
Abstract
Introduction:
Code status discussions are poorly understood by patients and variably performed by admitting providers, yet they are used as a quality metric. Surgical specialties, such as Vascular Surgery, admit patients with urgent and life-threatening illness. Surgical trainees are less likely to receive communication skills interventions when compared with nonsurgical specialties. Without a documented code status, nurses and physicians lack guidance on patient preference in the case of cardiopulmonary arrest and may deliver unwanted measures, which may also result in poor outcomes.
Methods:
We conducted a before–after Plan–Do–Study–Act quality improvement project between May 2018 and May 2019. A needs assessment included baseline code status documentation rates for the Vascular Surgery department admissions. A communication skills training (CST) and documentation intervention was provided to all Vascular Surgery trainees and advance practice providers (APPs). Departmental e-mails were sent over the 12-month intervention period, which demonstrated the code status documentation rates and served as reminders to document code status.
Results:
A total of 29 vascular surgery trainees and APPs received the intervention. At completion of the intervention, learners reported increased comfort initiating a code status discussion, making a recommendation for cardiopulmonary resuscitation (CPR) status, and having a strategy to discuss code status. A total of 2762 patient admissions were reviewed, with 1562 patient admissions occurring during the 12-month intervention period. The average code status documentation rate for the three months before the intervention was 7.8%. At the end of the 12-month intervention, documentation rates were 44.9% and 6 months after completion of the study period, average rates remained 45.2%. There was no change in admission rates during the study period.
Discussion:
CST and regular reminders increased vascular surgery residents' and APPs' comfort in engaging in code status discussions. After intervention, documentation of code status discussions increased with persistence up to six months after the intervention.
Introduction
Code status discussions are nuanced conversations, which encompass uncertainty, prognosis, and discussion of possible morbidity and mortality.1–7 In academic medical centers, trainees and advance practice providers (APPs) perform them as part of inpatient admissions. However, trainees and APPs may not feel confident or comfortable to discuss code status,1,6,8 resulting in low rates of completion. In situations where patients do not have a code status documented and experience a cardiopulmonary arrest, there may be confusion among the care team as to how to proceed. The default code status of “Full Code” or “CPR Yes” leads to initiation of CPR on patients who clinicians fear will not survive or may not have chosen CPR.
In review of our electronic health record (EHR) data, we found that surgical specialties have much lower rates of code status documentation when compared with nonsurgical specialties. Additional studies confirm that code status documentation occurs less frequently on admission to surgical services compared with medical services.9–11
In 2015, a patient at our institution had an unexpected cardiopulmonary arrest without a documented code status. The patient received advanced cardiac life support and survived with significant disability. The patient told their family and the care team they had not desired resuscitation and their current quality of life was unacceptable causing significant distress for the patient, family, and care team. We identified the Division of Vascular Surgery department as having high acuity patients and low code status documentation rates. We therefore developed a quality improvement project to improve code status documentation for a patient admitted to the Vascular Surgery service.
Methods
Context
Code status documentation is a quality metric used in many hospital systems. We noted there was a lack of code status documentation in the electronic medical records for patients admitted to the Vascular Surgery service at their four clinical institutions within the University of Pittsburgh Medical Center Health System, a quaternary hospital. Chart review demonstrated <10% code status documentation rate for patients admitted to a Vascular Surgery service during our needs assessment.
Intervention
After review of EHR data, we discussed barriers, facilitators, and areas for improvement related to code status documentation with Vascular Surgery service stakeholders. A yearlong educational initiative was formed to improve code status documentation (Fig. 1). This quality improvement project was approved through the University of Pittsburgh Medical Center Quality Improvement (UPMC QI) Review Committee. The primary outcome evaluated was improvement in code status conversation documentation rates.
