
Abstract
Background/Objective:
Evidence linking process-based, high-quality end-of-life (EOL) care indicators to family satisfaction with EOL care in intensive care units (ICUs) remains limited. This study aimed to fill this gap.
Design/Setting/Subjects/Measures/Statistical Analysis:
For this exploratory, prospective, longitudinal observational study, 278 family members were consecutively recruited from medical ICUs at two medical centers in Taiwan. Family satisfaction with ICU care was surveyed in the first month after patient death using the Family Satisfaction in the ICU questionnaire (FS-ICU). Associations between FS-ICU scores and process-based quality indicators collected over the patient's ICU stay were examined using generalized estimating equations.
Results:
Documentation of process-based indicators of high-quality EOL care was generally associated with higher scores for both the FS-ICU Care and FS-ICU Decision-Making domains. Higher family satisfaction with ICU care was significantly associated with physician–family prognostic communication (β [95% confidence interval (CI)]: 3.558 [2.963 to 4.154]), a do-not-resuscitate (DNR) order in place at death (23.095 [17.410 to 28.779]), and death without cardiopulmonary resuscitation (CPR) (13.325 [11.685 to 14.965]). Family members' satisfaction with decision making was positively associated with documentation of social worker involvement (4.767 [0.663 to 8.872]), a DNR order issued (10.499 [0.223 to 20.776]), and withdrawal of life-sustaining treatments (LSTs) before death (2.252 [1.834 to 2.670]).
Conclusions
: EOL care processes are associated with family satisfaction with EOL care in ICUs. Bereaved family members' satisfaction with EOL care in ICUs may be improved by promoting physician–family prognostic communication and psychosocial support, facilitating a DNR order and death without CPR, and withdrawing LSTs for patients dying in ICUs.
Introduction
Intensive care has grown substantially worldwide over recent decades,1–3 and death in intensive care units (ICUs) is common. 4 However, landmark studies highlighted the improving, but unsatisfactory, quality of end-of-life (EOL) care in ICUs.5–10 Thus, improving EOL care quality in ICUs is recognized worldwide as a priority for improving ICU quality to promote patients' and family members' values and preferences and to improve the quality of death and dying.11,12
To understand how well EOL care is provided in ICUs, thereby triggering quality improvements, measurements of EOL care quality delivery are needed from multiple domains and perspectives.8,13 The essential domains and indicators of high-quality EOL care in the ICU using medical record information have been proposed, defined, and validated since 200311,13 and examined for patients dying in ICUs worldwide5,8,9,13–16 while focusing on communication with and psychosocial support for families to facilitate informed EOL care decision making and limit potentially inappropriate life-sustaining treatments (LSTs) at the end of life.
However, quality of EOL care in ICUs measured only by chart-derived process-based indicators may not reflect how care is perceived by patients and families 17 and whether observed EOL events are linked with outcomes they consider important to reflect the core elements of high-quality EOL care, that is, goal-concordant care and patient- and family-centeredness.13,18,19
Family satisfaction with EOL care in ICUs reflects how well health care professionals can meet the needs and expectations of family members of critically ill dying patients, 20 thereby constituting an important outcome for evaluating EOL care quality in ICUs. Family members' poor experience of their beloved's death and dying or dissatisfaction with EOL care in ICUs has been associated with a greater risk of suffering from anxiety,15,21 depression,15,22 post-traumatic stress disorder,15,23 and complicated grief15,24 over the first bereavement year.
High family satisfaction with ICU care is associated with actionable high-quality EOL care in ICUs, for example, timely physician communication with the family, 8 offering psychosocial support, 8 discussing EOL care wishes during a family conference,25,26 withdrawing LSTs,25,27,28 no cardiopulmonary resuscitation (CPR) before death, 27 no use of LSTs (e.g., vasopressors), 15 no do-not-resuscitate (DNR) order issued, 29 and family presence at death. 27 However, evidence linking EOL care processes to bereaved family members' satisfaction with their beloved's EOL care in ICUs remains limited with only seven studies.8,15,25–29
Among these seven studies, sample sizes tended to be small, that is, 116–200,8,15,29 except for four studies25–28 derived from a multicenter study (N = 275–584). However, these four studies using data from over a decade ago may not reflect current EOL care practices in ICUs, especially with the emphasis on integrating palliative care into ICUs. 30 Among the three more recent studies,8,15,29 not all patients died in ICUs.8,29 Furthermore, associations of family satisfaction with EOL care were examined inconsistently with process-based indicators of high-quality EOL care in ICUs. Indeed, most of these studies examined only one indicator as shown above. Last, associations were commonly examined by univariate analysis8,15,25,29 without adjusting for patient and family characteristics to avoid false associations. 31
Therefore, we aimed to comprehensively examine associations between family satisfaction with EOL care in ICUs and chart-derived, process-based quality indicators of EOL care among a large cohort of ICU patients while adjusting for patient and family characteristics and length of ICU stay.
