival from the time of MAiD request to death. The dataset was complete, with the exception of a single missing date of death, which was noted in the data table and simply excluded from analysis.
Simple logistic regression was used to identify variables associated with a complete MAiD assessment. Multivariable logistic regression was subsequently conducted with specialist palliative care consultation as the main exposure of interest, with the model adjusted for other potentially significant variables (as defined by a p-value of ≤0.15 on single variable logistic regression).
Statistical analyses were performed using the statistical packages of R and R Studio. 9 This study was approved by the Research Ethics Board at the Nova Scotia Health Authority (Protocol No. 1023925).
Results
Between January 1, 2018 and December 31, 2018, a total of 239 patients requested MAiD in Nova Scotia (Fig. 1). Of those, 11 were excluded from analysis as they were alive at the time of data analysis, 4 were excluded as they were deemed ineligible on assessment, and 6 were excluded as they withdrew their request for MAiD. Of the remaining 218 patients, 48 patients had incomplete assessments before death, whereas 170 patients completed the assessment process and were deemed eligible for MAiD. Of those 170 patients eligible for MAiD, 79.4% (n = 135) completed the procedure.

Study cohort selection and outcomes.
The study groups differed significantly in terms of consultation with specialist Palliative Care and survival from time of MAiD request to death (Table 1). Compared with those with a complete MAiD assessment, a greater proportion of those with incomplete assessments were seen by specialist Palliative Care at any time (85.4% vs. 67.6%, p = 0.026). However, there was no significant difference between groups in the proportion of those receiving a specialist Palliative Care consultation before MAiD request (68.8% vs. 54.7%, p = 1.00). Those with an incomplete MAiD assessment had a median survival from MAiD request to death of 8.0 days (IQR = 11.5), compared with 23.5 days (IQR = 50.8) in those with a complete MAiD assessment (p < 0.001) (Fig. 2).
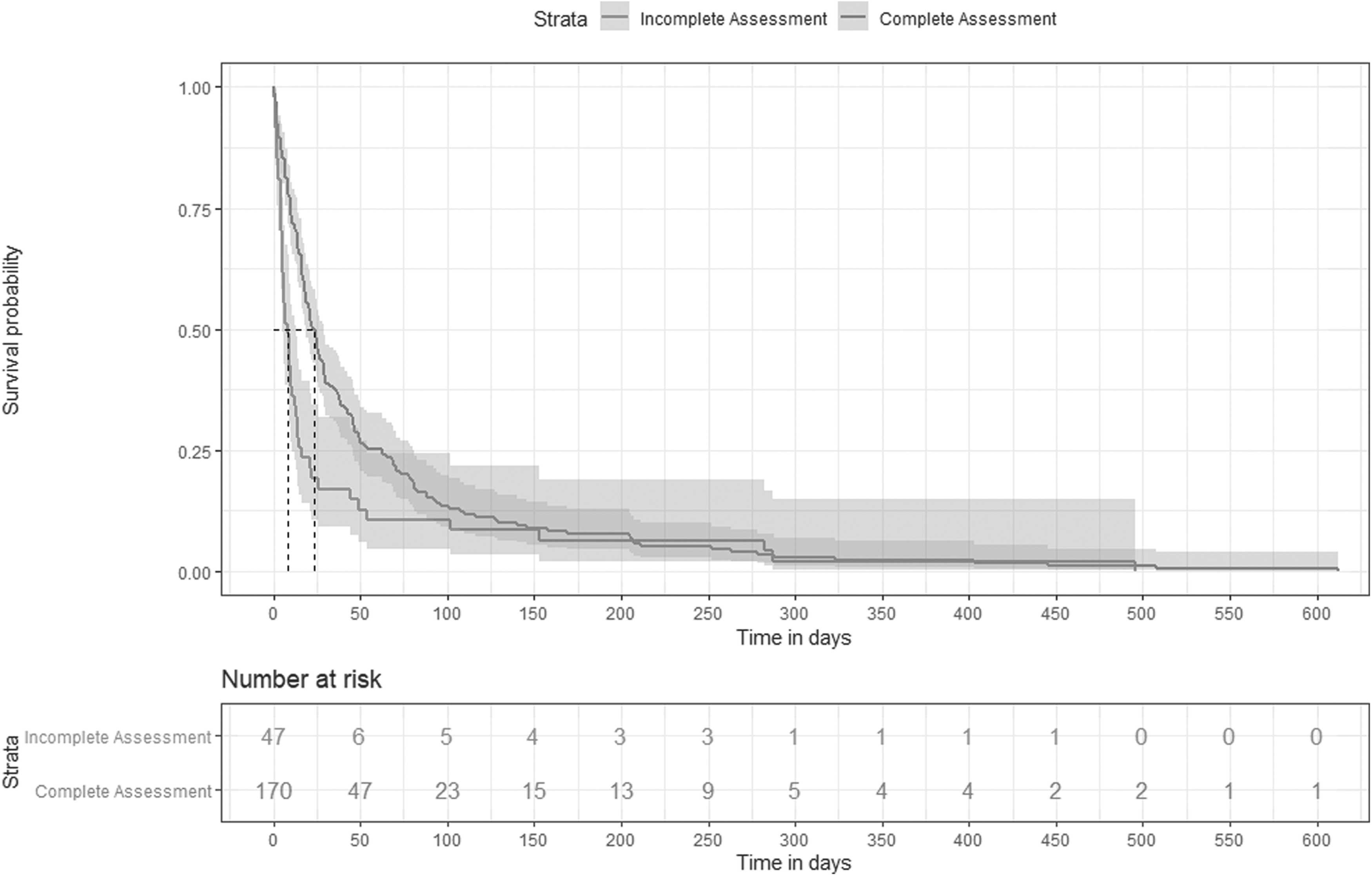
Overall survival from time of MAiD request by status of MAiD assessment. MAiD, medical assistance in dying.