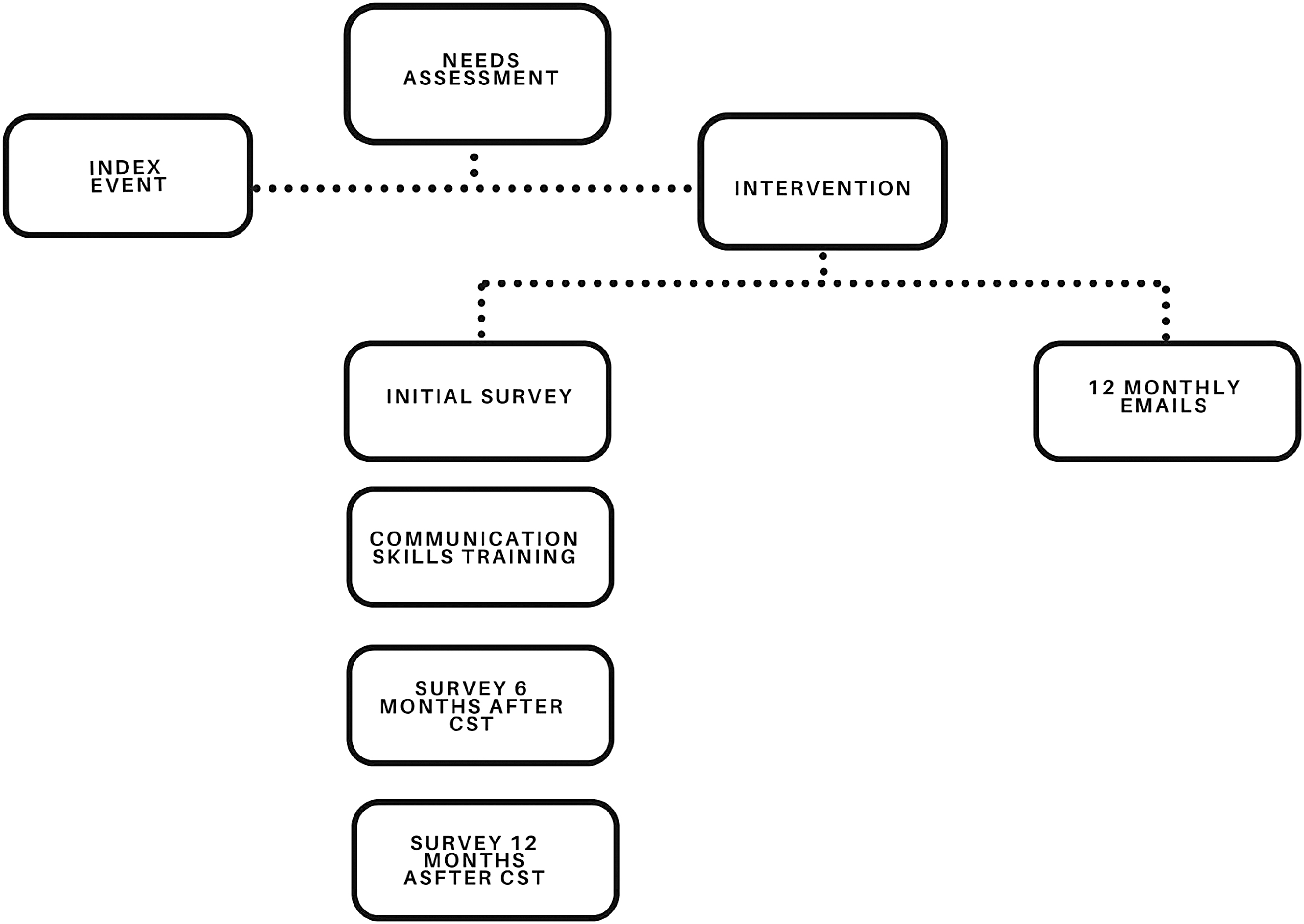
Study design. The study design included a communication skills intervention, which marked the beginning of the 12-month intervention period. Data were collected throughout the 12-month study period regarding patient demographics. Learners were reminded and encouraged to continue documenting code status through monthly e-mails.
We performed a pretest–posttest Plan–Do–Study–Act quality improvement study evaluating code status documentation rates and perceptions within the Division of Vascular Surgery at the University of Pittsburgh Medical Center between May 2018 and May 2019. This quality improvement project was performed as a collaboration between members of the Cardiology Department and the Division of Vascular Surgery. This comprised an initial survey of the learners evaluating their perceptions and comfort with code status conversations using a 5-point Likert Scale. Following this survey, a communication skills training (CST) for 29 learners was provided (Table 1). Follow-up surveys assessing learners' perceptions and comfort with code status conversations were conducted at the mid-point of the intervention (6 months) and the end of the project (month 12).
Vascular Surgery Learner Demographics
A total of 29 learners received the training.
APP, advance practice provider; PGY, postgraduate year.
The CST was facilitated by palliative care clinicians who had undergone training as communication skills educators. The first hour of the training consisted of a didactic session discussing the importance of code status discussions, outcomes of cardiopulmonary resuscitation, impact on patients and families, a conversation framework, and how to document code status in the electronic medical record. The “CPR” conversation framework was presented during the didactics (Fig. 2).