Materials and Methods
Study design and settings
This study was part of a prospective, longitudinal observational study focused on quality of EOL care in ICUs.16,22 Quality assessments of EOL care in ICUs by medical record review 16 and associations of EOL care quality in ICUs with bereaved family members' psychological distress 22 have been reported. In this study, we assessed the associations between family satisfaction with EOL care and the quality of EOL care for ICU patients by medical record review.
Patients and their family member were recruited from January 2018 to December 2019, and followed through January 2020, from two academically affiliated level III medical ICUs in Taiwan. Intensivists took charge of the patient's ICU care, the nurse-to-patient ratio was maximally 1:2 per shift, and an open visiting policy was implemented in the study ICUs. Palliative care by specialist consultations, a DNR order, and formally reimbursed family meetings were not mandated, but were promoted by the Taiwanese government for dying patients. Bedside physician–family prognostic and EOL care discussions were commonly conducted. The central Institutional Review Board of the study sites approved this study (201700343B0).
Sampling strategy and study participants
To be eligible for participation, ICU patients had to have an Acute Physiology and Chronic Health Evaluation (APACHE) II score >20 at enrollment to indicate they were at high risk for dying. Patients were excluded if they died within 3 days of ICU admission to allow sufficient time to implement high-quality EOL care.9,32 To be eligible for participation, adult family members had to meet the following criteria: (1) self-identified as having legal authority to act as a surrogate for their beloved's medical decisions and most involved in the ICU care experience and (2) competent to communicate with data collectors. Each patient's legal family surrogate signed an informed consent for reviewing the patient's medical record and their own participation.
Measures
Outcome variable
Family satisfaction with EOL care in ICUs was evaluated by the Family Satisfaction in the ICU questionnaire (FS-ICU),33,34 the most widely validated instrument for assessing family satisfaction with ICU care. 35 FS-ICU measures satisfaction in two domains: satisfaction with care (FS-ICU Care; 14 items) and satisfaction with decision making (FS-ICU Decision-Making; 10 items). The FS-ICU Care subscale assesses the level of satisfaction with how the patient and family member were treated in the ICU, including information access; care quality, coordination, continuity, and accessibility; and the ICU and waiting room atmosphere. The FS-ICU Decision-Making subscale measures the extent to which families are satisfied with the content, completeness, and consistency of information they received and the amount and quality of involvement and support during decision-making processes.
To score the FS-ICU, we followed the methods recommended by the developers of the FS-ICU.33,34 Item responses from participants were rescaled from the original 1–5 Likert scale to a scale from 0 (least satisfied) to 100 (most satisfied) by subtracting 1 from the scores and then multiplying each score by 25. No participant provided data for <70% of the items. Six items had a “not applicable” response (2.17%–56.32%), and two items (agitation management, 31.29%) and (waiting room atmosphere, 56.32%) were rated as “not applicable” by >10% of family participants. Therefore, these two items were removed to calculate the FS-ICU Care score.33,34 Internal consistency was high (Cronbach's alpha: FS-ICU Care 0.974; FS-ICU Decision-Making 0.974) and correlation between the two domains was 0.752 in this study.
Primary independent variables
Chart-derived process-based indicators of high-quality EOL care in ICUs8,11,13 were selected to focus on communication with and psychosocial support for family members to facilitate informed EOL care decision making to limit potentially inappropriate LSTs. These indicators included documentation of physician–family prognostic communication, family meetings conducted, offer of palliative care consultations, social worker involvement, a DNR order issued at death, death without CPR, withdrawal of any LSTs, and family presence at death. 16
Data collection
Research assistants experienced in ICU care were trained to use specifications, developed by literature review8,11,13 and clinical expert consultation, to extract data for the chart-derived, process-based quality measures. Research assistants' concern about and misunderstanding of each item were clarified by discussions with the principal investigator to establish consensus. The well-trained research assistants used the revised specifications to assess each quality indicator by information documented in medical records at the patient level over the duration of ICU care. Inter-rater reliability for reviewed medical records was well established. 16
Family surrogates' satisfaction with EOL care quality was assessed by phone interviews with experienced research assistants in Mandarin or Taiwanese Hokkien in the first month after patient death, which has been shown as feasible and not too stressful.17,19,35 Phone calls were made during different periods over a week (e.g., morning and evening, different weekdays) if the first attempt failed to reach participants.
