
Abstract
Background:
Transmucosal fentanyl (TF), used for breakthrough cancer pain (BTcP) treatment, has different formulations with distinctive attributes. The hypothesis is that, in shared decision making for the prevention of certain therapeutic problems, doctors and patients assign different value to the characteristics of treatment options.
Aim:
The aim of this study was to assess the discordance between the oncologists' opinion of attributes of TF and patients' expectations in BTcP treatment.
Methods:
This is a multicenter, cross-sectional observational study using simultaneous written surveys of doctors and patients suffering from BTcP episodes. The opinion of Spanish oncologists and patients regarding the importance of 14 different attributes of TF treatment (start of action, potency, duration, presentations and doses available, ease of use, titration, administration time, need for saliva, oral mucositis, rhinitis, adverse events, risk of abuse, evidence available, and need for instructions or health personnel to handle the medication), using two surveys, one for each group.
Results:
Sixty-three clinical oncologists and 272 patients participated in the study. The patients' satisfaction with and knowledge of BTcP treatment was 6.4 and 6.8 points, respectively (scale 1–9). The attributes with the highest relevance were shared by both groups, although their priority differed. Significant differences were observed in the greater importance given by oncologists (onset and duration of analgesia, need for saliva, presence of mucositis, and time required for patient education) and patients (risk of opioid abuse/aberrant behavior).
Conclusion:
Our results confirm that some aspects that most concern patients about the treatment of BTcP differ from those to which oncologists attach most importance. Increased patient awareness and education about BTcP and its treatment could lead to greater satisfaction and better patient involvement in therapeutic decisions. Certain barriers need to be overcome, such as lack of time in consultations and poor communication skills of oncologists that hinder patient health education.
Introduction
The shared decision-making (SDM) approach, which allows patients to engage in clinical and therapeutic decision making, has had a favorable impact on clinical results and patient satisfaction.1–4 This approach involves communicating clear and accurate information that builds patient understanding, while also meeting their needs and expectations.5–8 Treatment adherence and patient satisfaction are shown to be higher when patient preferences are taken into account, including for pain. 9 This is particularly important when dealing with health problems, such as cancer pain, which have a significant impact on the patient's quality of life. 10
For cancer patients, pain is one of the most feared and distressing symptoms 11 and can have a devastating effect on a patient's health and general wellbeing. For many of these patients, adequate pain control is just as important as the efficacy and the safety of the cancer treatment, namely its antitumoral effect and prevention of underlying complications. 12
Episodes of breakthrough cancer pain (BTcP), 13 a common phenomenon among cancer patients, are difficult to manage11,14,15 and tend to be poorly or inappropriately treated. 11 This often leads to significant psychological strain and functional deterioration in patients, as well as high levels of anxiety among their caregivers.15–17
The treatment of BTcP changed radically with the introduction of transmucosal fentanyl (TF), a potent, fast-acting opioid analgesic with acceptable tolerance.13,18,19 There are different oral TF galenic formulations available 11 (oral, sublingual, and intranasal), prescribed according to doctors' judgment18,20 and their personal experience. The Adapta study (2017) collected the opinions of an expert panel of Spanish oncologists on the different attributes of these formulations based on their clinical experience. 21 The features most highly valued by the experts were rapid onset, ease of use, and duration. Although the panel considered all TF formulations to be safe and well tolerated, possible differential advantages among them were suggested when choosing treatments. 21
The Adapta study was based exclusively on the opinions of TF prescribing physicians. This study adds the assessment of cancer patients on the same question. Patients' expectations about these treatments depend on the information available to them about BTcP treatment options and on their personal experience of illness. Describing possible discordances between physicians' and patients' opinions on the different attributes of TF can help to identify problems that can be rectified in patients (lack of knowledge, misunderstandings, unfounded fears, unrealistic expectations,…). In addition, it can help oncologists to better understand and consider the specific preferences of each patient when personalizing TF treatment, improving its acceptability and adherence. 9
Methods
Study design
This was a multicenter, cross-sectional observational study carried out using written surveys to collect the opinions of oncologists and patients regarding different attributes of the rescue analgesic medications used for BTcP.
Participants
Oncologists from all over Spain were invited to participate in the study, including public and private hospitals and outpatient centers, with a stratified distribution of professionals according to the population size of each Autonomous Community. The eligibility criteria for the participation of oncology patients were as follows: adults (≥18 years of age), receiving treatment from a doctor/researcher participating in the study, with a history of BTcP episodes occurring at least one month before the start of the study, and with no restrictions in prescribed treatments or other concomitant treatments before the study.
To detect significant differences in the proportion of doctors and patients assigning “high importance” to the different aspects and main variables of the survey (after a binomial categorization of the evaluation scales, described below), a total of 105 oncologists and 525 patients were consulted.