Characteristics of Patients by Medical Assistance in Dying Assessment Status
Non-normal distribution as determined by the Shapiro–Wilk test, medians and IQR reported, Wilcoxon rank sum test used for determination of significance.
CCI, Charlson comorbidity index; CI, confidence interval; IQR, interquartile range; MAiD, medical assistance in dying.
By univariable analysis (Table 2), we found that receipt of a specialist Palliative Care consult at any point in time was associated with decreased odds of a complete assessment (odds ratio [OR] = 0.35, confidence interval [95% CI] = 0.14–0.80, p = 0.019). Specialist Palliative Care consultation before MAiD request was not significant. In multivariable analysis adjusted for specialist Palliative Care consultation and CCI (identified as potentially significant on univariable analysis, OR = 0.52, 95% CI = 0.27–1.01, p = 0.053), specialist Palliative Care consultation at any point in time remained associated with decreased odds of complete assessment (OR = 0.38, 95% CI = 0.15–0.86, p = 0.028).
Logistic Regression: Predictors of Complete Assessment
OR, odds ratio.
Of those with a complete assessment and eligible for MAiD (n = 170), the majority completed the procedure (79.4%, n = 135). There were no significant differences between those who completed the procedure and those who experienced a natural death in terms of age, sex, access to a primary care provider, underlying condition, area of residency, CCI, or specialist Palliative Care involvement (Table 3). Median time from request to being deemed eligible for MAiD was 8 days (IQR = 16.0) in both groups (p = 0.531). However, the median survival from the time of eligibility for those completing the MAiD procedure was 6 days (IQR = 16.0), compared with 27 days (IQR = 78.5) for those who experienced a natural death (p = 0.001) (Fig. 3).

Overall survival from time of MAiD request by mode of death (MAiD eligible patients).
Characteristics of Patients Eligible for Medical Assistance in Dying by Mode of Death
Non-normal distribution as determined by the Shapiro–Wilk test, medians and IQR reported, Wilcoxon-rank sum test used for determination of significance.
Discussion
The majority of those deemed eligible for MAiD completed the procedure. At a completion rate of 79.4%, a greater proportion of patients in Nova Scotia who request MAiD completed the procedure compared with similar 2018 data from Alberta (61.9%), Saskatchewan (39.0%), and Manitoba (58.6%). 3 This is potentially owing the organization of MAiD delivery in Nova Scotia, which has one Health Authority overseeing a population of under 1 million people located within a manageable geographic area for access to MAiD services. In addition, there is a centralized MAiD Coordination office with a dedicated Nurse Navigator who answers questions and guides MAiD assessors, providers, and patients through the process. The Nurse Navigator keeps an active log of patients who have made a request for MAiD, which is organized and triaged based on the urgency of the cases. In the case of patients who are deteriorating rapidly, it is possible for assessments and procedures to be expedited if necessary.
The median time from request to being deemed MAiD eligible was 8 days, whereas the median survival of those with incomplete MAiD assessment was also 8 days. It is noteworthy that the median survival of those with an incomplete MAiD assessment is shorter than the 10-day reflection period required by law following a formal written request for MAiD. More than one-third patients receiving MAiD in Canada have had the requirement for the 10-day reflection period waived because of imminent risk of losing capacity or dying, although we unfortunately did not have these data for our own study cohort. 3 When looking at survival among those in our cohort who completed the assessment process and were found to be MAiD eligible, the difference in median life expectancy between those who had a MAiD death and those who had a natural death was 21 days (6.0 days, IQR = 16.0 days vs. 27.0 days, IQR = 78.5). It is possible that for many with life-limiting illness, intolerable suffering leading to requests for MAiD is most prevalent in the very late stages of disease and that natural death or incapacity frequently ensues before MAiD could be provided under the stipulations of the previous MAiD legislation.