Statistical analysis
Each chart-derived, process-based quality indicator was analyzed using descriptive statistics. Results are presented as proportions of patients who experienced each quality indicator. To analyze associations between process-based quality indicators and family satisfaction with EOL care in ICUs, we used the generalized estimating equation method 36 with robust standard errors that account for correlation in the within-subject error term. To specifically examine the associations of process-based quality indicators and family's unique satisfaction levels with clinical care provided and the EOL care decision-making process, two separate models were fitted for the FS-ICU Care and FS-ICU Decision-Making scores with covariates of patient and family characteristics and length of ICU stay controlled. 31 Results are reported as β estimates and 95% confidence intervals (CIs).
Results
Participant characteristics
Among the 4454 patients admitted to the study ICUs during the period 2018–2019, 479 (10.8%) were eligible for participation (Fig. 1), and 326 patients (68.1%) who died during the same ICU stay as they were first enrolled constituted the final patient sample. Eligible patient participants were excluded primarily due to being discharged alive (n = 74, 48.4%) despite their high APACHE II score at screening or due to a family member's refusal to participate (n = 63, 41.2%) (Fig. 1). Among the 326 ICU decedents, 278 (85.3%) bereaved family members provided satisfaction data in the first month after patient death. Nonparticipation in bereavement surveys was primarily due to active refusal by bereaved family members (n = 21), followed by patient death within one month; thus, data collection was not due yet (n = 16). Participant and nonparticipant demographics did not differ (data not shown).
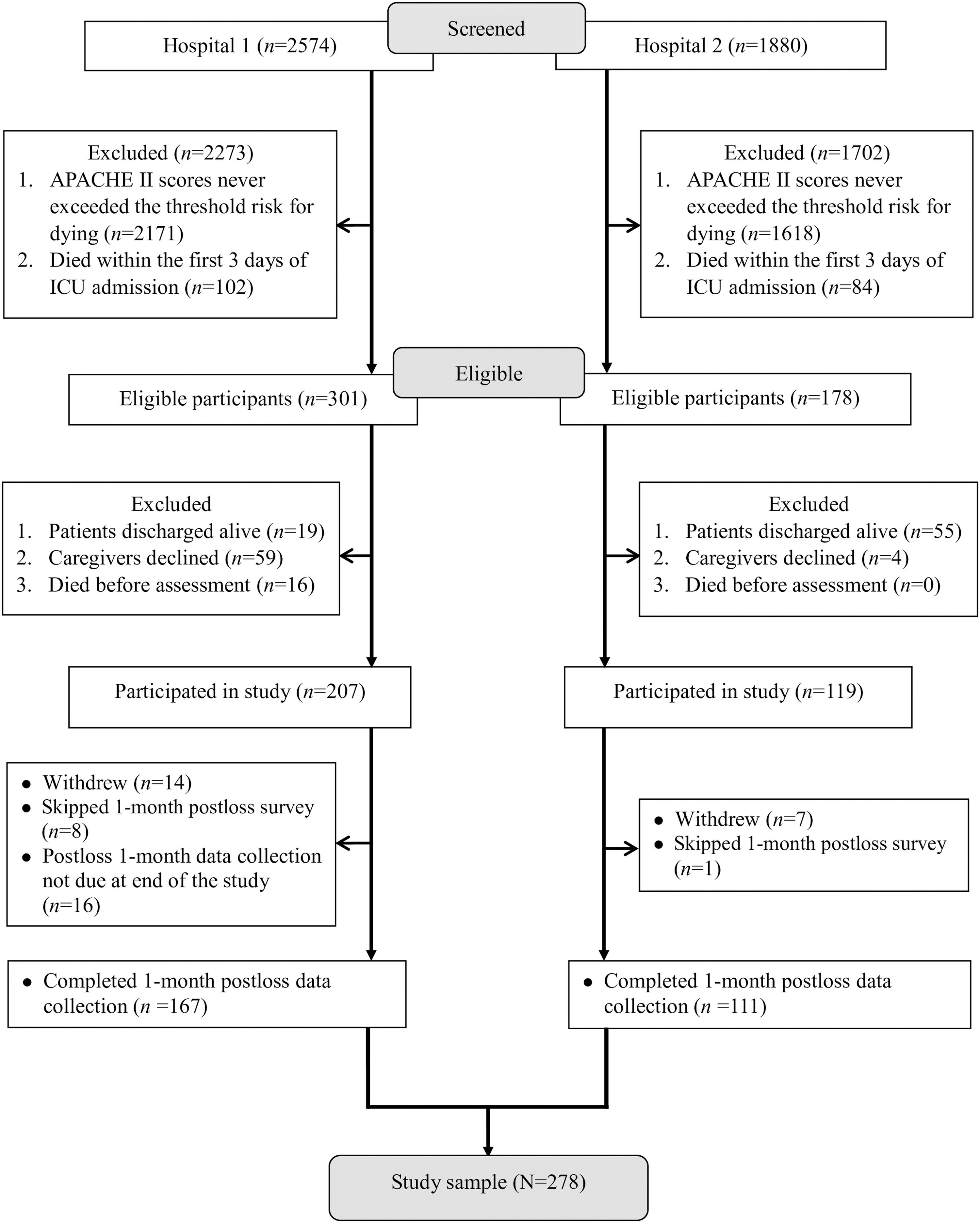
Case flow chart 1 month postloss.
