
Abstract

Dear Editor:
Use of intrathecal medication is one of the options to manage oncological and nononcological refractory pain.1–3 Current recommendation is to position the catheter tip close to the pain generator to deliver medication.1,2 The classic technique describes implanting an intrathecal drug delivery device using the superior lamina of the interlaminar space in an oblique, cephalic, and medial position as a reference point, 4 which makes it difficult to locate the catheter tip in lumbar and sacral regions. Therefore, a different approach could be used to access the correct positioning of the catheter tip in these anatomical regions. We describe a technique to approach and locate a catheter in the lower lumbar space.
A 53-year-old male, with metastatic epithelioid sarcoma, presents severe neuropathic pain in the right lower limb, refractory to comprehensive pain management, therefore, multidisciplinary consensus agreed the patient would benefit from interventional management. He was currently treated with oral methadone 30 mg per day, intravenous patient-controlled analgesia (PCA) with 120 mg of morphine per day, and gabapentin 400 mg three times a day (TID) plus acetaminophen 1 g TID, with no adequate pain control.
He underwent a neurolytic procedure at the erector spinae plane muscle at an L2 level with a reduction of the visual analog scale by 50%. Nonetheless, there was an increase in pain due to rapid tumor progression. Therefore, the patient was considered candidate for intrathecal analgesia through retrograde subarachnoid catheter targeting L5–S1.
We describe the procedure as follows:
The L1–L2 level was selected and marked in a prone position using biplanar fluoroscopy. The needle was advanced toward the inferior contralateral lamina, using a medial caudal inclination. With the needle caudally directed, cerebrospinal fluid was obtained after passing the spinolaminar line (Fig. 1A). The catheter was directed to the L5–S1 target level. (Fig. 1B, C) A control myelogram confirmed adequate intrathecal contrast distribution. (Fig. 1D, E) Once the intrathecal location was assured, the patient was placed in a lateral decubitus position to create an abdominal pocket for the port. Catheters were protected with transparent dressing to assure a sterile state, the pocket was performed in a lateral position (Fig. 1F), using a conventional technique, and implantation of the port was successful.
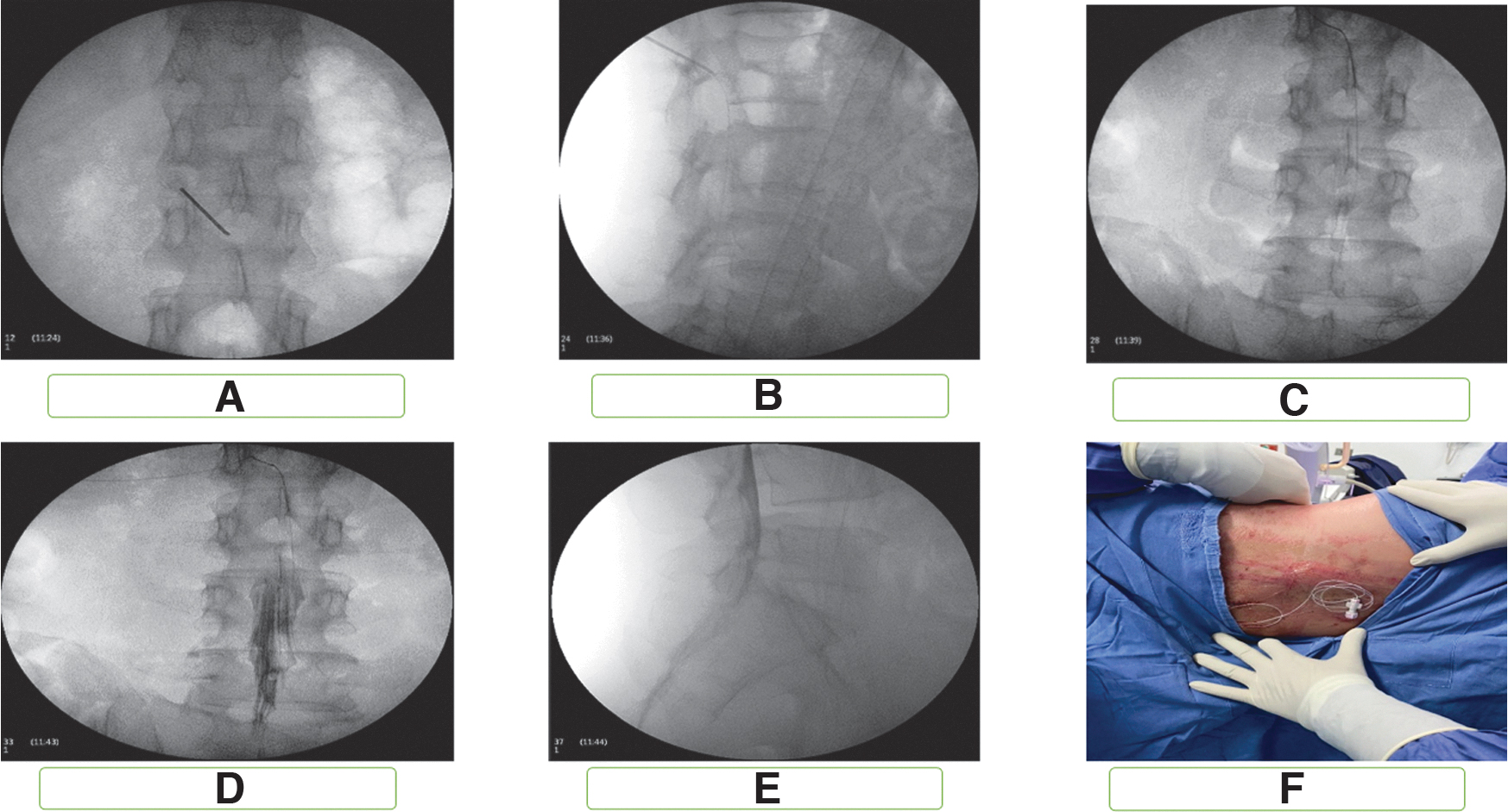
Implantation sequence of the intrathecal port through a retrograde approach.
Adequate pain control was archived. PCA morphine infusion and methadone were suspended, with posterior hospital discharge. This retrograde approach was replicated in three more patients.
A retrograde approach could be a valuable tool in patients with pelvic malignancies and refractory cancer pain. This technical vignette is easy to replicate and can be implemented as part of a comprehensive pain program.
Footnotes
Authors' Contributions
The authors declare that all authors included meet authorship criteria.