Family caregivers have highlighted issues with quality and access when it comes to provision of MAiD in Canada. 10 The short survival time of those with incomplete assessments and the significant numbers of MAiD completers who have the 10-day reflection period waived underscores a pressing need for MAiD quality indicators that incorporate standard triage criteria, dashboards and benchmarks for wait times, taking into account projected survival beyond the broad qualifier of a reasonably foreseeable death. Although the 10-day reflection period required of our study population has since been removed under Bill C-7 as of March 17, 2021, loss of capacity or natural death while waiting for assessments or for the procedure itself will remain a concern and should receive ongoing attention. 2 One study of MAiD requests at a tertiary care center in Ontario found that patients with a Palliative Performance Scale Score 11 of 40% or less was associated with loss of capacity or a shortened reflection period. 1 Along with indicators for hospice and palliative care, indicators for MAiD should be incorporated into broad frameworks for quality end-of-life care.
We previously reported that specialist Palliative Care consultation was associated with decreased odds of MAiD completion in this cohort. 5 In this study, specialist Palliative Care involvement before MAiD request had no impact on the odds of complete assessment, whereas specialist Palliative Care consultation at any time was associated with decreased odds of a complete MAiD assessment. We hypothesize that specialist Palliative Care consultation, particularly following a request for MAiD, is a surrogate marker of severe disease and decline precluding further assessment owing to imminent loss of capacity and proximity to natural death. It is possible that under the expanded criteria of Bill C-7, more patients will complete MAiD following a request. 2 As patients who withdrew their request for MAiD were excluded from analysis, this association likely does not represent an effect of Palliative Care on the desire for MAiD in this population, although we do not have data on patient-driven delay of the MAiD assessment process, as opposed to clear withdrawal.
Strengths and Limitations
Our study is provincial in scope, with only a single data point missing. To our knowledge, this is also the first study of its kind looking at timely access to MAiD in Canada.
Our study is limited by our inability to determine any intervening factors in access to MAiD, such as performance status at the time of request and patient-driven delays. Furthermore, prospective research with careful documentation of performance status at the time of request and notation of the reason underlying any interruption to the MAiD assessment process would provide stronger evidence of underlying associations between geographic, demographic, or systems factors and access to MAiD. In addition, the nature of the eligibility criteria for MAiD is such that there is no way to retrospectively determine whether someone would have been eligible had they survived the assessment process, as some facets of eligibility would not necessarily be documented as such in the medical record. If a substantial number of patients in the Incomplete Assessment cohort would have been deemed ineligible, this could certainly have biased results, although the small proportion of ineligible patients overall (just 4 of 239 requests in this study were found ineligible) make this unlikely.
Conclusion
In this provincial study of MAiD requests in 2018, we found that the majority of patients who request MAiD and are deemed eligible complete the procedure. Of those who died before MAiD eligibility could be determined, the median survival time after request was 8 days, which was also the median time from request to determination of MAiD eligibility in those who complete the process. We hypothesize that poor prognosis and decreased performance status at the time of the MAiD request may result in incomplete MAiD assessments.
Quality indicators for end-of-life care in the MAiD-seeking population would be helpful to provide guidance around appropriate, timely access to care, and further to determine the optimal time at which patients who desire MAiD should make their request to ensure they survive long enough to complete the assessment process. It is reasonable to assume that given the large proportion of eligible patients who opt to undergo death by MAiD, a number of those who do not complete the assessment process may not have experienced the mode of death of their choice.
Footnotes
Funding Information
Funding for this project was generously provided by the Nova Scotia Health Authority Research Fund. This funding agency had no role in data collection, its analysis or interpretation, and have no rights in the approval or disapproval of publication.
Author Disclosure Statement
C.L.: Current member of Canadian Society of Palliative Care Physicians; Current member of Canadian Association of MAiD Assessors and Providers. G.G.: MAiD Assessor and Provider in Nova Scotia; Clinical Lead for the Nova Scotia MAiD Network. R.H.: Current member of Canadian Society of Palliative Care Physicians; Current member of Canadian Association of MAiD Assessors and Providers; Former Member of the Physician Advisory Council Dying with Dignity Canada, Former Board Director Hospice Halifax.