Patient participants were mainly male (63.7%), their mean (standard deviation [SD]) age was 66.09 (14.01) years, their primary underlying disease was cancer (50.0%), and their primary attributable causes of ICU admission were respiratory failure/distress (51.3%), infection (28.2%), and shock (8.7%) (Table 1). Lengths of ICU stay and postenrollment survival were 21.37 (14.63) and 7.24 (8.00) days, respectively. Many family participants were female (59.0%), married (76.3%), the patient's adult child (53.6%), and living with the patient (64.8%) (Table 2). Family participants had a mean (SD) age of 49.78 (12.50) years.
Characteristics of Patient Participants (N = 278)
At ICU admission.
At enrollment.
APACHE, Acute Physiology and Chronic Health Evaluation; ICU, intensive care unit; SD, standard deviation; SOFA, Sequential Organ Failure Assessment.
Characteristics of Family Participants (N = 278)
Documentation of identified EOL care quality indicators for ICU decedents
Documentation of process-based indicators of essential high-quality EOL care for Taiwanese ICU decedents was high for physician communication of the patient's poor prognosis to family members (93.9%), provision of palliative care (71.6%), a DNR order in place at death (95.7%), and death without CPR (93.5%) (Table 3). However, documentation was infrequent for social worker involvement (9.7%) and interdisciplinary family meetings (23.0%). Furthermore, few (19.1%) patients had LSTs withdrawn, but the majority (80.9%) died with full life support and in the presence of a family member (75.2%).
Quality of End-Of-Life Care Identified in the Medical Records of Patients Who Died in Intensive Care Units (N = 278)
LSTs included intubation with mechanical ventilation support, vasopressors, hemodialysis, enteral and/or parenteral hydration and nutrition, antibiotics, and transfusion of blood products.
Without orders to withdraw any life support.
CPR, cardiopulmonary resuscitation; DNR, do-not-resuscitate; LSTs, life-sustaining treatments.
Associations between family satisfaction with EOL care and identified process-based indicators of high-quality EOL care in the ICU
The median (interquartile range [IQR] and mean [SD]) FS-ICU Care and FS-ICU Decision-Making scores were 70.83 (IQR: 58.33, 75.00, and 67.14 [16.59]) and 78.50 (IQR: 71.00, 83.50, and 76.12 [15.13]), respectively. Documentation of process-based indicators endorsed as essential high-quality EOL care was generally associated with higher scores for both FS-ICU domains (Table 4).
Associations between Quality of End-of-Life Care Identified in the Medical Records and Family Evaluation of End-of-Life Care in ICUs
Without experiencing the event as reference for each quality indicator.
Patient characteristics (gender, age, and disease severity [APACHE and SOFA scores]), family factors (gender, age, educational attainment, relationship with the patient, financial sufficiency, social support, anxiety symptoms, and depressive symptoms), and length of ICU stay were controlled in the multilevel linear regression models by the generalized estimating equation methods.
Bold indicates statistically significant.
LSTs included intubation with mechanical ventilation support, vasopressors, hemodialysis, enteral and/or parenteral hydration and nutrition, antibiotics, and transfusion of blood products.
CI, confidence interval.