CPR Framework. “CPR” Framework used to guide code status discussions. CPR, cardiopulmonary resuscitation.
The second hour of the training involved drills and practice in small groups. The facilitator used a drill sheet and handouts addressing the different code status outcomes. Finally, the learners performed role play with the facilitators using three scripted scenarios. The role play reinforced the “CPR” framework and allowed for immediate feedback to the learners.
After the CST, we sent monthly e-mails to the Vascular Surgery physicians (attendings and trainees) and APPs reminding them to document code status and providing data regarding their code status documentation rates. Additional feedback was provided during departmental meetings to reinforce code status documentation, especially if documentation numbers were noticed to be decreasing at a site.
Measures
Electronic anonymous surveys of learners were performed at three time points: immediately before the training session, six months after the CST, and at the end of the yearlong intervention period. These surveys were evaluated for change in perception and comfort related to code status discussions (available on request). Those who completed the final survey received a $15 gift card.
Code status documentation rates were obtained monthly for 3 months preintervention, the 12 months of the intervention, and for 6 months postintervention. Patient demographics, length of stay, and admitting diagnoses were obtained through reports generated by the EHR (Table 2). We evaluated variation in CPR documentation rates based on sex, age, and length of stay.
Patient Demographics
Preintervention refers to the three months before the CST. Intervention is the 12-month intervention following the training inclusive of the regular e-mails. Postintervention refers to the following six months. Admission diagnosis information was obtained and then categorized. p-Values were calculated using ANOVA and Chi-squared statistic.
Missing data.
ANOVA, analysis of variance; CST, communication skills training.
Analysis
Descriptive statistics were obtained of both learner data and patient demographics and presented as frequency and percentage. Categorical variables were compared using analysis of variance, Fisher's exact test, and Chi-squared test for the parametric data, as appropriate. For nonparametric data, Kruskal–Wallis test was used. Statistical analysis was performed using Stata SE 16 (version 16.1; College Station, TX).
Results
A total of 29 learners were identified to participate in this intervention. All 29 learners, of which 18 were Vascular Surgery trainees and 11 were APPs, received the CST in May 2018. Half of the Vascular Surgery trainees and 10 APPs were female (Table 1). The preintervention survey had a 55% completion rate, the six-month survey 38%, and postintervention survey 69% (Table 3).
Learner Survey Results
A total of 16 trainees completed the initial survey and 20 trainees filled out the final survey evaluating their perception and comfort with having code status conversations. Responses were on a 5-point Likert Scale. p-Values were calculated with the use of Kruskal–Wallis test for nonparametric data.
Missing values.
ACLS, advanced cardiac life support; CPR, cardiopulmonary resuscitation.
In this initial survey, 43.8% learners reported they had previous CST related to code status or goals of care. Attitudes toward having the conversation were positive with 81.3% reporting they felt code status should be documented for all patients. A much lower number, 43.8%, felt comfortable making a recommendation regarding code status (Table 3).
Six months after the CST, learners were more comfortable making CPR status recommendations, which increased to 75% at the time of the final survey. There also was an increase in self-perceived documentation rates from 6.25% initially, to 45% on survey administered immediately after the study period (Table 3).
A total of 2762 patient admissions were evaluated during the 21-month study period, (360 preintervention, 1562 patient admissions during the 12-month intervention period, and 840 postintervention). In the intervention group, 882 (56.9%) were male, and 782 (50.1%) were over the age of 70 years. The most common admission diagnoses were peripheral vascular disease, admission related to hemodialysis access, or limb ischemia (Table 2). Length of hospital stay was less than three days for 49.7% of the patients. The frequency of admissions did not change throughout the hospital stay (p = 0.836). There was a slight increase in peripheral vascular disease as an admitting diagnosis (p = 0.016); an increase in patients 30–40 and 50–69 years of age (p = 0.0001, p = 0.0001, respectively) and a statistically significant difference in length of stay less than three days (p = 0.004). Otherwise, patient demographics, gender, age, admitting diagnoses, and length of stay were not statistically different between the preintervention, intervention, and postintervention groups.