To recruit these patients, each participating doctor was requested to recruit the first five eligible patients who agreed to take part in the study from the beginning (May 2018). The fieldwork was completed between May and June 2018.
Study variables and data collection
Two self-administered surveys were used: one for patients and another for oncologists.
The content of the survey comes from the proposal of differential attributes of available analgesic treatments for BTcP episodes presented in an expert consensus published in our same setting previously (Adapta study, 21 DOI: 10.20986/resed.2018.3661/2018). In that study, 14 characteristics of such treatments were identified and prioritized for their importance in making therapeutic decisions about individual patients. The practitioner version of the survey transcribed verbatim the wording of findings from the previous study (Table 1). The version for patients included the same items with identical content, after adapting the language to avoid technical jargon and ensure its comprehension by all types of people.
Discrepancies in the Proportion of Doctors and Patients Who Award High Importance (Score 7–9) to the Different Attributes of the Treatment Evaluated (in Each Item, the Definition Used for Each Group Is Detailed)
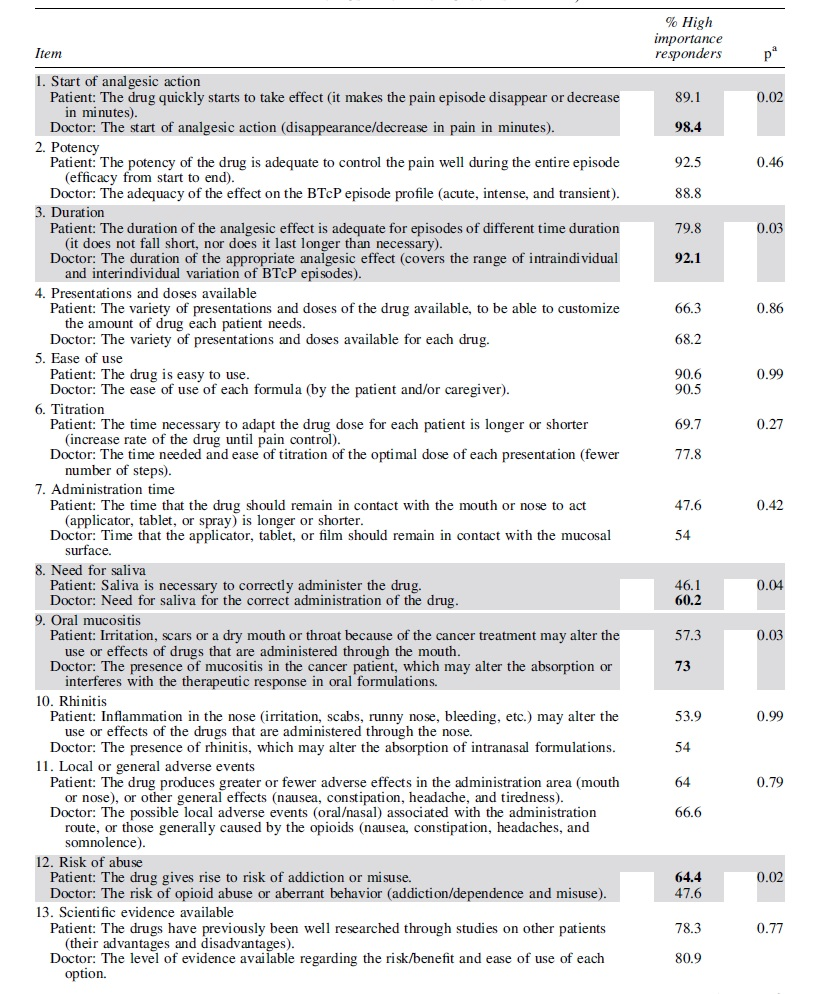

To confirm the stability of the content, three editors adapted the text, compared their versions, and agreed on a single draft. The semantic reversibility of the final text was confirmed by exploring the coincident understanding of physicians and patients in a mixed focus group (10 subjects) arranged ad hoc. Table 1 compares the definitions of the 14 survey items in both versions.
Each item presents an attribute of TF treatment proposed by expert oncologists in the cited study 21 (Table 1). Our survey was constructed by adding to each item a 9-point Likert-type ordinal scale to assess the relative “importance” of each item (by its weight in therapeutic decision making), according to a widely used format for its application in consensus processes 22 (Fig. 1).
Likert-type 9-point scale used to collect patients' and prescribers' opinions of the different attributes of BTcP treatments included in the survey. BTcP, breakthrough cancer pain.
The oncologists first completed an online survey to ascertain their opinions on the subject of the study using an access-restricted website. Patients were then recruited during their routine clinical follow-up visits. Patients' opinions were collected using an anonymous, written survey completed by the patients or, where necessary, by their main caregiver, to minimize their doctor's influence or bias on the patient's answers. Each oncologist collected the responses from their five patients and the data were aggregated on the website.