Higher family satisfaction with ICU care was significantly associated with documentation of physician–family prognostic communication (β [95% CI]: 3.558 [2.963 to 4.154]), a DNR order issued at death (23.095 [17.410 to 28.779]), and death without CPR (13.325 [11.685 to 14.965]). Bereaved family members' satisfaction with decision making was positively associated with documentation of social worker involvement (4.767 [0.663 to 8.872]), a DNR order issued at death (10.499 [0.223 to 20.776]), and withdrawing LSTs before death (2.252 [1.834 to 2.670]).
Discussion
Taiwanese patients dying in ICUs received high-quality EOL care on physician–surrogate prognostic communication, provision of palliative care, dying with a DNR order, and death without CPR, but heavily used LSTs until death with infrequent documentation of social worker involvement and family meetings and less family satisfaction with care and decision making. Having a DNR order issued before patient death was associated with greater bereaved family members' satisfaction with care and decision making in ICUs. Documentation of physician–family prognostic communication, death without CPR, social worker involvement in EOL care, and withdrawal of LSTs were also positively associated with higher FS-ICU Care or FS-ICU Decision-Making scores.
Bereaved Taiwanese family members reported low satisfaction with decision making in the ICU (median [IQR]: 78.50 [71.00, 83.50], mean [SD]: 76.12 [15.13]), which is slightly lower or comparable with reported FS-ICU Decision-Making scores (median [IQR]: 80 [62.5, 92.5]–82.5 [70, 92.5], mean [SD]: 73–78.2 [18.2]),18,25,31,34,37 but substantially lower (median [IQR]: 70.83 [58.33, 75.00], mean [SD]: 67.14 [16.59]) than reported FS-ICU Care scores (median [IQR]: 88.5 [75, 96.4], mean [SD]:73.5 [19.4]–83 [16]).29,31,34,37
Our substantially lower observed satisfaction with EOL care in ICUs warrants further investigation since few cross-country and -cultural comparisons of FS-ICU scores have been conducted 38 especially with reports from Asian countries. However, variations of EOL care in ICUs have been well documented worldwide. 39 Furthermore, our observed lower satisfaction with care may be explained by participants' expectations of care in different health care contexts. 40
Having a DNR order issued before patient death was associated with greater family satisfaction with both care and decision making in ICUs. The only study on the association between DNR orders and family members' satisfaction with EOL care in ICUs showed an opposite result than ours. 29 However, this result 29 may be confounded by the fact that although family members signed a DNR order for their dying beloved, bereaved family members had significantly lower FS-ICU total scores than those of patients who survived in that study. 29
The Taiwanese government promotes DNR orders by legislation and by educating health care professionals to facilitate prognostic disclosure, promote EOL care discussions to explain the risks versus benefits of CPR/LSTs to family members, and respect patient/family wishes to forgo LSTs, thus letting patients die peacefully and avoid suffering. Indeed, a DNR order is associated with fewer potentially inappropriate LSTs for patients dying in ICUs, including CPR, invasive mechanical ventilation, and hemodialysis, but more palliative care. 41 Therefore, Taiwanese bereaved family members who signed a DNR order may perceive better ICU care for the patient, facilitating their EOL care decision making.
Our findings of positive associations between bereaved family satisfaction with ICU care and physician–family prognostic communication, 8 social worker involvement in EOL care, 8 death without CPR, 27 and withdrawal of LSTs before death25,27,28 are consistent with the literature. Specifically, under a strong influence of the Confucian doctrine of filial duty, 42 Taiwanese family members feel culturally obligated to use every possible means to keep their beloved alive. However, physician prognostic communication can meet family members' information needs to better understand their beloved's poor prognosis, thereby minimizing optimistic prognostic expectations about CPR 7 and letting patients die without CPR to avoid unnecessary suffering. Under these circumstances, bereaved family members may perceive the patient and themselves being treated appropriately, both physically and psychologically, to report higher satisfaction with ICU care.
Social worker involvement in EOL care may indicate offering psychological support and financial resources to help family members cope with the highly emotionally laden process of making appropriate EOL care decisions and deciding whether to withdraw LSTs before their beloved's death, possibly inducing bereaved family members to retrospectively evaluate ICU decision making as more satisfactory. However, social workers in Taiwan primarily play the role of seeking financial resources for patients who need a subsidy. Due to the coverage of health care expenditures by the National Health Insurance Program and strict criteria for applying for financial subsidy from social resources, documentation for social worker involvement was only shown for few participants (9.7%). Facilitating social worker involvement, especially for psychological support, is an actionable high-quality EOL care intervention to improve bereaved family members' satisfaction with ICU decision making.