Average code status documentation rates for the three months before the study period was 7.8% with 1.7% being “CPR No” (Fig. 3). Code status documentation rates increased to 44.9% with 3.3% being listed as “CPR No” at the completion of the yearlong intervention period (decreased to 3.1% in the six months following) (Table 4). Patients who were older or with hospital stays less than three days were less likely to have a code status documented throughout the intervention period (Table 5). Six months after the end of the yearlong intervention and e-mail reminders were no longer sent, and documentation rates remained 45.2% (Fig. 3).

Code status documentation rates. Comparison of code status documentation by quarter. Preintervention refers to the baseline code status documentation rates for the three months before the CST. Documented code status includes “CPR Yes,” “CPR No,” and “CMO.”
Code Status Documentation Rates
Data during the 12-month intervention was evaluated in 3-month quarters. The CST was performed during the middle of May 2019; therefore, the data from May were excluded. p-Value were calculated using the Chi-squared statistic.
CMO, comfort measures only.
Code Status Documentation by Patient Characteristic
Code status documentation improved after the CST. Code status documentation for the variables such as gender and age did not differ significantly. There was an increase in code status documentation based on length of hospital stay.
p-Values were obtained using ANOVA.
Discussion
This CST and monthly e-mail code status documentation intervention is effective in improving code status documentation rates in a Vascular Surgery service. Similar interventions have been done within Internal Medicine and nonsurgical specialties with improved code status documentation rates, but none has been done for Vascular Surgery.1,12–22 In our quality improvement initiative, Vascular Surgery trainees and APPs increased their code status documentation and demonstrated behavioral change, resulting in increased rates of code status documentation. The behavior change continued for six months after the intervention stopped, suggesting culture change.
The patient populations and admitting diagnoses in our preintervention, intervention, and postintervention analysis are similar to other Vascular Surgery programs.23–26 In a study by Hutul et al., only 36% of surgical trainees were comfortable discussing DNR orders. 27 Other studies evaluating code status documentation rates note that surgical specialties are less likely to have code status documented, especially discussions regarding end of life.28,29 Furthermore, surgical specialties are less likely to have CST.30,31 Many studies have demonstrated improvement in trainees' comfort and self-efficacy with communication related to code status or end of life through communication skills interventions.12,31,32 Our study suggests change is possible with communication training and feedback.
During our intervention, we hoped to achieve a 70% code status documentation rate. While we did not achieve this benchmark, we were able to improve code status documentation rates sixfold. Surgical service code status documentation rates were not as high as Internal Medicine and nonsurgical subspecialities at our institution, which average around 90%. Unique to some surgical training programs is the overnight and cross-coverage by other surgical services, such as general surgery or orthopedics. At our institution, overnight and weekend admissions may be admitted by nonvascular surgical trainees who did not receive the CST, which might have resulted in lower-than-expected rates of admission code status discussion documentation.
The study had several limitations. First, the study was done at one institution with a strong Palliative Care program, a strong communication education program, in addition to Vascular Surgery leadership who supported this quality improvement program. Whether the interventions would be possible at other institutions with other palliative care programs is unclear. The small number of enrolled learners and the variable number of responses on the surveys limited the statistical analysis. While there was an overall improvement of the code status documentation, change in individual practice patterns and the quality of documentation of the code status conversation in the EHR was not evaluated.
Conclusion
This study demonstrates CST is effective in improving code status documentation rates in Vascular Surgery. Future directions for improving code status discussions and documentation may include longitudinal CST courses, especially at the beginning of academic years and a broader integration of this training, so that all providers develop the skills and comfort with code status discussions, thus resulting in an institutional culture change. Obtaining the code status documentation rate by program managers for departmental distribution can provide helpful feedback. Furthermore, measures such as direct observation of code status discussions and chart analysis for description of the code status discussion provides opportunities for direct feedback.
Footnotes
Authors' Contributions
A.B.T., J.E.L., K.M.S., J.K.W., and R.M.A. developed, designed, collected, and/or analyzed the data. All authors revised the article. All coauthors have reviewed and approved of the article before submission. All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in the Journal of Palliative Medicine.
Acknowledgments
The authors would like to thank the Division of Vascular Surgery at the University of Pittsburgh Medical Center for their administrative support. They would like to thank Ahmet Sezer for his biostatistical support.
Funding Information
This work was supported by the ACGME Back to Bedside Initiative.
Author Disclosure Statement
R.M.A. serves as an editor for AAHPM PC FACS and is a Palliative Care editor for UpToDate. He also serves as a board member for VitalTalk. M.S.M. serves on the advisory board of Gore and Medtronic. He has no conflict of interest. The remaining authors have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this article.