For descriptive purposes, the professional characteristics of the oncologists were recorded (age, gender, health care environment, professional experience, experience with BTcP, and the use of rescue therapy), as well as the demographic and clinical profile of the patients (age, gender, experience with BTcP rescue therapy, and any other information the patient has regarding these treatments).
Statistical analysis
Quantitative variables were described with conventional pooling and dispersion measures (mean and range). Each group ranked different attributes of the evaluated drugs, and the arithmetic mean of the total scores in each survey group was calculated to rank the level of priority/importance.
To detect possible differences in criteria (overvaluation or undervaluation between oncologists and patients), the ordinal scores were categorized dichotomously, creating the new variable “High importance/priority” (score 1–6 = n and score 7–9 = yes) to compare the percentage of subjects of each group that ranked each attribute as “high importance.” The proportionate differences were calculated using the chi-square test (p < 0.05 is considered significant). Version 13.0 of the SPSS-W integrated package was used for statistical analysis of the results, presented below.
The study was performed in accordance with the ethical requirements of the Declaration of Helsinki (October 2013) for research on human subjects and was approved by the independent Ethics Committee for Research with Medicinal Products (Princesa University Hospital, Madrid) on April 26, 2018 (Acta 07/18).
The personal data of participants were collected in aggregate form (anonymized data) after their verbal informed consent was obtained by the oncologists.
Results
Sixty-three oncologists participated in the study (response rate: 60%), of whom 44% were female, with a mean age of 42 years (range: 30–75). Most of the oncologists (96.8%) worked in the public health system in hospitals. The mean professional experience was 12 years (range: 2–28 years). On average, oncologists reported seeing 20 cancer patients per day, of whom about 25% had episodes of BTcP.
Oncologists recruited 272 patients with BTcP episodes (52% response rate), 57% of whom were male. The age of patients ranged between 18 and 87 years (25% between 55 and 64 years and 38% between 65 and 74 years), with 48% of the patients older than 64 years.
Analgesic treatment (TF preparations) for BTcP episodes was used by 89% of the patients (for one to four months) and had been used previously by the remaining patients. The level of satisfaction with the BTcP treatment (mean) reported by the patients was 6.8 points and the self-perceived level of knowledge regarding the issues (advantages, risks, use, precautions, alternatives, etc.) was 6.4 points (scores from 1 to 9).
Figure 2A and B show, in order of priority, the importance that oncologists and patients give to different attributes of the treatment, based on the average score of each attribute (scale of priority: 1 to 9 points).

Importance of the attributes of BTcP treatment, based on the mean score (low = 1–3, medium = 4–6, and high = 7–9) given by oncologists
The attributes with the highest importance (scores of 7 to 9) were the same for oncologists and patients (Fig. 2A, B), although the order of importance differed between the groups. The differences in perception of the attributes of BTcP treatment among patients and oncologists are compared in detail in Table 1.
Compared with patients, oncologists gave a statistically significant higher relevance to the following items: “onset of analgesic action,” “duration of the analgesic effect,” “need for saliva for the correct administration of the drug,” “presence of mucositis in the cancer patient, which alters the absorption or interferes in the treatment response in oral formulations,” and “time necessary for healthcare staff to explain the correct administration of each pharmaceutical form.” On the other hand, patients gave a statistically significant higher relevance of the item regarding “risk of opioid abuse or aberrant behavior (addiction/dependence and misuse).”
For the remaining issues, there were no significant differences in criteria between the groups.
Discussion
Main findings/results of the study
Although several previous studies reported high levels of patient satisfaction with some TF preparations,23,24 our results detect room for improvement in this matter (6.8 on a scale of 1 to 9). The results provided below may further explain this point.
Patients' self-perceived level of knowledge regarding BTcP treatment is limited (6.4 on a scale of 1 to 9) and seems congruent with some of the barriers recently identified by a Spanish expert group for BTcP management,25,26 namely the lack of appropriate written information for patients and limited time in clinical practice to educate patients.