Our study has several limitations. Participants were sampled from two hospitals in Taiwan, possibly limiting the representativeness of national and international target populations, especially for cultural differences in physician–family prognostic communication and family-dominant decision making for the dying patient. Our results cannot be generalized to patients who died within 3 days of ICU admission and their family members. Few bereaved family members withdrew from bereavement surveys, limiting the generalization of our findings to those family members. The FS-ICU is a subjective quality rating scale that assesses family satisfaction with care and the EOL decision-making process in ICUs, which may not fully reflect patient/family-centered experiences of ICU EOL care, and no clinically significant difference has been established for either the FS-ICU Care or FS-ICU Decision-Making subscale.
Our process-based measures focused on communication with and psychosocial support for family members to facilitate informed EOL care decision making and to limit inappropriate LSTs at the end of life. Our results cannot be generalized to other focuses of high-quality EOL care in ICUs. We recognized that some proposed process-based quality indicators of EOL care in ICUs may interact, but our study did not explore the underlying process of care for each identified, chart-derived, process-based quality indicator of EOL care, nor did it elucidate causal–effect relationships or the mechanisms by which quality indicators lead to family members' satisfaction with ICU care.
Our study may be underpowered to identify potential associations of bereaved family members' satisfaction with ICU care with provision of family meetings and with LSTs differentiated by extreme (e.g., mechanical ventilation support) and less (e.g., nutritional support and vasopressors) burdensome treatments due to low prevalence. We can never exclude the possible impact of unmeasured residuals, for example, family members' emotional preparedness for their beloved's forthcoming death, concordance between family members' preferred and actual decision-making roles, physician–family agreement on the appropriateness of EOL care decisions, and physician attitudes/practices toward respecting family preferences, commonly found in observational studies that may facilitate or diminish family satisfaction.
Conclusions and Clinical Implications
Our study showed that chart-derived process-based indicators of high-quality EOL care are positively associated with bereaved family's satisfaction with care provided in ICUs. We identified important opportunities for improving EOL care quality for critically ill patients and their families. Promoting physician–family prognostic communication to minimize optimistic prognostic expectations and providing psychosocial support to help family members cope with the highly emotionally laden processes of making an informed DNR decision to avoid CPR and continuing LSTs until death benefit not only the patient by avoiding unnecessary suffering but also may increase bereaved family members' satisfaction with the care provided to their beloved and their own decision-making process in ICUs.
Role of Sponsors
No funding sources had any role in designing and conducting the study; collecting, managing, analyzing, and interpreting the data; or preparing, reviewing, or approving the article.
Consent to Participate
Each patient's legal family surrogate signed informed consent for reviewing the patient's medical record and their own participation.
Consent for Publication
All authors have read the manuscript and consented for this article to be published by the Journal of Pain and Symptom Management.
Availability of Data and Material
Sharing of anonymized data from this study is restricted due to ethical and legal constrictions. The data contain sensitive personal health information, which is protected under the Personal Data Protection Act, thus making all data requests subject to Institutional Review Board (IRB) approval. As per the Chang Gung Memorial Hospital (CGMH) IRB, the data that support the findings of this study are restricted for transmission to those within the primary investigative team. Data sharing with investigators outside the team requires IRB approval. All requests for anonymized data will be reviewed by the research team and then submitted to the CGMH IRB for approval.
Footnotes
Authors' Contributions
The corresponding author (S.T.T.) takes responsibility for the content of the manuscript, has full access to all data in the study, and is responsible for the integrity of the data and accuracy of the data analysis, including and especially any adverse effects. W.C.C., C.C.H., T.H.H., L.P.C., M.C.C., and S.T.T. contributed substantially to the study conception and design. W.C.C., C.C.H., T.H.H., L.P.C., and M.C.C. contributed by providing study patients. W.C.C., C.C.H., T.H.H., L.P.C., M.C.C., and S.T.T. contributed to collection and/or assembly of data. W.C.C., C.C.H., T.H.H., L.P.C., M.C.C., and S.T.T. contributed to data analysis and interpretation. W.C.C., C.C.H., T.H.H., L.P.C., M.C.C., and S.T.T. contributed to the writing and final approval of the manuscript.
Funding Information
This study was funded by the National Health Research Institutes (NHRI-EX110-10704PI) with partial support from the Ministry of Science and Technology (MOST 108-2314-B-182-061-MY3) and Chang Gung Memorial Hospital (BMRP888).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.