The participating oncologists see an average of 20 cancer patients a day, pointing to the time limitations previously reported by Spanish oncologists.25,26 The time pressure in consultations may explain why oncologists were more concerned than patients about the time needed to explain the correct administration of each pharmaceutical form. This time limitation may make it difficult to ensure that patients are appropriately informed and have understood all the information and instructions for the analgesic therapy. It may also limit the performance of routine, systematic pain evaluations.26,27
Furthermore, oncologists may not have the adequate communication skills to elicit patients' concerns and preferences regarding the BTcP treatment. 26 Improving these skills and improving written and verbal information may be an effective strategy to overcome these barriers. 26 Our study seems to confirm these findings, suggesting the need to raise oncologists' awareness about the relevance of explaining the correct handling of each analgesic drug effectively and in detail. The supportive role of specialized nurses 28 should be considered part of the multidisciplinary approach required for BTcP management. 11
The main characteristics of the drug (onset, duration, and analgesic potency) were very important for both groups. However, oncologists valued kinetic attributes (speed and duration of action) more than patients, while patients were more concerned about the adequate potency effect for the intensity of pain. These differences can be attributed to the fact that many patients essentially link the disabling nature of the BTcP episode to its very high intensity (7 on a visual analog scale [VAS] of 0–10 in 77% of BTcP patients needing medication 29 ). Patients' expectations should be suitably addressed by doctors, who should ensure that patients receive the most suitable pharmacological dose for partial or complete remission of BTcP episodes. 18
The temporal pattern of BTcP episodes requires fast analgesia. 11 This explains why “onset of analgesic action” was the most relevant attribute among oncologists (8.2/9 points; of “high importance” for 98.4% of the professionals), and the second most relevant attribute among patients (8/9 points; “high importance” for 89.1% of them). Onset of analgesic action was also highly important in the Adapta study 21 (for 84% of participating professionals) and in an exploratory Delphi study performed in Spain 30 (for 97.8% of oncologists surveyed; 6.5 on a scale of 1 to 7).
Patients expressed greater concern for the risk of abuse or dependence in comparison with doctors (64.4% vs. 47.6% considered it to be a problem of “high importance”). This may reflect the oncologists' knowledge of ways to reduce the risk of patients developing dependence 31 and a lack of patient awareness of this matter. On the other hand, it may also suggest that oncologists prioritized aspects associated with efficacy and ease of use, which offer a better quality of life for patients with a short life expectancy (inferior to three to six months in some cases). These differences suggest that oncologists should make a greater effort to understand the expectations of patients and evaluate their concerns, including their concerns about drug dependence, in the new patient-centric clinical approach.
Oncologists give greater importance to the need for saliva and/or the presence of mucositis, which may alter the absorption of the drug32,33 and act as a crucial factor when choosing among drugs with different administration routes. These are strictly technical concerns for the doctor, mainly with sublingual or nasal administration, for preventing analgesic inefficiency due to disruption from the mucosal barrier. Without specific knowledge, this factor can be less relevant to the patient, who believes that all medication will be effective regardless of its administration route. Once again, this suggests the need for patient education, 11 spending more time making patients aware of this issue, and making these issues easier to understand.
Strengths and weaknesses/limitations of the study
This multicenter study establishes the opinions of a wide group of geographically stratified Spanish cancer patients treated at some time with TF as a rescue analgesic for BTcP. Physicians were instructed to consecutively recruit the first eligible patients in their appointment schedule from a random date assigned by the study leaders, to minimize possible selection bias. Patients who agreed to participate were invited to express their opinions about the drugs according to their personal experience with their BTcP, before (at baseline) their own medical consultation and by means of an anonymous written survey. They were informed that at no time during the study would the physicians be able to know their opinions or identify the responses of any particular patient. This was intended to reduce the risk of feeling influenced by their physicians in assessing their treatments.
One limitation of our study is that the forecast sample size for both oncologists and patients was not achieved. The sample size achieved (63 of the 105 oncologists invited to participate) proportionally reduced the number of patients recruited with respect to the initial pretensions (272 of 525). However, a significant number of oncologists and patients did participate and this does not invalidate the overall results: the samples collected allow us to detect differences in proportion equal to or greater than 10% (80% vs. 90%) in the number of physicians and patients who hold a similar opinion, all this for a confidence level of 95% and a study power of 80%. For all these reasons, we consider that the sample collected is sufficient.
A larger sample may have provided the conventionally required level of significance (p > 0.05) in other differences observed regarding other characteristics of fentanyl.
What this study adds
The results of our study suggest that expectations of and preferences for BTcP treatment differ between oncologists and patients. These differences may reveal the need to enhance cancer patients' knowledge and understanding of their illness and pain therapy. This could better enable patients to engage in clinical and therapeutic decision making with its demonstrated benefits. Moreover, additional barriers in BTcP management were revealed, such as time limitations in oncologists' consultations and insufficient communication skills. As regard of time-pressured situation, the focus topic in both oncologists and patients is anticancer treatment, which may affect the content of their discussions and how much time they spend on it.
Taking these findings into account would allow for a more effective SDM process and could contribute to improving treatment adherence and efficacy in controlling BTcP in cancer patients. 14
Footnotes
Acknowledgments
We thank the participating oncologists and patients for their collaboration in answering the study questionnaire. We thank the Francisco de Vitoria University for the technical coordination work of this study. We thank Kyowa Kirin Farmacéutica S.L. for funding the study.
Funding Information
The study has been funded by Kyowa Kirin Farmacéutica S.L.U.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.